Article Text

Abstract
Introduction/Purpose Safety and efficacy of thrombectomy devices are assessed in large animal models with extracranial vascular occlusions1. These models do not incorporate important features of cerebrovascular thrombectomy, such as downstream emboli and cerebrovascular trauma2. We refine our previously developed canine ischemic stroke model3 to: (Aim 1) create a reproducible occlusion of the MCA, (Aim 2) achieve microcatheter navigation to the clot and (Aim 3) perform stent-retriever thrombectomy (TigerTriever 17, Rapid Medical, Yokneam, Israel).
Materials and Methods One mongrel (23.5 kg) and two hound-cross (24 kg) dogs were used for this study. A unilateral occlusion of the MCA was created by injecting autologous, barium-enhanced clot in the first two animals4 and a fibrin-rich clot in the third. Diffusion-weighted MRI was acquired at 51±7 min after clot injection. Upon confirmation of an ischemic stroke, endovascular treatment was attempted.
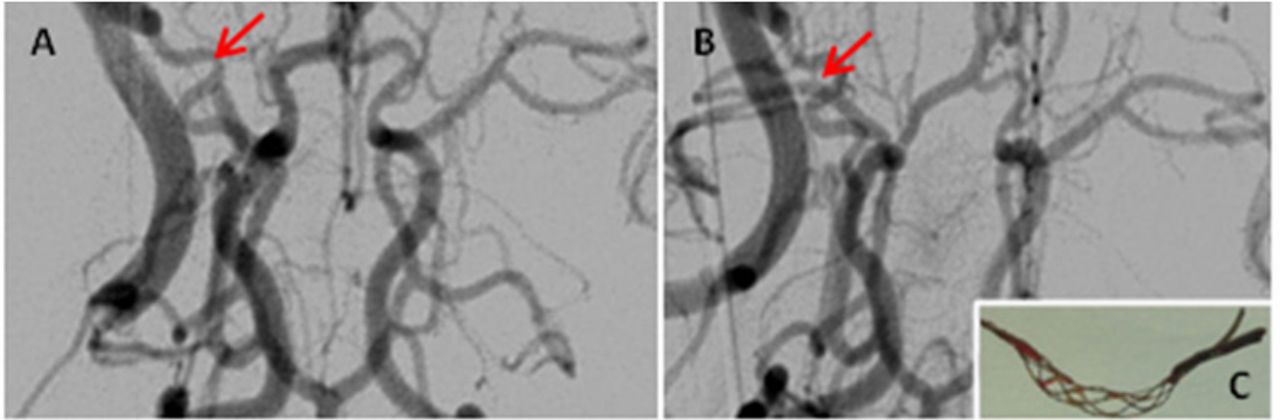
Results Occlusion of either the MCA (n=2) or the ICA terminus (n=1) was achieved in all animals (Aim 1). In the first animal, microcatheter access was complicated by perforation during microwire navigation (due to atypically small cerebrovasculature, MCA=0.76 mm) leading to subarachnoid hemorrhage (SAH). Despite successful clot extraction in this animal, documentation of revascularization failed due to increased intracranial pressure from the SAH. Refinement of the technique by using an intermediate catheter (DAC) to achieve better support in an extremely tortuous ICA was incorporated. In the second animal, distal microcatheterization was hampered by clot hardness followed by clot mobilization distally. Further refinement of the modeling included modification of the clot by incorporating fibrininogen and excluding barium. Uncomplicated microcatheter (1.7F) navigation distal to the clot and device delivery was achieved following model optimization (Aim 2). In all experiments, clot was mobilized and extracted by the controllable-expansion TigerTriever 17 device. In the two cases where reperfusion was documented, TICI 2a and TICI 2b were achieved in animals 2 and 3, respectively (Aim 3). Ultimately, this model optimization process required: (1) young hound-cross dogs with sufficient arterial diameters of the MCA (1.1±0.1 mm); (2) a tri-axial system with a 6Fr Shuttle sheath in the common carotid artery, a DAC 044 in the cervical ICA, and an SL-10 microcatheter for stent-retriever delivery to the MCA; and (3) modification of the clot model.

{kind=link}
Conclusion The development of a stroke model amendable to mechanical thrombectomy provides a potential paradigm to study neuroprotection strategies coupled with clinical standard-of-care endovascular treatment. Further reproducibility studies are underway.
References
. JNIS 2012;4:307–313.
. Stroke 2015;46:1099–1106.
. AJNR2012;33:353–358.
Disclosures O. Brooks: None. R. King: None. J. Chueh: None. M. Marosfoi: None. E. Nossek: 2; C; Rapid Medical. R. Eckhouse: 5; C; Rapid Medical. M. Gedulter: 5; C; Rapid Medical. M. Gounis: 1; C; Rapid Medical.