Article Text

Abstract
Introduction/purpose The efficacy of endovascular stroke treatment is highly time-dependent. Thus optimizing systems of care to deliver appropriate treatment as swiftly as possible is a key goal of stroke care providers. We aim to analyze timeliness of treatment in a large endovascular cohort by assessing 1) real-world time metrics of care delivery, 2) specific causes of delays to treatment, and 3) time lost due to interhospital transfer.
Materials and methods The STRATIS registry is a prospective, multicenter study of patients with large vessel occlusion (LVO) treated with the Solitaire Stentriever within 8 hours of onset. Subjects were separated by direct presentation (direct group) vs. interhospital transfer to the enrollling hospital (transfer group), and further characterized by the use of IV tPA (IVT) or mechanical thrombectomy alone (MT). Total alarm-to-revascularization time measured overall performance of the system of care. We also calculated a hypothetical ‘bypass’ scenario by comparing the door-to-tPA times for the two groups and adding the transfer time to the direct group for an extremely conservative estimate of additional travel time.
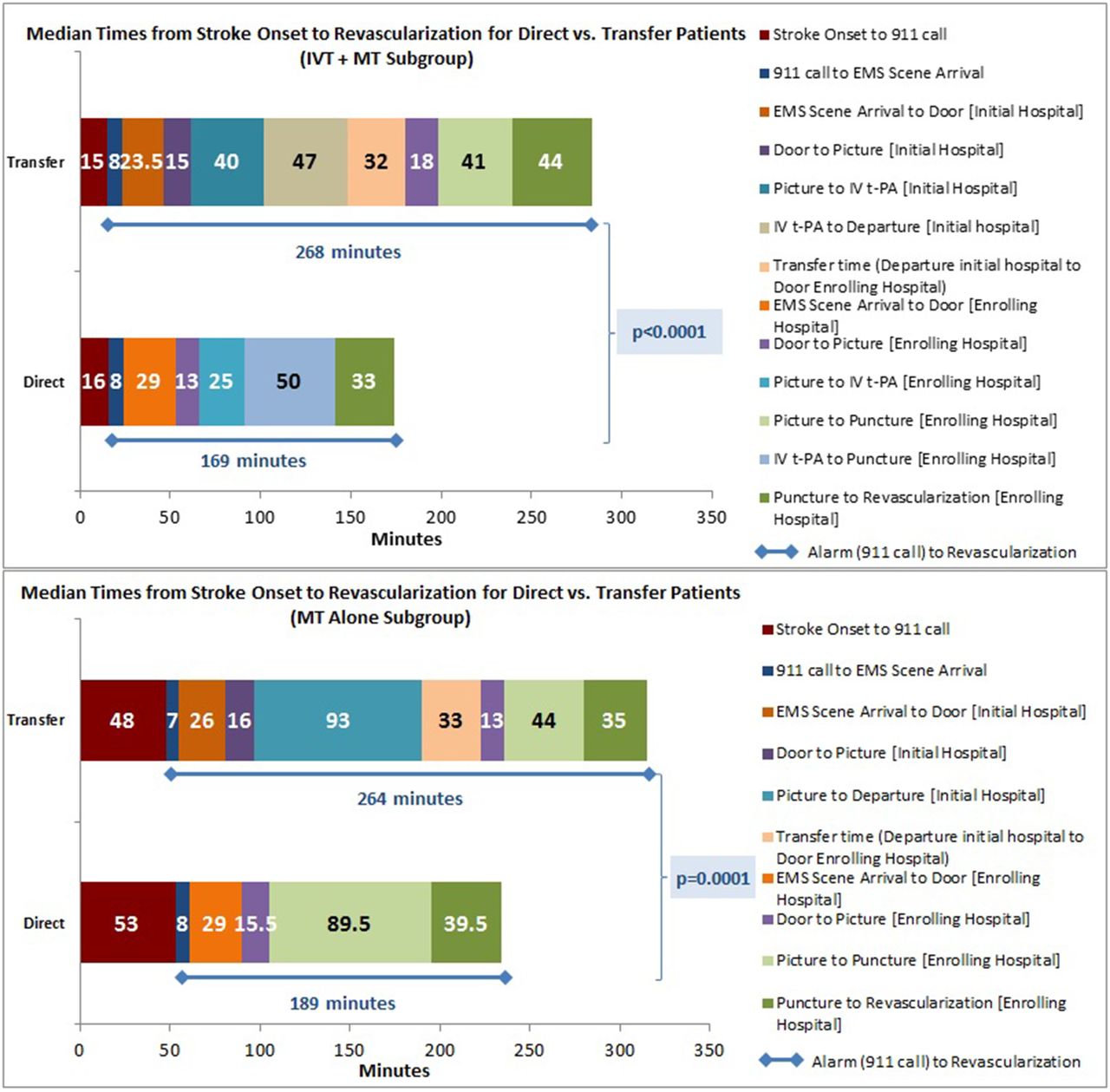
Results A total of 688 subjects were analyzed. Median times from stroke onset to revascularization for direct vs. transfer patients in the MT-alone subgroup were 238.5 and 325.0 minutes respectively, and in the IVT plus MT were 192.0 and 305.5 minutes respectively (Figure 1). Median alarm-to-revascularization times for direct vs. transfer patients in the MT subgroup were 189 and 264 minutes respectively (75 minute difference; p = 0.0001), and in IVT were 169 and 268 respectively (99 minute difference; p < 0.0001). These differences were accounted for by imaging-to-transfer time, which was 93 minutes for MT-alone and 87 minutes for IVT. Median door-to-tPA times were 56.5 minutes at regional hospitals and 38.0 minutes at enrollling sites (p < 0.0001). Transfer time was 32.0 minutes, making the hypothetical bypass time-to-tPA 70.0 minutes.

{kind=link}
Conclusion Time to revascularization is much slower for patients requiring interhospital transfer. The delay is accounted for by the time between imaging and departure, which is when treatment decisions and transfer arrangements are made, and should be a target for improvement.
An important consideration for many regional systems is whether certain stroke patients should bypass the nearest hospital to go directly to an endovascular center. We created a conservative model of such a scenario, which suggests that successful revascularization would be achieved 99 minutes earlier by bypass. This may have significant implications for regional stroke systems of care.
Disclosures M. Froehler: 2; C; Medtronic Neurovascular. 6; C; Site PI (Large, Liberty, SCENT, Feat, Barrel, Atlas, Rhapsody, Positive, Sep 3D) payment to institution. M. Aziz-Sultan: 2; C; Medtronic Neurovascular. 6; C; Expert Witness - BMC. R. Jahan: 1; C; Medtronic Neurovascular. 2; C; Medtronic Neurovascular. R. Klucznik: 3; C; Medtronic Neurovascular. J. Saver: 2; C; Medtronic Neurovascular, Stryker, Neuravia, Cognition Medical, Boehringer Ingelheim (prevention only). O. Zaidat: 2; C; Medtronic Neurovascular. D. Yavagal: 2; C; Medtronic Neurovascular. 6; C; ESCAPE trial DSCMB member. N. Mueller-Kronast: 2; C; Medtronic Neurovascular.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/