Article Text

Abstract
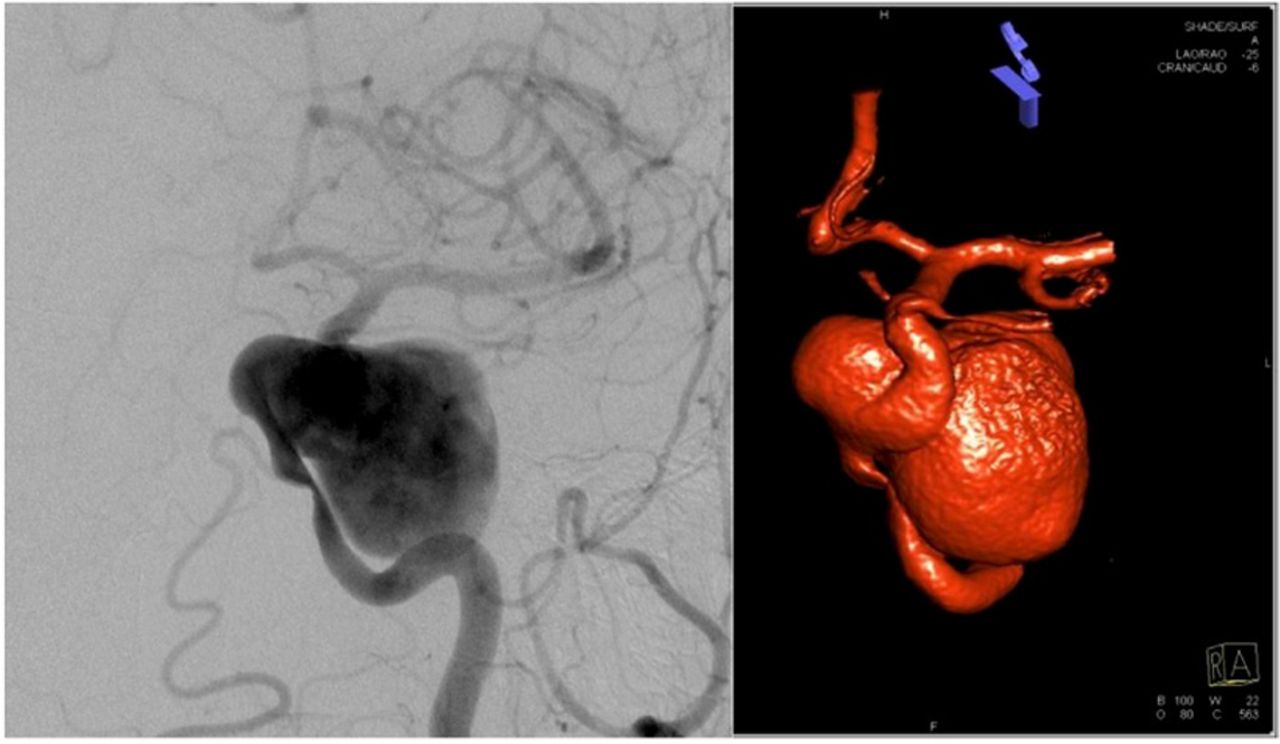
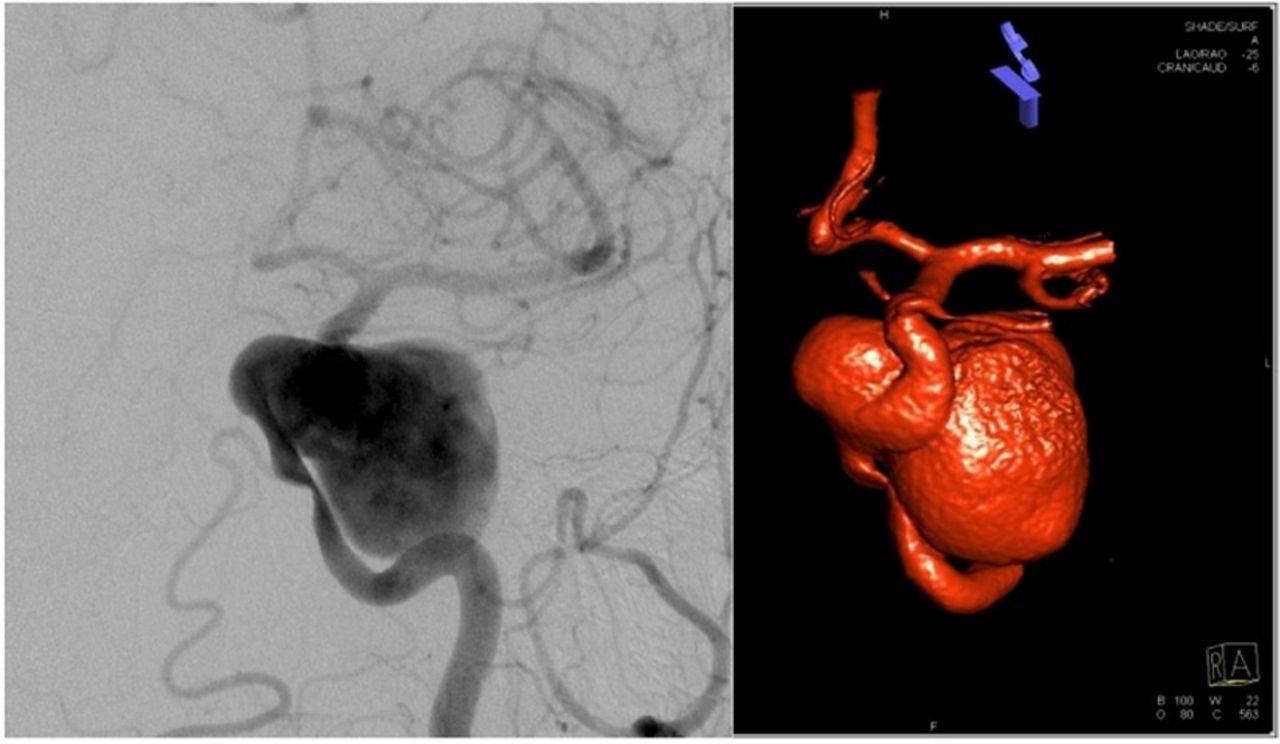
Background Cavernous carotid aneurysms (CCAs) represent a unique subset of intracranial aneurysms due to their distinct natural history and the anatomy of the cavernous sinus. Enlarging CCAs can cause elastic compression of the parent internal carotid artery (ICA). We suggest that cavernous carotid aneurysms which cause luminal stenosis of their parent vessels be referred to as “matricidal aneurysms.” Though many patients are asymptomatic, presenting symptoms of CCAs include ophthlalmoplegia with resulting diplopia, vision changes, pain, ptosis, facial numbness, and cavernous-carotid fistula. Less commonly, patients with CCAs can present with epistaxis, subarachnoid hemorrhage, and in cases of matricidal aneurysms, ischemia due to luminal stenosis. The proper management of stenosis caused by a matricidal cavernous carotid aneurysm is not well established and may not be intuitive.
Methods We present a multicenter retrospective case series of patients with matricidal CCAs.
Results 37 patients with matricidal aneurysms presented with both asymptomatic and symptomatic stenosis. These patients were treated with either conservative medical management, coiling, flow diversion, or endovascular sacrifice of the parent artery. Planned treatment modalities were not executed in 10 cases (27% treatment failure rate). Failure rates for individual treatments were 28% for flow diversion, 50% for parent vessel sacrifice with bypass, 0% for parent vessel sacrifice without bypass, 29% for coiling with or without balloon or stent assistance, and 100% for conservative management. Presenting symptoms, patient outcomes, and follow up data are presented for all cases.
Discussion/Conclusion Matricidal aneurysms require careful consideration and planning. The restricted anatomy of the cavernous sinus can make successful execution of endovascular interventions difficult. Direct elastic compression of the parent artery does not respond to angioplasty and stenting the way that atherosclerotic stenosis does. Because of this, planning for possible parent vessel sacrifice is important.
Abstract E-027 Table 1 Intended Treatments and Outcomes
{kind=link}
Abstract E-027 Table 2 Presenting Symptoms
Disclosures M. Roberts: None. C. Nickele: 1; C; Microvention. B. Welch: 2; C; Stryker Neurovascular, Covidien. V. Ban: None. A. Ringer: None. L. Kim: 2; C; Aesculap Inc., Microvention Inc.. 4; C; SpiSurgical. M. Levitt: 1; C; Covidien, Inc: unrestricted educational grant, Volcano Philips: unrestricted educational grant. G. Lanzino: 1; C; unrestricted educational grant: ev3/Covidien. 2; C; ev3/Covidien. P. Kan: 2; C; Medtronic, Stryker Neurovascular. H. Shallwani: None. A. Siddiqui: 1; C; Coinvestigator: NINDS 1R01NS064592–01A1, Coinvestigator: NIBIB 5 R01 EB002873–07, Coinvestigator: NIH/NINDS 1R01NS091075, Principal Investigator/National Steering Committee: Codman and Shurtleff LARGE Aneurysm Randomized Trial, Covidien (now Medtronic) SWIFT PRIME Trial, Medtronic’s Solitaire With the Intention For Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-retriever Thrombectomy in Acute Anterior Circulation Stroke (SWIFT DIRECT), MicroVention CONFIDENCE Study, MicroVention FRED Trial: Flow Diversion Versus Traditional Endovascular Coiling Therapy, Penumbra 3D Separator Trial, Penumbra COMPASS Trial, Penumbra INVEST Trial, MUSC POSITIVE Trial. 2; C; Amnis Therapeutics Ltd., Cerebrotech Medical Systems Inc., CereVasc LLC, Claret Medical Inc., Codman, Corindus Inc., GuidePoint Global Consulting, Medtronic, MicroVention, Neuravi, Penumbra, Pulsar Vascular, Rapid Medical, Rebound Therapeutics Corporation, Silk Road Medical Inc., Stryker, The Stroke Project Inc., Three Rivers Medical Inc., W.L. Gore and Associates. 5; C; Board Member: Intersocietal Accreditation Committee (Dr. Siddiqui receives no consulting salary arrangements. All consulting is per project and/or per hour). 6; C; Buffalo Technology Partners Inc., Cardinal Health, International Medical Distribution Partners, Medina Medical Systems, Neuro technology Investors, StimMed, Valor Medical. L. Elijovich: None. A. Arthur: 1; C; Siemens. 2; C; Codman, Stryker, Covidien, Medtronic, Sequent, Microvention.