Article Text

Abstract
Background Early identification and transfer of patients with acute stroke to a primary or comprehensive stroke center results in favorable outcomes.
Objective To describe implementation and results of an emergency medical service (EMS)-driven stroke protocol in Lucas County, Ohio.
Method All county EMS personnel (N=464) underwent training in the Rapid Arterial oCclusion Evaluation (RACE) score. The RACE Alert (RA) protocol, whereby patients with stroke and a RACE score ≥5 were taken to a facility that offered advanced therapy, was implemented in July 2015. During the 6-month study period, 109 RAs were activated. Time efficiencies, diagnostic accuracy, and mechanical thrombectomy (MT) outcomes were compared with standard ‘stroke-alert’ (N=142) patients from the preceding 6 months.
Results An increased treatment rate (25.6% vs 12.6%, p<0.05) and improved time efficiency (median door-to-CT 10 vs 28 min, p<0.05; door-to-needle 46 vs 75 min, p<0.05) of IV tissue plasminogen activator within the RA cohort was achieved. The rate of MT (20.1% vs 7.7%, p=0.06) increased and treatment times improved, including median arrival-to-puncture (68 vs 128 min, p=0.04) and arrival-to-recanalization times (101 vs 205 min, p=0.001) in favor of the RA cohort. A non-significant trend towards improved outcome (50% vs 36.4%, p=0.3) in the RA cohort was noted. The RA protocol also showed improved diagnostic specificity for ischemic stroke (52.3% vs 30.1%, p<0.05).
Conclusions Our results indicate that EMS adaptation of the RA protocol within Lucas County is feasible and effective for early triage and treatment of patients with stroke. Using this protocol, we can significantly improve treatment times for both systemic thrombolysis and MT.
- Stroke
- Standards
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Mechanical thrombectomy (MT) was recently established as the standard treatment for eligible patients with acute stroke and emergent large vessel occlusion in the anterior circulation.1 The positive effect of this treatment is time dependent with a more likely chance of achieving a favorable outcome in patients who have early recanalization.2 ,3 To incorporate these recent findings into clinical practice, experts recommended improving stroke systems of care to increase timely and equitable access to this therapy.4 Over the past year, several major medical centers have attempted to streamline regional systems of care for early stroke recognition and transfer of patients with severe stroke to facilities that offer advanced therapy.5 Although it is recommended that patients with stroke should be transported to the closest primary or comprehensive stroke center,6 there is no standard clinical criterion for this process. On-site evaluation by the emergency medical service (EMS) squad using the Rapid Arterial oCclusion Evaluation (RACE) scale was validated as a simple prehospital tool that can accurately assess stroke severity and identify patients with acute stroke due to large vessel occlusion.7 Using this strategy, we reorganized our EMS stroke triage protocol in Lucas County in northwest Ohio to improve timely access to patients who might benefit from MT. In this study, we describe the implementation of this protocol and report the initial 6 months' results and outcomes.
Methods
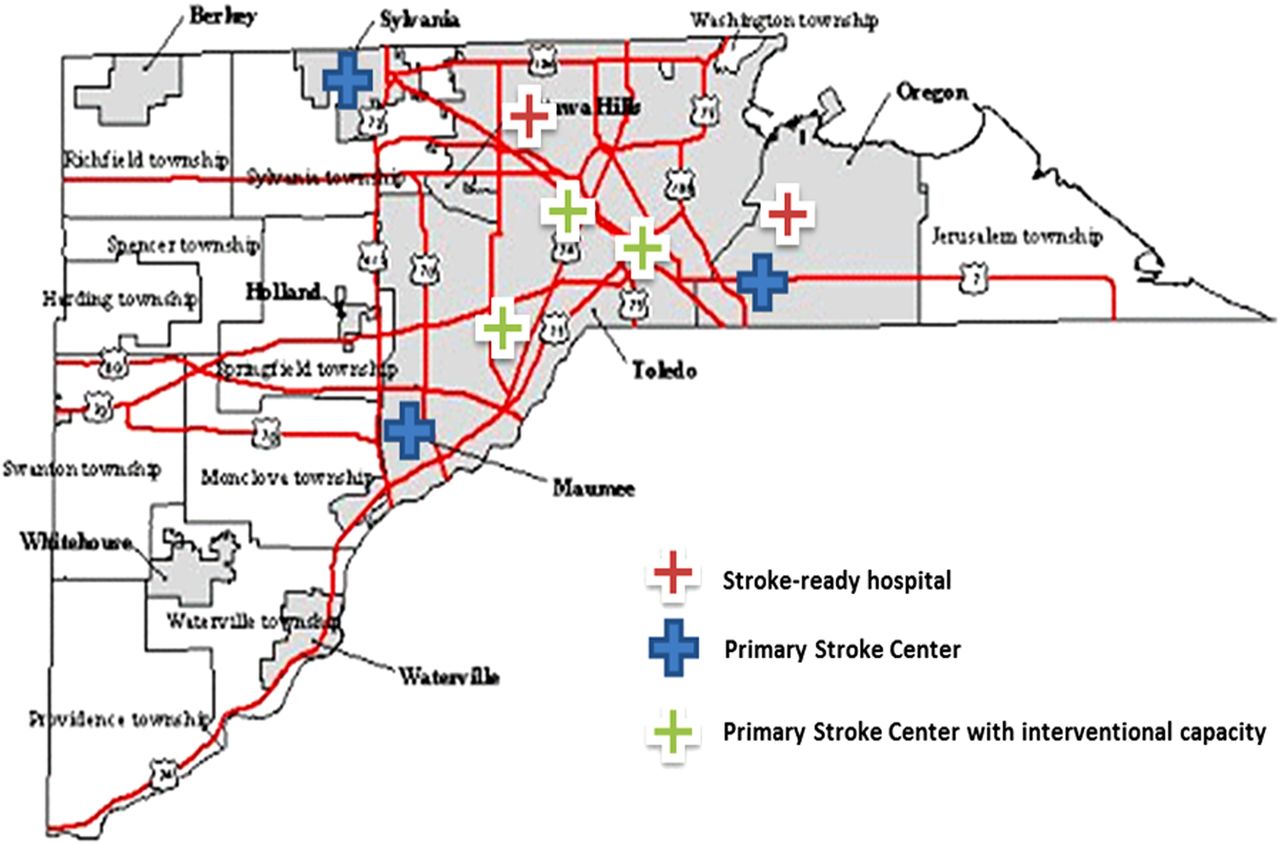
Located in northwest Ohio, Lucas County is spread over 596 square miles and has an estimated population of 436 393. The county has eight hospitals, of which six centers have Joint Commission primary stroke center (PSC) designation (figure 1). Three of these hospitals have additional interventional capacity (PSC-IC). Of the three hospitals with PSC-IC in the Lucas County, our stroke team operates at two facilities: University of Toledo Medical Center and Promedica Toledo Hospital. Thus, we report our findings and outcomes of patients presenting at these two centers.

Lucas County stroke centers.
EMS training
Lucas County EMS leadership formed a local prehospital stroke care committee to design and monitor the educational content of a stroke training module. Over 10 individual sessions, vascular neurologists provided comprehensive training and materials using the approved stroke training module to all 464 Lucas County EMS paramedic personnel. The training material included a 2-hour lecture on acute stroke syndromes, stroke mimics, and prehospital management. This was followed by a 2-hour interactive session with video demonstration of the RACE score and hands-on RACE scale assessment using mock patients.
The RACE Alert (RA) protocol was implemented in Lucas County on July 1, 2015. The protocol is outlined in figure 2. After potential stroke identification using the Cincinnati Stroke Scale, EMS personnel conduct the RACE scale assessment. All patients who are last seen normal within 12 hours or wake up with stroke symptoms or have an undetermined timeline of stroke symptoms, and who also meet a RACE scale threshold ≥5 are emergently transferred as RA patients to the nearest hospital with PSC-IC, bypassing closer emergency centers, if any.
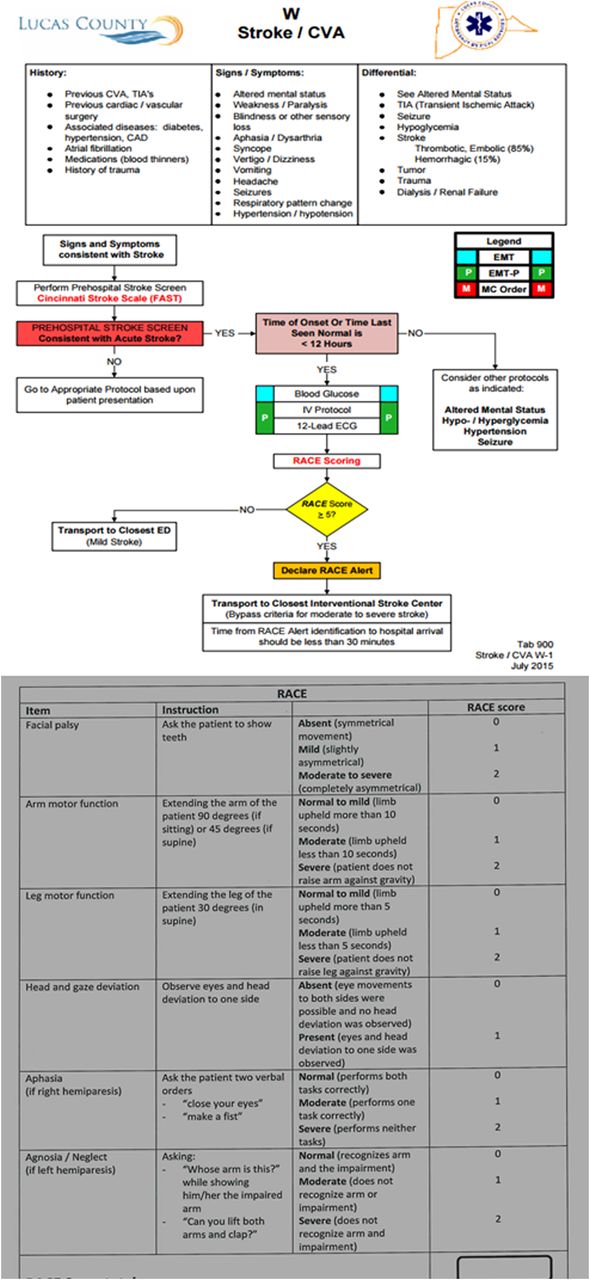
Lucas County Rapid Arterial oCclusion Evaluation (RACE) Alert protocol. CAD, coronary artery disease; CVA, cerebrovascular accident; ED, emergency department.
Emergency center protocols
We also established emergency room (ER) protocols for patients presenting as RA (figure 3). Our processes include pre-arrival notification by the EMS personnel with time last known well, expected time to the ER, and RACE score. This notification is sent as an RA page to the vascular and interventional neurologists on call, stroke nurse, ER, neuro intensive care unit (ICU), pharmacy, laboratory, and radiology departments. Patients are preregistered with a unique ID in the electronic medical record system. After a brief assessment by the ER physician, patients are rapidly moved to the radiology department for head CT scan and CT angiography of the neck and head. The stroke nurse accompanies the patient to the scanner. We cancel CT angiography if an ischemic stroke is ruled out by the time the CT head is completed.

{kind=link}
{kind=link}
{kind=link}
Emergency room protocol. ED, emergency department; EMS, emergency medical service; NIHSS, National Institutes of Health Stroke Scale; PT/INR, prothrombin time/international normalized ratio; RACE, Rapid Arterial oCclusion Evaluation; RN, registered nurse.
Data collection
We obtained institutional review board approval to maintain a prospective registry of all stroke alert (SA) and RA patients. Data include demographics, vascular risk factors, RACE score, National Institutes of Health Stroke Scale (NIHSS) score, diagnosis, treatments/procedures, and clinical and radiographic outcomes. A NIHSS certified neuro ICU nurse (stroke nurse) determines the NIHSS score on presentation. The neurointerventionalist determines the baseline Alberta Stroke Program Early CT Score (ASPECT) and post-thrombectomy Thrombolysis in Cerebral Infarction (TICI) recanalization grade. Clinical outcomes are assessed using the modified Rankin Scale (mRS) score obtained by a mRS certified investigator at the 90 days' clinic follow-up appointment. For patients who cannot come to the clinic, we assess the mRS score by a phone interview. Favorable clinical outcome is defined as a mRS score of ≤2.
The control group consisted of SA patients brought directly to PSC-IC ER in the 6 months before RA protocol activation— that is, January 1 through June 30, 2015. According to our previous protocol, the ER team activated ‘SA’ for patients with suspected stroke who had a NIHSS score >3 and who were last known well within the past 12 hours. To ensure adequate comparison, only patients transferred by the Lucas County EMS squad were included in the analysis. We excluded from the control group, patients with stroke transferred from outlying facilities, arriving at the ER by private transportation, or developing stroke while hospitalized. The control group for MT consisted of SA patients who presented directly to our PSC-IC centers and patients who were transported by Lucas County EMS squads to other county ERs before they were transferred to our PSC-IC centers for thrombectomy.
Statistical analysis
Statistical analysis was performed using Stata 11 (StataCorp LP, College Stanton, Texas, USA). The aim of this analysis was to assess the operation of RA protocol and to compare the time efficiencies and clinical outcomes of the RA and SA cohorts. Mann–Whitney or t-tests were used for comparison of continuous variables and χ2 or Fisher exact tests for categorical variables. We evaluated the correlation between NIHSS scores and RACE scales using a non-parametric Spearman coefficient.
Results
Demographics
During the 6-month study period from July 1 through December 31, 2015, there were 293 Lucas County life squad stroke transports and 135 RACE alerts. Of these, 109 RAs were brought to our two PSC-IC ERs. In the preceding 6 months, between January 1 and June 30, 142 SAs were activated in our two PSC-IC ERs and were included in this analysis.
Baseline patient demographics are outlined in table 1. Compared with the control group, the RA patients were older (72.5 vs 65 years, p=0.02) with higher median NIHSS score (12 vs 5, p<0.05) on presentation. The median 911 activation time to arrival was 31 min in the RA group.
Baseline demographics, diagnosis, and treatment times
IV thrombolysis
Among the RA cohort, 28 (25.7%) patients received IV tissue plasminogen activator (tPA) while 18 (12.7%) of the SA patients were treated with IV tPA (p<0.05). The median time (in minutes) from door to CT scan was 10 (IQR 5–16) for the RA patients and 28 (IQR 20–41) for the control group (p<0.05). For patients receiving IV tPA, the median door to needle time was 46 (IQR 28–55) in the RA arm as compared with 75 (IQR 60–95) for the SA patients (p<0.05).
Mechanical thrombectomy
In 2015, we performed 85 thrombectomies at the two PSC-IC ERs. We identified for analysis 11 subjects meeting MT control criteria during the first half of 2015, and 22 RA subjects during the latter half of the year. Five of the 11 patients in the MT control group were transferred from other Lucas County ERs.
Among RACE patients who underwent MT (table 1), we found that median time (in minutes) from ER arrival to groin puncture (68 (IQR 60–93) vs 128 (IQR 101–142), p=0.04) and time to recanalization (101 (IQR 88–118) vs 205 (IQR 131–218), p<0.05) were significantly faster than for SA patients (figure 3). No statistically significant difference was found in the rate of successful recanalization (TICI 2b/3 recanalization 86.4% vs 81.2%, p=0.7) or favorable clinical outcome (50% vs 36.4%, p=0.3).
The RA thrombectomy cohort showed a strong correlation between presentation NIHSS score and RACE scores (Spearman's r 0.69, p<0.05).
Hospital course
The RA patients were more likely than the SA patients to have a discharge diagnosis of acute ischemic stroke (52.3% vs 31%, p<0.05). Other diagnoses in the RA cohort included intracranial bleeding (N=12, 11%) and seizures (N=19, 17.4%). Rapid symptom resolution was noted in 7 (6.4%) patients who were diagnosed as having transient ischemic attacks. Of patients presenting as RA, 68 (62.4%) required admission to the ICU.
Discussion
Owing to the significant implications of a protocol that recommends bypassing stroke-ready hospitals or primary stroke centers, it is imperative that it is well studied in the community it will affect.
Our results indicate that in northwest Ohio Lucas County, EMS adaptation of the RACE protocol is a feasible and highly effective tool for early in-field assessment and bypass/transfer decision for patients with acute stroke symptoms. It resulted in shorter door-to-needle time in patients who received IV tPA, shorter door-to-recanalization time, and a trend towards improved clinical outcome and decreased mortality in patients who underwent MT.
A strong correlation was found between the RACE score obtained by the EMS and the NIHSS score obtained in the emergency department in the MT group (Spearman's r 0.69, p<0.05). No major adverse effects of this diversion were reported during the study period and the median dispatch to arrival time remained within the recommended time limit.6 EMS personnel were instructed to go to the closest hospital if there was a safety concern or if delay was expected, but no such cases were reported.
This triage protocol did not seem to have influenced the final destination of most patients. Of the 109 RA patients, 22 (20.2%) were eventually diagnosed with emergent large vessel occlusion requiring rescue MT. An additional 14 (12.8%) were treated with IV tPA only. Of the remainder, 32 (29.4%) still required admission to a neuro ICU for management of various conditions, including seizures and intracerebral hemorrhages. If taken to the closest community hospital ER, we estimate that 72 (66.1%) would have been transferred to tertiary care hospitals.
Approximately 31% of patients in this cohort were diagnosed with a stroke mimic. This is significantly higher than the 12.6% rate reported in the initial RACE experience.7 Compared with other studies,8–10 stroke mimics were identified with a similar frequency when the initial assessment was performed in the emergency department in our SA cohort. Most stroke mimics were seizures and encephalopathy, and additional training may be required to decrease this rate. Patients with seizures or symmetric weakness will not be declared RAs in the next phase of our protocol implementation.
The biggest impact of this protocol was on the door-to-needle time for IV tPA and the door-to-recanalization time for patients who underwent MT. Several centers have recently reported data from mobile stroke units as an alternative early triage tool for patients with acute stroke. Although both approaches are still in the early stages, MT rates are fairly comparable to those achieved by the mobile stroke units, with better door-to-recanalization times achieved in our cohort.11 Additionally, our fastest door-to-needle time of 16 min suggests that there remains room for improvement to better our median treatment times.
Our study is limited by the number of patients treated during the study period. Also, our unique geographic setting with several PSC-IC ERs in a small county may not be generalizable to other regions. Finally, our process improvements within the ER setting and the suboptimal efficiency of our old process are major confounding factors as they may have independently contributed to time improvements seen in the RA cohort.
Acknowledgments
The study investigators acknowledge all members of Lucas County EMS who made the Rapid Arterial oCclusion Evaluation (RACE) Alert protocol a possibility.
References
Footnotes
Contributors SFZ, MAJ: drafting, study design, data acquisition, analysis, and interpretation. JS, BP, AA, AK: data acquisition and analysis. AEM, HS: data acquisition, analysis, and interpretation. GT: study design, manuscript revision, data analysis and interpretation. DL: study design, manuscript revision.
Competing interests None declared.
Ethics approval Institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.