Article Text

Abstract
Introduction/Purpose In-stent stenosis and intimal hyperplasia (IH) occur in 9% and 35%, respectively, after flow diverter treatment1. Although this phenomenon is not rare, severe, symptomatic flow limiting narrowing is rarely observed. Recently FD have been used in several cases in small vessels (off-label indication), which can potentially result in a higher rate of symptomatic in-stent stenosis or stent thrombosis. We sought to determine the patterns of intimal hyperplasia after flow diversion treatment using a high resolution intravascular imaging technique (optical coherence tomography). Furthermore, we assessed the effect of phosphoryl-choline surface modified FDs in preventing in-stent stenosis.
Materials and methods Forty New-Zealand white rabbits with elastase induced aneurysm were treated with classic Pipeline (C-PED) or with Pipeline-Flex with Shield Technology (S-PED). Four treatment groups were created, based on device type and the usage of dual anti-platelet therapy (DAPT). Ten animals per group were randomized for the following treatment: C-PED-no-DAPT, C-PED-with-DAPT, S-PED-no-DAPT, S-PED-with-DAPT. Optical coherence tomography was used in order to determine the location, thickness and the vessel involvement of intimal hyperplasia. Intimal hyperplasia was considered when the newly formed intraluminal tissue exceeded 0.1 mm in thickness and in stent stenosis when the lumen narrowing was >20%.
Results Intimal hyperplasia developed at two specific locations: at the mid-segment of FD (at the inner curve of the innominate artery), presented as a focal IH with a mean thickness of 0.11–0.16 mm. And at the distal end of FD, where the mean device/vessel ratio >1.8, presented as circumferential hyperplasia with mean IH: 0.14–0.22 mm. Mild in-stent stenosis (20%–50%) was only seen distal to the vertebral artery. In stent stenosis was identified in 5 cases (50%) in C-PED group with and without DAPT, in 33% in S-PED-no-DAPT and in 0% in S-PED-with-DAPT. Phosphoryl-choline surface modified FD with DAPT showed a significant (Fisher’s exact, p<0.05) reduction in in-stent stenosis when compared to classic Pipeline.

{kind=link}
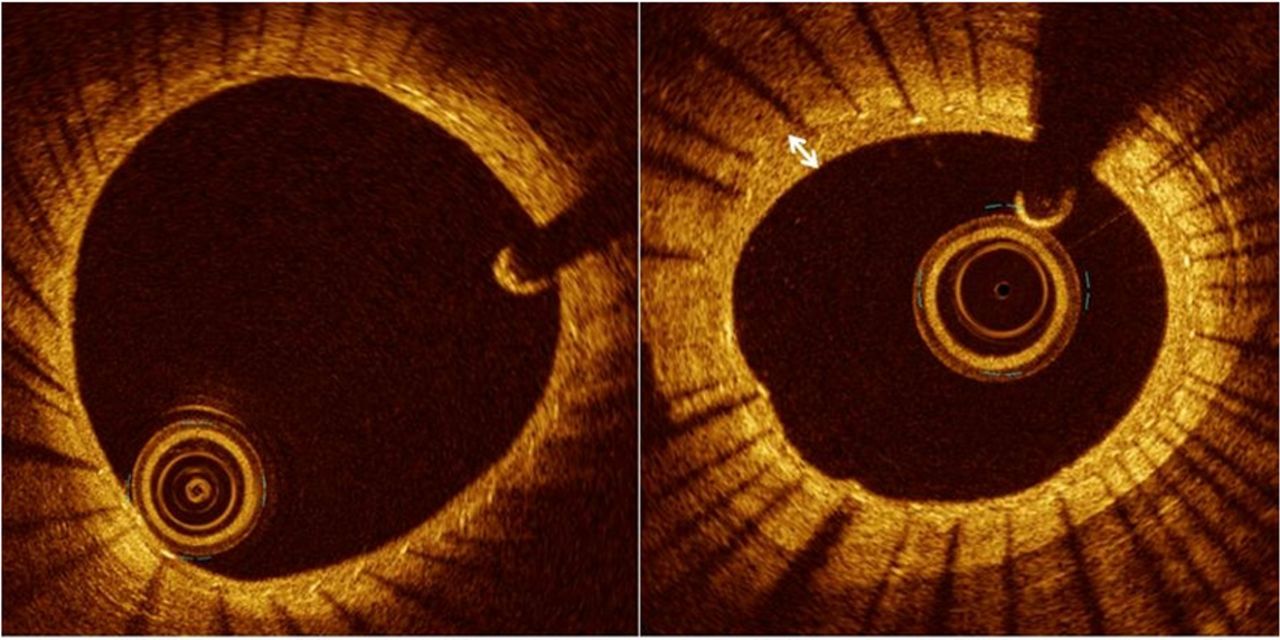
(A) Neointimal formation with no intimal hyperplasia; (B) Circumferential intimal hyperplasia with maximum thickness = 0.25 mm (arrow)
Conclusions Our preliminary study suggests that the distal end of the FD (landed in small vessel) and the area of high metal density (mid-portion of FD) are more prone to develop intimal hyperplasia. Furthermore, using phosphoryl-choline surface modified flow diverters can be beneficial in preventing in-stent stenosis in small vessels.
Reference
. Neurosurgery. 2016;78:862–867
Disclosures M. Marosfoi: None. F. Clarençon: None. E. Langan: None. R. King: None. O. Brooks: None. T. Tamura: None. J. Wainwright: 5; C; Medtronic Neurovascular. M. Gounis: 1; C; Medtronic Neurovascular. A. Puri: 1; C; Medtronic Neurovascular.