Article Text

Abstract
Background and purpose: Dissections and dissecting aneurysms involving the basilar artery (BA) are rare lesions with a poor prognosis, and controversies exist on treatment strategy. We describe the clinical presentation, radiologic features, and clinical outcomes of 11 consecutive patients with these lesions, treated using stent alone placement.
Materials and methods 11 patients were studied (10 men, one woman), with a mean age of 51 years (range 30–68 years). Clinical and angiographic data were reviewed retrospectively.
Results It was technically feasible to place stents in all 11 cases, and a multiple stents technique was used in nine patients. Procedure related posterior circulation ischemic complications occurred in two cases. One patient presenting with locked-in syndrome died of a pulmonary embolism 3 months after treatment although the clinical condition was gradually improving after stent placement. In the other eight cases, improvement in initial symptoms or a stable condition was observed on follow-up at 1–48 months. Angiographic follow-up was obtained in nine cases using DSA (n=8) or CT angiography (n=1). Successful occlusion of the aneurysm or dissection sac was noted in two cases, BA occlusion in one case, disappearance of double lumen sign in one case, and delayed retention of contrast medium in one case. For the remaining four patients there was no change in the configuration of the lesions on follow-up angiographic results.
Conclusions Stent alone treatment as a potential and disputable alternative therapeutic option for the treatment of BA dissection and dissecting aneurysms, although technically feasible, was effective in only certain lesions, and this treatment carries substantial risks of complications and a high failure rate. The true effect of this strategy is questionable. A study involving larger populations and a longer follow-up is necessary to evaluate the efficacy of this treatment modality.
- Aneurysm
- Angioplasty
- Dissection
- Stent
Statistics from Altmetric.com
Introduction
Dissections and dissecting aneurysms involving the basilar artery (BA) are rare lesions with a poor prognosis, and controversies exist as to the proper management of these lesions, which most commonly present with subarachnoid hemorrhage or posterior circulation ischemic stroke, and sometimes a mass effect due to brainstem compression.1–4 Although conservative management has been advocated by some authors,1 ,3 selected cases might require positive surgical or endovascular treatment, especially when they are ruptured or present with progressive ischemic or mass effect symptoms. Because of the morphological characteristics of these lesions and complicated anatomical structures in the posterior cranial fossa, surgical treatment is usually difficult.5 ,6 Hence endovascular treatment has gradually become an important alternative therapeutic option to manage these lesions.7–12
Endovascular BA occlusion for these lesions, which may be life threatening as a result of severe ischemic complications unless sufficient collateral is present through the posterior communicating arteries, is rather limited compared with lesions of the vertebral artery (VA). Recently, with the improvement in modern endovascular techniques and materials, reconstructive therapy using stents for vertebrobasilar dissection and dissecting aneurysms has been increasingly reported.9–14 However, to the best of our knowledge, the literatures regarding stent alone treatment (SAT) for dissection and dissecting aneurysms involving the BA are sparse, and relevant case series reports are rare.7 ,12 ,14 Here we present our experience using a stent alone technique for the treatment of 11 consecutive patients with these types of lesions, describing the clinical presentation, angiographic features, and clinical outcome.
Materials and methods
Patients
Between December 2008 and December 2012, 11 consecutive patients diagnosed with dissection or dissecting aneurysms of the BA were treated using a stent alone placement technique in our department. There were 10 men and one woman, with a mean age of 51 years (range 30–68 years). The clinical and imaging characteristics of these 11 patients are presented in table 1. Clinical presentation was posterior circulation ischemic stroke in case Nos 2, 3, 4, 5, 8, 9, and 11, mass effect on the brainstem in case Nos 1, 6, and 11, agnogenic headache in case No 7, and in case No 10, the aneurysm was an incidental finding on CT angiography performed for unrelated symptoms.
Clinical and imaging characteristics of 11 patients with dissection or dissecting aneurysm involving the basilar artery
Preoperative radiologic evaluation
Every patient underwent preoperative planar image examination, including CT scanning or MRI, or both. Before the treatment procedure, all patients underwent DSA to confirm the diagnosis and angiographic characteristics and to assist in treatment planning. Diagnosis was based on clinical manifestations and findings of radiological examinations, including CT, MRI, and CT/MR/cerebral angiography. Intramural thrombus on T1 weighted images (case Nos 1, 2, 3, 5, 6, 7, and 10) and intimal flaps on T2 weighted images (case Nos 1, 4, 6, 9, and 11) were major findings indicating dissection. Demonstration of these lesions on cerebral angiography included typical results such as double lumen (case Nos 2, 5, 8, and 9), tapered narrowing (case No 1), pearl-string sign (case No 7), or retention of contrast medium in the aneurysmal or dissection sac (case Nos 1, 3, 4, 6, and 8).
Endovascular treatment and techniques
All patients received dual antiplatelet therapy, including 100 mg of aspirin and 75 mg of clopidogrel from at least 3 days prior to the procedures. Dual antiplatelet therapy was maintained for 2 months postoperatively followed by aspirin monotherapy lasting indefinitely for cases presenting with ischemic stroke; in the other cases, aspirin monotherapy lasted for 6 months.
All procedures were performed with the patient under general anesthesia. Anticoagulation during the treatment process included an IV bolus of 3000–5000 IU of heparin given at the beginning of each procedure and 1000 IU bolus administered intravenously thereafter every hour. Every coaxial catheter flushing fluid was mixed with heparin at a concentration of 1000 IU of heparin per liter of saline.
In all cases, vascular access to the BA for stent placement was obtained via a transfemoral approach using a 6 F guiding catheter. Diagnostic angiography and three-dimensional rotational angiography were performed through a single or bilateral VA contrast injection. Following the diagnostic angiogram, the guiding catheter was navigated into VA, usually the preponderant one. The stents used in this case series included the Solitaire AB (eV3), Enterprise (Codman Cordis), Neuroform (Boston Scientific), Wingspan (Boston Scientific), and Leo (Balt). The choice of stent was dependent on anatomic geometry, size, and length of the aneurysmal lumen, and the availability of the devices. Using the roadmapping technique, a microcatheter (Rebar 027, eV3; Prowler Select Plus, Codman Cordis) or specialized delivery system (Vasco, Balt; Wingspan, Boston Scientific) was coaxially, using a microguidewire (Silverspeed 14, eV3; Traxcess-14, Microvention; Transcend-14, Boston Scientific), navigated through the guiding catheter into the BA to cover the lesion. In some cases, a single stent was not sufficient to remodel the blood flow sufficiently or completely cover the entire length of the lesion, so subsequent overlapping stents or cascading stents were deployed. Basilar dissection may develop via antegrade progression of unilateral or bilateral VA dissections. In this case, the proximal stent should cover the lesion of the VAs. In lesions involving bilateral VAs, after deploying stents into the BA and unilateral VA, the guiding catheter should be transferred to the contralateral VA to deploy the stent through the mesh of the stent placed at the vertebrobasilar junction to cover the lesion at this side. After stent deployment, control angiography was performed to confirm the patency of the parent artery and evaluate intra-aneurysmal hemodynamic changes.
Follow-up protocol
Patient followup was performed clinically and with angiography examination, preferably DSA. Clinical outcomes were evaluated according to modified Rankin Scale (mRS).
Results
It was technically feasible to place stents in all 11 cases. A multiple stents technique were used in nine cases (case Nos 2, 3, 4, 5, 6, 7, 8, 9, and 11), and the true overlapping stents technique was used in five (case Nos 2, 5, 6, 9, and 11). In the remaining four cases (case Nos 3, 4, 7, and 11), multiple stents deployed in tandem or in a partial overlapping fashion were used to completely cover the long lesions involving the distal unilateral VA (case Nos 4 and 11) or bilateral VAs (case Nos 3 and 7).
Immediately after stent angioplasty, control angiography was performed to evaluate postprocedural hemodynamic changes in all 11 cases. More retention of contrast medium was observed in the aneurysmal or dissection sac in three cases (case Nos 1, 6, and 8; 27.3%). In case No 4, improvement in blood flow in the parent artery and bilateral posterior cerebral arteries was e observed after stenting. In another seven cases (63.6%) there was no obvious hemodynamic change immediately after stenting. Angiographic follow-up was obtained in nine cases. In case No 1, follow-up DSA obtained 6 months after treatment revealed delayed occlusion of the BA after stenting and the aneurysm had also disappeared. This patient did not present with any symptoms related to the occluded BA because the hypertrophied bilateral posterior communicating artery supplied the distal BA and its branches sufficiently. In case Nos 6 and 8, follow-up DSA obtained 6 months after treatment confirmed delayed thrombosis of the dissection or aneurysmal sac with patency of the BA. In case Nos 3, 9, and 11, there was no obvious change on follow-up DSA compared with the angiogram performed immediately after stent placement during the procedure. Follow-up DSA 5 month later revealed disappearance of the double lumen sign in case No 2. In case No 7, follow-up DSA 8 months later showed delayed retention of contrast medium in the dissection sac. In case No 10, CT angiography follow-up obtained 2 months after treatment confirmed that the morphology and size of the aneurysm was stable, and there was good patency of the BA. Follow-up angiography was unavailable for case Nos 4 and 5.
Complications after treatment occurred in three patients (27.3%). Case No 4, who was bed-ridden because of locked-in syndrome before SAT, unfortunately died of a pulmonary embolism 3 months later although the clinical condition had been gradually improving after treatment. Ischemic complications were encountered immediately after treatment in case Nos 5 and 10. Case No 5 presented with right hemiparesis, left facial paralysis, and vertigo, and CT scanning confirmed pontine infarction. Case No 10 presented with left hemiparesis after treatment, and CT scanning discovered pontine and cerebellar infarction in this patient. No other complication was observed prior to patient discharge and during follow-up.
Clinical followup was performed in all 11 patients. Case No 6, who presented with right clonic facial spasm, improved gradually, and this symptom had disappeared when he was admitted for DSA followup 6 months after treatment. Symptoms in case Nos 1, 2, 8, and 9 were improved during followup; in case Nos 3, 7, and 11, their condition was unchanged compared with their baseline condition. Although the condition of two patients presenting with ischemic complications were gradually improving during follow-up, both still suffer from moderate disability (case No 5, mRS score=4; case 10, mRS score=3). Clinical and angiographic outcomes are summarized in table 2. Representative cases are provided in figures 1⇓–3.
Clinical and angiographic outcomes
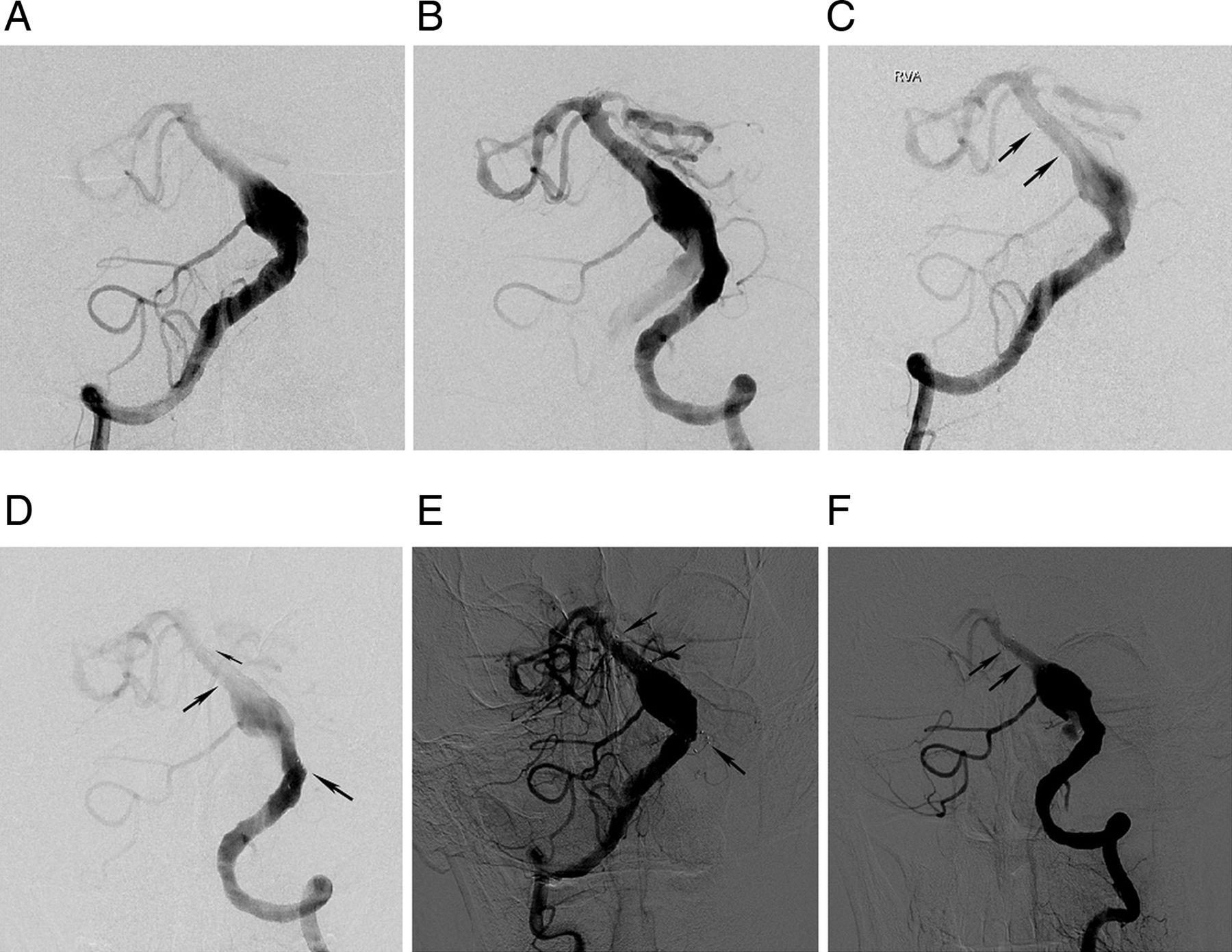
A quadragenarian presenting with blurred vision for 2 months (case No 3). (A, B) Bilateral vertebral angiograms, frontal view, show a fusiform basilar trunk aneurysm involving the right anterior inferior cerebellar artery and distal segments of the bilateral vertebral arteries. Note the irregular distal vertebral arteries and right posterior inferior cerebellar artery originate from the aneurysm. (C, D) Bilateral control vertebral angiograms performed immediately after stenting during the procedure. No obvious change in retention was observed after stenting. Follow-up DSA obtained 11 months later shows there is still no hemodynamic changes and no newly formed thrombosis in the aneurysm sac (E, F). Arrows in (C–F) show stent markers. The condition of this patient was unchanged compared with baseline after treatment (modified Rankin Scale score=2).

A tricenarian presenting with locked-in syndrome (case No 4). T2 weighted MRI (A) and conventional preoperative DSA (C) demonstrate a serpentine dissection involving the basilar trunk and distal segment of the left vertebral artery. (B) MRI shows extensive diffusion weighted imaging infarct burden. (D) Unsubtracted angiogram after placement of four partially overlapping stents. Note markers of the stents (D, arrows). (E, F) Control angiography after stenting. After stenting, improvement in blood flow in the perforators and bilateral posterior cerebral arteries was observed. The clinical condition of the patient gradually improved after treatment. Unfortunately, this patient died of a pulmonary embolism 3 months later and follow-up angiography was not available.
{kind=link}
{kind=link}
{kind=link}
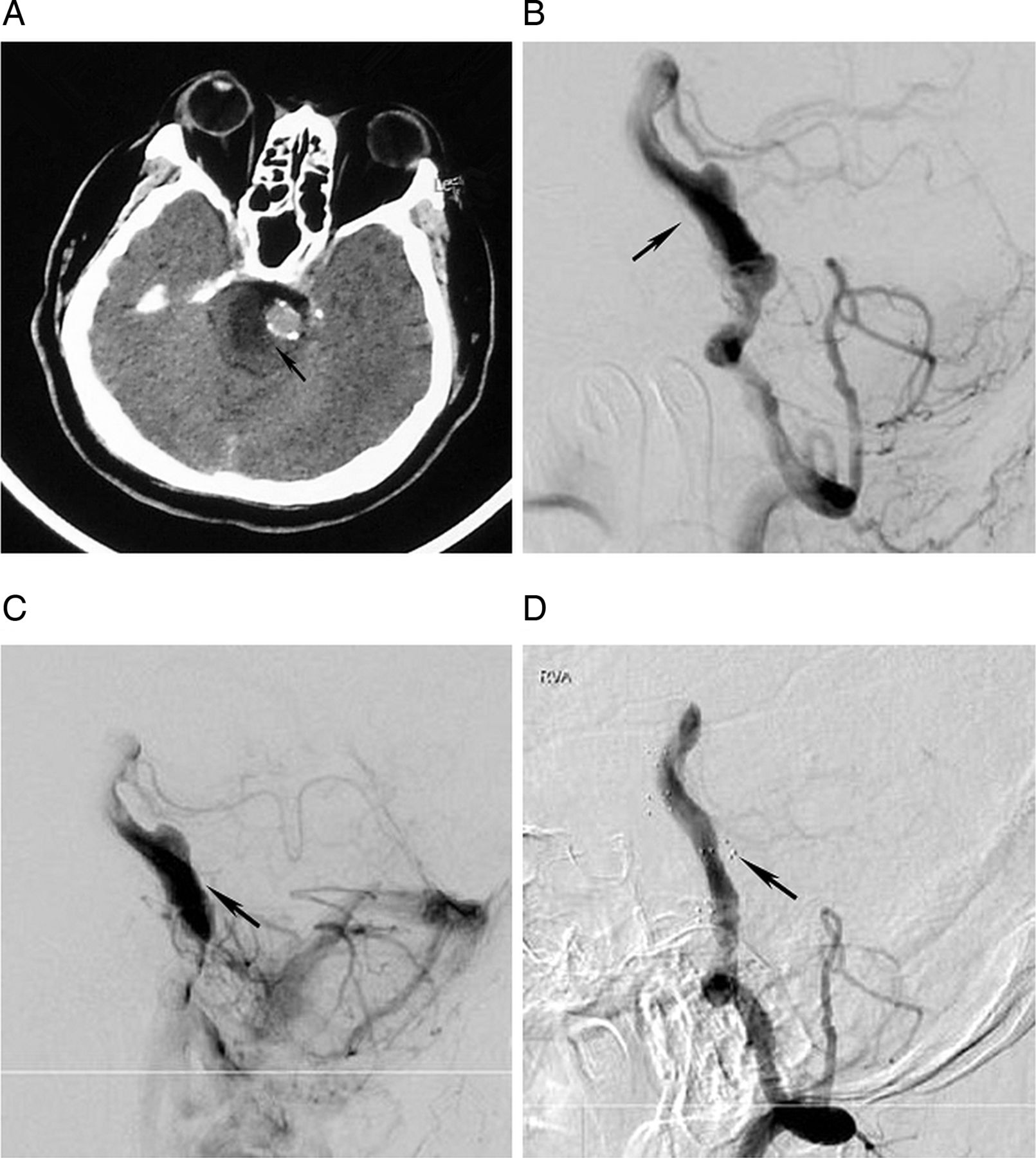
A quadragenarian presenting with sudden vertigo, followed by unconsciousness, alalia, and quadriplegia (case No 8). (A, B) CT and right vertebral angiogram in the lateral view demonstrates dissection of the entire basilar artery, resulting in brainstem infarction (A, B, arrows). (C) Lateral view of the right vertebral angiogram after stent placement demonstrates obvious retention of contrast media in the dissection sac (arrow). (D) Follow-up DSA obtained 6 months later confirmed delayed thrombosis of the dissection sac (arrow). The presenting symptoms in this case were gradually improved after treatment. However, this patient is still dependent in daily life (modified Rankin Scale score=3).
Discussion
Advances in angiography and MRI have led to increased recognition that posterior circulation cranial vessel dissections and dissecting aneurysms are a noteworthy cause of stroke.2 ,9 ,12–17 Dissections and dissecting aneurysms involving the BA have been reported much less frequently compared with those involving the VA. Currently, reconstructive endovascular treatment with stents has been used as an important therapeutic option for dissections and dissecting aneurysms involving the BA. However, apart from a few anecdotal cases,7 ,9 ,12 ,14 case series reports on using SAT for the management of these lesions have rarely been described. In this study, we have presented our experience using SAT for these lesions.
Patient selection
Reconstructive strategies utilizing stents for the treatment of intracranial dissecting aneurysms and dissections consist of stent assisted coiling (SAC) and SAT. Both methods promote thrombosis of the aneurysm while preserving or even improving blood flow in the parent vessel. In most circumstances, SAC is preferential because coiling decreases blood flow impingement into the fragile vessel wall of the lesion and further reduces wall stress of the pseudoaneurysm, which is beneficial for thrombosis within the aneurysmal or dissection sac, thereby facilitating long term healing of the lesions and decreasing the possibility of bleeding compared with SAT.18 However, dissecting aneurysms of the basilar trunk may be fusiform or dolichoectatic, which often involve the whole circumference of the BA and lack a defined neck. On the other hand, some of these lesions involve vital perforating branches, the occlusion of which can have a catastrophic outcome. Therefore, sometimes SAC is not feasible for these lesions due to the morphological features because the coils may protrude into the parent artery or nearby large perforators, thus resulting in ischemic complications.
Conservative management using anticoagulation and antiplatelet therapy for these lesions presenting with ischemic stroke has been advocated by some authors. However, conservative management has been followed by disappointing results in some patients.1 ,11 For patients presenting with progressive ischemic symptoms despite adequate conservative treatment or brainstem mass effect, SAT is a potential alternative therapeutic option to heal the lesions or improve blood flow in the parent vessel and thus prevent infarct progression.
Reports suggest that stent struts play a role in diminishing intra-aneurysmal blood flow and promote thrombosis in the aneurysmal sac.19 ,20 It is still not known whether placement of a stent alone can effectively prevent rupture of aneurysms, especially for ruptured ones. Although we cannot confirm that SAT cannot effectively prevent rebleeding, we would suggest that using SAT for the management of hemorrhagic lesions requires great caution considering the high rebleed rate after SAT reported by some authors.10 ,11
In conclusion, SAT for the management of these lesions should be tailored to individual patients after giving cautious consideration to the clinical manifestations and angiogram results. In this series, there were seven patients presenting with recurrent progressive ischemic stroke (case Nos 2, 3, 4, 5, 8, 9, and 11) and three patients with progressive mass effect (case Nos 1, 6, and 11). Case No 7 presented with progressive headache within the previous 1 month before SAT, which was considered a sign of progression of the lesion. SAT was performed with the aim of preventing progression of the lesions in these cases. The remaining case No 10, who was incidentally diagnosed and clinically asymptomatic, developed severe depression after knowing the diagnosis and the potential risks, and strongly requested procedural intervention. Unfortunately, ischemic complications occurred. Hence we feel that the lesson we have learnt from this case is that treatment for such lesions should considered as a last resort only in instances where patients present with subarachnoid hemorrhage, progressive ischemic complications, mass effect, etc. The use of invasive interventions for such lesions needs cautious consideration, especially for those lesions that are asymptomatic.
Theoretical mechanism
There are theoretical and experimental data supporting the use of the SAT technique for the management of these lesions. Firstly, computational fluid dynamic and other experimental studies elucidated that stents alter blood flow within the aneurysmal or dissection sac and decrease blood flow impingement on the fragile wall by providing a mechanical hindrance to the inflow patterns, and postulated that sufficient flow remodeling and hemodynamic stress reduction within the aneurysm after placement of the stent would create favorable conditions for thrombus formation.19 ,20 Secondly, stents serve as a scaffold for subsequent neoendothelialization of the aneurysm neck or the injured parent vessel, consequently facilitating long term healing of the lesions.21–23 The inherent pathology of dissecting aneurysms and dissections may also account for their susceptibility to SAT. The deployed stent could tag down the intimal leaflet which is the inflow route of the dissection pseudolumen and support or repair the intimal flap of these lesions, thereby further reducing inflow to promote thrombosis. A previous report of real time observation of intimal collapse after stent placement via intravascular ultrasonography could explain this effect.24
Dissections and dissecting aneurysms involving the BA can cause ischemic symptoms or stroke as a result of stenosis or occlusion of the parent vessel, or by vital perforating or circumflex vessels. For these patients, SAT is a potential treatment option which may assist with ischemic stroke, as verified in previous reports.7 ,11 ,12 For patients presenting with ischemic symptoms caused by luminal narrowing and flow restriction of the parent vessel, SAT can improve blood flow in the parent vessel and thus prevent ischemic stroke. For patients presenting with progressive perforator ischemic symptoms, how SAT assists with these patients is not known because the pathophysiology of these lesion is not clearly defined. We postulate that SAT could prevent progression of these lesions and remodel blood flow in the parent artery, thus facilitating improvement in blood flow in the perforators to assists with progressive perforator ischemic symptoms.
Stent type and techniques
As mentioned above, flow remodeling and repair of the intimal flap are two important reasons for using SAT to manage dissecting lesions. Porosity is the key factor in creating hemodynamic changes.20 The stronger radial force of the stent is advantageous for tagging down of the intimal leaflet in these lesions. Thus the mesh design is strongly correlated with efficacy of SAT. The advantage of a balloon expanding stent with respect to porosity and radial force is clear. However, these stents are relatively inflexible and difficult to advance into the tortuous intracranial vasculature. Also they may exert a traumatic radial force in fragile vasculature during deployment, with risks of chronic reactive intimal proliferation or acute vessel injury, especially when inflating balloons across a freshly ruptured lesions. Therefore, we prefer the self-expandable nitinol intracranial stents to the balloon mounted coronary stents, not only because they are easier to navigate but also they exert a lower radial force against the fragile dissection wall, thereby avoiding the dangers associated with balloon inflation. To achieve a lower porosity, we prefer using a thick stent, the diameter of which is larger than the parent vessel, to provide relatively stronger radial force and less porosity. In order to induce neoendothelialization, we use bare metal stents rather than drug eluting stents. This is why 4.5 mm Enterprise and 6 mm Solitaire stents were so frequently used in this case series.
The overlapping stent in stent technique is based on the premise of a less porous mesh causing greater intra-aneurysmal hemodynamic changes, and also providing relatively stronger radial force. In addition, many basilar dissections and dissecting aneurysms are too long to be completely covered with only one stent, and complete coverage of lesions with stent is ideal when using SAT because we could not judge the location of the torn intimal leaflet in these lesion. In our series, the true overlapping stent in stent technique was used in five of the 11 cases. This small number of cases cannot definitively clarify whether the overlapping stent technique is superior to the single stent technique in producing favorable remodeling; however, as advocated by some authors,12 ,25 this technique may be useful in cases of remodeling failure with single stent treatment.
Treatment result and complications
Currently, appropriate treatment of basilar dissection and dissecting aneurysms is very challenging and there is no satisfactory management to obtain ideal result for these lesions.1 ,2 ,6 ,9–11 Only certain lesions responded to SAT and benefitted from this treatment in this series. For other cases, there was no change in the configuration of the lesions or hemodynamic remodeling in the control angiography during the procedure or even in the follow-up angiography. We found that there was contrast media retention in the preoperative angiogram in all three patients who had technical treatment success, which may be an indicator for using SAT. We postulate that contrast media retention may mean the existence of a torn intima, and blood flow through this defect into the pseudoaneurysm may have been responsible for contrast media retention. Contrast media retention may disappear with spontaneous healing of the torn intima which act as the inflow route of the dissection pseudolumen. So the effect of SAT for lesions without contrast media retention may be limited, because these lesions are often relatively stable. However, not all the lesions showing contrast media retention responded to SAT. In this series, no change in the configuration of the lesions was observed on follow-up angiogram in two cases presenting with postprocedural contrast media retention. From this small series, we cannot definitely explain why certain lesions responded to treatment while others did not. A study involving a larger population and longer follow-up is necessary to clarify this issue and evaluate the efficacy of this treatment modality.
SAT for these lesions carries a substantial risk of complications. Ischemic complications after treatment occurred in two patients. Previous reports indicated that levels of P2Y12, a platelet membrane protein receptor which plays a key role in platelet activation, vary in individuals and influence the effect of antiplatelet therapy.26 ,27 To reduce ischemic complications for these patients receiving reconstructive endovascular treatment, P2Y12 platelet function tests, to evaluate if there is P2Y12 resistance to antiplatelet therapy, and coagulogram tests, such as thrombelastography to monitor blood coagulation, may be helpful.27 Unsatisfactory results of thrombelastography could prompt a change in the anticoagulation and antiplatelet strategy to obtain a better effect.
There are many other issues to clarify for this treatment modality. Improvement or stable condition of initial symptoms was observed in eight cases, apart from those who encountered complications. However, was the improvement in initial symptoms in the above cases caused by stenting or the antiplatelet therapy after SAT, or was it a natural course of the disease? For example, although comparison of preprocedural and postprocedural angiograms could confirm whether SAT remodelled blood flow and improved perfusion of the brainstem perforators and bilateral posterior cerebral arteries in case No 4 (who suffered from locked-in syndrome resulting from spiral dissections of the BA), it is not clear whether this treatment had anything to do with the gradual clinical improvement. In most of these cases, follow-up time was short. Does SAT improve the prognosis of patients with basilar dissections and dissecting aneurysms in the long-term? Only certain lesions responded to SAT. Are there lessons to be leant in terms of patient selection, stent selection, and use of a single stent or overlapping stent in stent technique that may impact on the treatment result? If a flow diverter is available for treating these lesions using SAT, what is the result? Could SAT effectively prevent rebleed of ruptured lesions? A study with a larger population and longer follow-up is necessary for validation of the efficacy of this treatment modality.
Conclusions
SAT as a potential and disputable alternative therapeutic option for the treatment of BA dissections and dissecting aneurysms. Although technically feasible, SAT is effective in only certain lesions and carries a substantial risk of complications and a high failure rate. The true effect of this strategy is questionable. A study involving a larger population and longer follow-up is necessary to evaluate the efficacy of this treatment modality.
References
Footnotes
-
Contributors CL: collecting the data, and drafting and revising the article. YL, CJ, ZW, and YW: substantial contributions to conception and design, revising the article, and analysis and interpretation of the data. XY: conception and design, revising the article, and final approval of the version to be published.
-
Funding This work was supported by the National Science Foundation of China (grant Nos 81220108007 and 81171079), National ‘Twelfth Five-Year’ Plan for Science and Technology Support (grant No 2011BAI08B06), High-Level Health Technique Talent Training Plan of Beijing Health System (grant No 2009-3-22), and National 973 Basic Research Program of China (grant No 2010CB732605).
-
Competing interests None.
-
Ethics approval The study was approved by the ethics committee of Beijing Tiantan Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.