Article Text

Abstract
Background Endovascular treatment of wide-necked aneurysms remains challenging without the use of adjunctive devices to preserve the parent artery.
Objective To present our initial experience with a temporary bridging device, the Comaneci (Rapid Medical, Israel). The compliant remodeling mesh protects the parent artery during coil occlusion without flow arrest in the distal vasculature. Permanent dual antiplatelet therapy is not required since the device is fully removed at the end of the procedure.
Methods All intracranial aneurysms treated by coil occlusion with the Comaneci device between December 2014 and November 2015 were included. Angiographic and clinical results were retrospectively analysed, including follow-up examinations. All aneurysms were unruptured.
Results 18 aneurysms of the internal carotid artery were included. Successful coil occlusion assisted by the Comaneci device as intended was possible in 14 cases (77.8%). Insufficient coverage of the aneurysmal neck was observed in four cases (22.2%), with modification of the treatment to stent-assisted coiling or remodeling. One clinically relevant complication occurred (5.6%).
Conclusions Our initial experience shows that use of the Comaneci device is straightforward for the treatment of selected wide-necked aneurysms. Further studies with long-term follow-up data are needed to identify the significance of the presented technique in the neurointerventional armamentarium.
- Aneurysm
- Device
- Intervention
- Angiography
- Balloon
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Endovascular treatment of both ruptured and unruptured intracranial aneurysms is a well-established treatment option for the majority of patients.1 Aneurysms in which a defined neck serves as a boundary line to the parent artery can be treated by standard coiling, without the need for adjunctive devices in most cases. Use of standard endovascular techniques to treat aneurysms with complex shapes especially wide-necked aneurysms remains a challenge. Stent-assisted coiling (SAC), and flow diversion, are both approaches that focus on reconstruction of the affected section of the parent artery with or without additional coiling of the aneurysm.2 ,3 However, the need for dual antiplatelet therapy with the risk of hemorrhagic or thromboembolic complications places these techniques at a considerable disadvantage. The remodeling technique, with preservation of the parent artery by a compliant balloon during insertion of coils into the aneurysm, increases the risk of thromboembolic complications, as the inflation of the balloon arrests flow in the parent artery.
The Comaneci device deals with these problems. The compliant remodeling mesh temporarily bridges the neck of the aneurysm to support coil occlusion without compromising flow in the parent artery.
In this paper we describe our initial experience gained from the endovascular treatment of 18 wide-necked intracranial aneurysms of the internal carotid artery (ICA) using the Comaneci device.
Material and methods
Comaneci device
The Comaneci device is a compliant radiopaque mesh composed of 12 nitinol wires mounted on a 182 cm core wire (figure 1). The device is CE marked, and not cleared by the Food and Drug Administration. The distal end of the device consists of a 7 mm flexible tip, allowing for gentle and safe navigation. The device is released via a 0.021 inch microcatheter. The cell size of the device measures 1.33 mm2 at the nominal diameter of 3.0 mm.

Demonstrates the compliant mesh of Comaneci in a broad-based aneurysm model.
Three versions of the device are available. The standard version has a length of 32 mm, which shortens to 12 mm when deployed in a vessel of 4.5 mm diameter. The shorter version (Comaneci Petit) measures 27 mm before deployment and contracts to 10 mm when fully deployed in a vessel of 3.5 mm diameter. The extent of expansion is adjustable by the operator via a slider at the handle.4
A third version of Comaneci is also available but was not included in the series. It is the Comaneci 17 which is delivered via a 0.0165 inch microcatheter.
Patient population and aneurysm characteristics
We retrospectively analyzed all medical records and radiographic studies of patients with intracranial aneurysms who were treated by endovascular coil occlusion with the Comaneci device at our institution between December 2014 and November 2015. The decision to use endovascular treatment was reached in a multidisciplinary conference. Inclusion criteria were wide-necked intracranial aneurysms with an expected difficulty of standard coiling. Wide-necked was defined as a dome-to-neck ratio (aspect ratio) of ≤2.5 Only sidewall aneurysms of the ICA were considered for treatment with the Comaneci device in our initial phase with this new technique.
Only incidental findings of aneurysms or remnants of previously coiled aneurysms were included. Exclusion criteria for the treatment with the Comaneci device were a previous stent implantation in the target vascular territory; a bifurcation-type aneurysm; fusiform shape; or extradural location of the aneurysm.
All patients were informed about the planned treatment strategy, and given a detailed explanation of all treatment alternatives, at least 24 hours before the procedure. Our retrospective study received approval of the local ethical review committee.
The clinical pre- and postinterventional status of each patient was graded by a neurosurgical team member according to the modified Rankin scale (mRS).
Endovascular procedure
In each procedure, either an 8F/6F guiding catheter combination, or an 8F catheter alone, was introduced into the target artery. Three-dimensional (3D) rotational angiography aided in visualizing the aneurysm without superposition of surrounding vessels (working position) where necessary. A 0.021 inch microcatheter (Prowler select; Codman & Shurtleff, Inc, Massachusetts, USA or VIA; Sequent Medical, Inc, California, USA) was navigated into the parent artery and placed distally to the aneurysm, while a 0.014 inch Excelsior SL10 microcatheter (Stryker Neurovascular, California, USA) was positioned inside the aneurysm. The choice between Comaneci and Comaneci Petit was based on measurements of the affected artery and widths of the aneurysmal orifice, based on 2D angiographic runs. Expansion of the device, necessary to cover the aneurysm neck, results in an explicit shortening (32 to 12 mm vs 27 to 10 mm for Comaneci Petit when fully deployed), which must be considered when preparing the treatment strategy. To guarantee a stable bridging position we recommend the longer version, especially for neck sizes close to the maximum length of Comeneci Petit.
The device was loaded into the microcatheter and navigated to a position providing optimal coverage of the aneurysm neck. Unsheathing of the device by withdrawal of the microcatheter, followed by cautious expansion of the device using a slider on the control handle, facilitated the neck coverage of the aneurysm. The correct expansion of the device, with proper adaptation to the circumference of the parent artery, was documented by fluoroscopy at various angles.
Once the aneurysm neck was completely covered by the remodeling mesh, the expansion was fixed with the locking screw on the control handle. At this point the first coil was inserted into the aneurysm via the previously placed microcatheter. Coil loops that evolved directly toward the bridging mesh of the Comaneci device were repositioned to avoid an interlacing between the coil loops and the mesh. The Comaneci device was manually ‘deflated’ before detachment of the first coil, to document the stable position of the first coil. This was followed by successive coil occlusion of the aneurysm under permanent protection by the expanded device. Finally, the device was recaptured into the microcatheter and withdrawn from the target artery.
Antiplatelet and anticoagulation regimen
All patients were placed on dual antiplatelet therapy with clopidogrel or ticragrelor and acetylsalicylic acid at least 1 day before the procedure in order to provide an opportunity for SAC if the Comaneci device failed. Once the procedure was completed as intended, treatment with clopidogrel was stopped. Acetylsalicylic acid (100 mg) was continued for 4 weeks, in anticipation of any thromboembolic complications secondary to the broad contact between the coil loops and the bloodstream.
Follow-up schedule
Angiographic and clinical follow-up examinations were carried out 3 and 12 months after the intervention. The angiographic results were classified into three grades: complete occlusion, minor neck remnant, and incomplete occlusion.
Results
Patient population and baseline characteristics of aneurysms
Seventeen patients with 18 intracranial aneurysms of the ICA were scheduled for endovascular treatment assisted by the Comaneci device during the sample period. The mean age of the 13 female and the 4 male patients was 49.7 years.
Fourteen aneurysms were found incidentally and four were remnants or reperfusions of previously coiled aneurysms. Eleven of the 18 aneurysms were located at the posterior communicating artery segment of the ICA, whereas seven were paraophthalmic aneurysms.
The mean fundus diameter of all aneurysms in this series was 6.0 mm (range 2.0–12.0 mm) with a mean neck size of 3.9 mm (range 2.0–8.0 mm).
Fifteen patients had a mRS score of 0 before the procedure, whereas one had a mRS score of 2, caused by an unrelated ischemic stroke, and two were mRS 3 caused by a previous subarachnoid hemorrhage unrelated to the target aneurysm. In one patient, the mRS grade declined from 0 to 1 related to the procedure. The remaining patients were discharged with unchanged mRS grades.
The baseline characteristics of the treated aneurysms are summarized in table 1.
Baseline aneurysm characteristics; aneurysms scheduled for endovascular treatment assisted by the Comaneci device including baseline anatomical findings, immediate, and F/U (follow-up) angiographic results, alternative treatment strategies and complications
Technical results
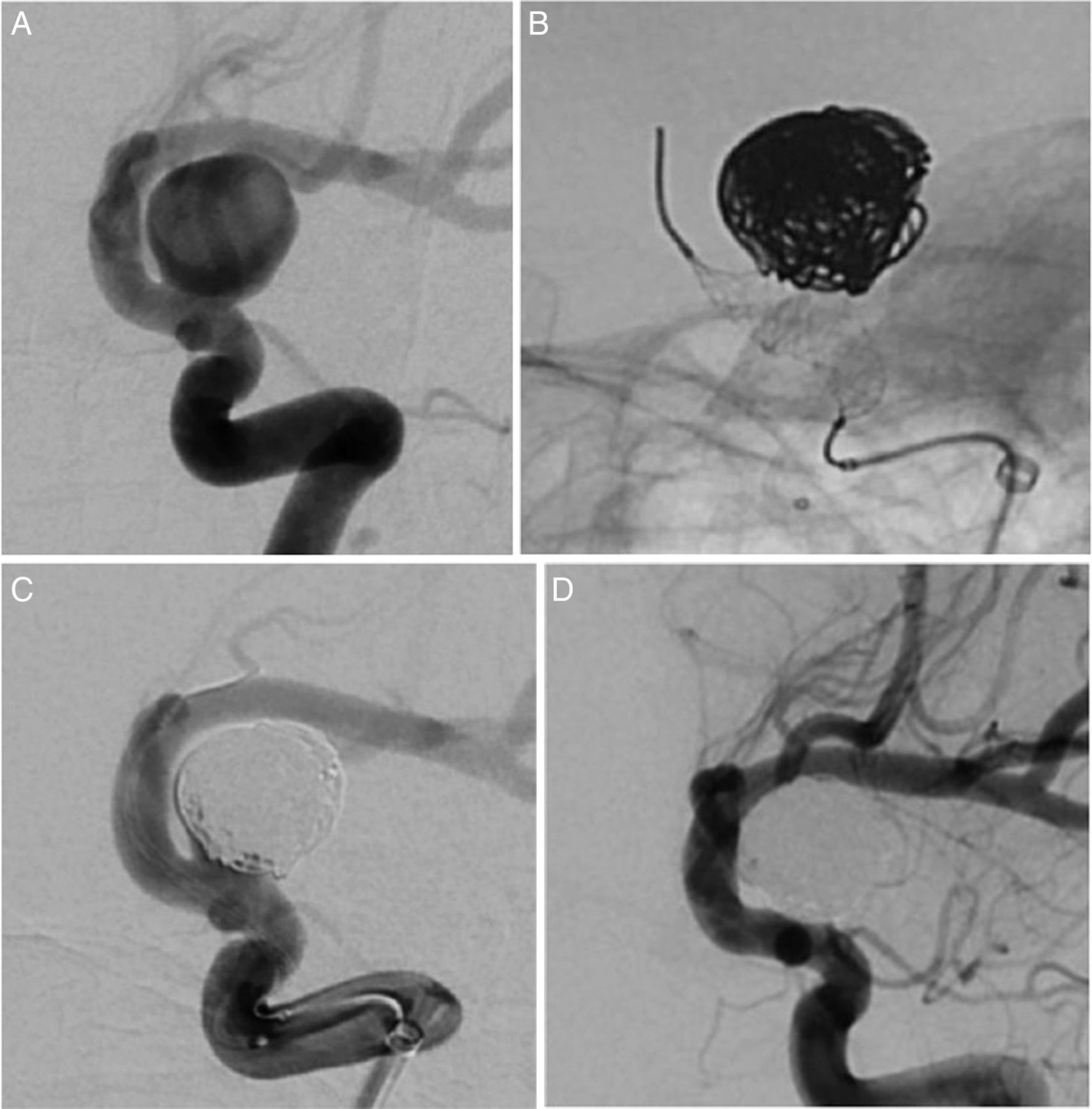
Coil occlusion with the Comaneci device, including uneventful insertion, expansion and withdrawal of the device, was carried out as intended in 14 (77.8%) cases (figure 2A–D). In four cases (cases 2, 6, 7, 9) a stable position of the Comaneci device with proper expansion and coverage of the vessel wall and the aneurysm orifice could not be achieved (figure 3). The treatment strategy was changed to SAC in two of these cases, and the remaining two cases were treated using the remodeling technique, with a compliant balloon (Scepter C, MicroVention, Tustin, California, USA).
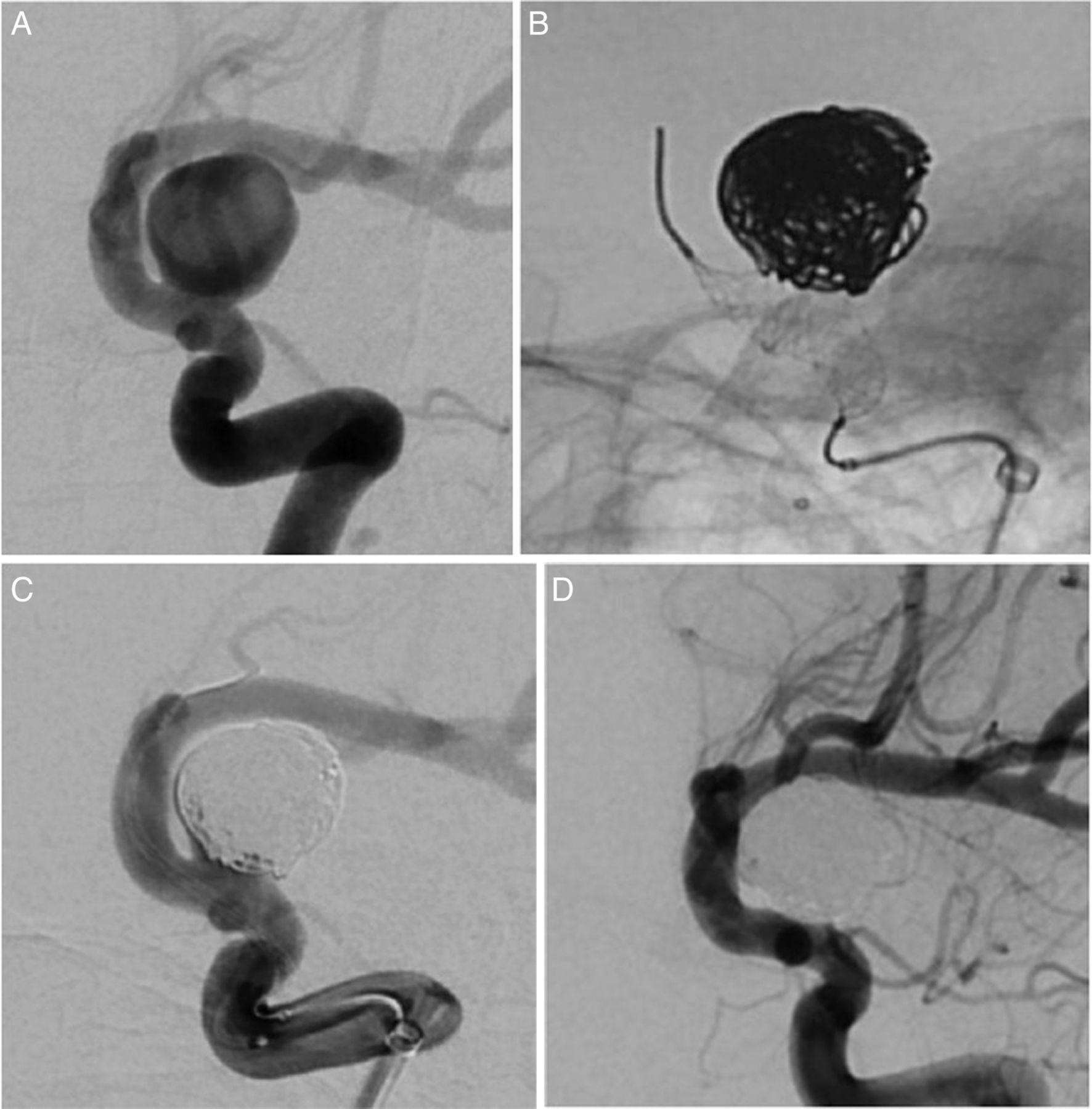
(A) Incidental finding of a broad-based internal carotid artery (ICA) paraophthalmic aneurysm; an additional small ICA paraophthalmic aneurysm originating slightly proximal to the ophthalmic artery origin; right anterior-oblique view. (B) Coiling of the aneurysm assisted by the Comaneci device; sufficient coverage of the aneurysm neck; right anterior-oblique view. (C) Final result with near complete occlusion of the aneurysm and stable position of the coils after ‘deflation’ of the Comaneci device; right anterior-oblique view. (D) Follow-up angiography 4 months later demonstrated a complete occlusion of the aneurysm; right anterior-oblique view.

{kind=link}
{kind=link}
{kind=link}
Insufficient coverage of a small internal carotid artery (ICA) paraophthalmic aneurysm owing to an incomplete expansion of the Comaneci device possibly caused by the highly curved segment of the ICA; the treatment strategy was changed to stent-assisted coiling; right anterior-oblique view.
Complications
As indicated in table 1 one complication occurred, which might have been device-related. In this patient (case 12), with a right-sided ICA posterior communicating (Pcom) aneurysm, the Comaneci could not be completely ‘deflated’ before removal and it was therefore withdrawn without protection of the microcatheter. The postprocedural angiogram was without pathological findings. The patient developed a left-sided hemiparesis within 3 hours after the intervention. Digital subtraction angiography disclosed a thrombotic occlusion of the target ICA that was successfully recanalized by mechanical thrombectomy. The patient's clinical condition improved significantly to a mRS grade of 1, with a remaining mild weakness of the left arm at discharge. Retrospective analysis of this case leads to the assumption that a dissection, followed by the removal of the Comaneci device, caused the parent artery occlusion.
Another patient (case 10) with an acute groin hematoma 3 days after the intervention was treated with a covered stent, without clinical impairment during the follow-up period.
Immediate and follow-up anatomical outcome
Among the 14 aneurysms treated with the Comaneci device, immediate complete occlusion was achieved in nine (64.3%) cases compared with five (35.7%) cases with a remaining neck remnant.
At least one angiographic follow-up angiogram has been obtained in 11 cases, with a median follow-up interval of 4.8 months. Of those, nine (81.8%) showed a complete occlusion and two (18.2%) a near-complete aneurysm occlusion. Of the remaining cases, one examination is scheduled and two patients have been lost to follow-up.
One clinically silent ICA occlusion without evidence of a causal relation to the device was documented at the 3-month follow-up examination in a patient with a small ICA Pcom aneurysm on the right side. In another case of a small ICA Pcom aneurysm, 3-month follow-up angiography showed dislocation of a single coil loop into the parent artery without flow limitation or thrombus formation.
Discussion
Several endovascular techniques seek to deal with the problem of wide-necked aneurysms. These techniques aim to preserve the parent artery with permanently or temporarily deployed adjunctive devices. Standard coiling of wide-necked aneurysms increases the risk of thromboembolic complications or vessel occlusions caused by a partial or complete dislocation of coils into the lumen of the parent artery. SAC and balloon-assisted coiling (BAC) are the best established strategies for wide-necked or complex aneurysms.6–8 However, numerous innovative techniques have been introduced in recent years, in which the concept of flow-diverting devices capable of promoting intra-aneurysmatic thrombosis is clearly the most remarkable.9 ,10 The complete occlusion rate after 6 months was better with SAC than with BAC for similar complication rates, as demonstrated in a meta-analysis by Wang et al.11 The complete occlusion rate of intracranial aneurysms treated with extra-aneurysmatic flow diverters increases progressively, up to 81.5% during the follow-up period.12
BAC represents an opportunity to treat wide-necked aneurysms without the need for postprocedural antiplatelet therapy. BAC, in contrast to the Comaneci, offers the possibility of temporary occlusion of the parent artery, which becomes essential when an intraprocedural aneurysm ruptures. The main limitation of BAC is a complete flow arrest in the parent artery during inflation of the balloon which, in combination with the essential deflation and inflation maneuvers, increases the risk of thromboembolic events caused by vasospasm, endothelial damage, or prolonged flow arrest.13–15
The concept of a temporary neck remodeling stent refers to these limitations. Almekhlafi et al16 described three cases of intracranial aneurysms treated analogously to BAC with a temporarily deployed Solitaire stent that was completely removed at the end of the procedure. Although no complications were encountered in these three cases, a major drawback of the presented technique remains. The visibility of conventional self-expanding stents like the Solitaire stent is insufficient to define a clear margin between the coil loops and the stent struts at the aneurysm orifice. An interaction of coil-loops with the stent struts might result in severe complications followed by the retrieval of the stent.
The Comaneci provides a compliant remodeling mesh, comparable to a compliant balloon, without the drawback of blocked flow within the parent artery during expansion of the device. Once the Comaneci covers the aneurysm orifice sufficiently, no further deflation and inflation maneuvers are required, and this can reduce the risk of vessel injuries. The overall remodeling capability of the device, compared with a compliant balloon, is difficult to assess. Highly compliant balloons like the Scepter XC balloon (MicroVention, Tustin, California, USA) probably offer a more distinctive remodeling competence, especially in cases of highly curved arteries or broad-based bifurcation aneurysms.
Overall, our experience with the Comaneci device is promising. Once a stable position of the device with complete expansion above the aneurysmal neck is achieved, occlusion of the aneurysm is possible without difficulty. We did not observe any cases of interaction between coil loops and the device, mainly owing to the high radio-opacity of the mesh. Retrieval of the device with inflation and resheathing into the microcatheter was achieved without difficulty in all except one of 18 cases. Two ICA occlusions occurred, but the second of these was a clinically silent occlusion during the follow-up period without evidence of a causal relation to the device. The complication rate related directly to the device (5.6%; 1/18) is similar to that of other adjunctive devices such as balloon-assisted aneurysm embolization (5.5%, 8.1% 9.5%, 12.5%).17–20
Nevertheless, four aneurysms were not sufficiently covered by the device owing to an incomplete expansion within the target artery, and the operator decided to change the treatment strategy. In retrospect, we could not identify any possibly anatomical circumstances that might explain these failures with the Comaneci. Apart from potential technical problems, this might also be attributable to our limited experience with a new mechanically expandable device.
Gupta et al,21 in their animal study involving 20 elastase-induced aneurysms, analyzed the occurrence of endothelial injury with the Comaneci device compared with a compliant balloon. In contrast to the results one might have expected based on the structure of 12 nitinol wires compared with the smooth surface of a balloon, the rate of endothelial damage was not increased in the Comaneci group in comparison with the balloon group. The aneurysm obliteration rates did not differ between the two groups, demonstrating the similarity of Comaneci compared with a compliant balloon in this preclinical evaluation.
We observed one acute and one delayed case of ICA artery occlusion, as described above. No evidence of parent artery dissection was found angiographically. The possibility of hidden endothelial damage induced during expansion and positioning of the device cannot be ruled out completely. Lawson et al4 in their series of three aneurysms treated with the Comaneci, observed one thromboembolic phenomenon. They discussed the possibility that the device itself might be the source of the emboli, although no clot was found within the device during and after the bridging time. The reason for the thromboembolic complication remains unclear, as it does in our cases. General procedure-related circumstances (ie, comparatively large catheters, two microcatheters, and procedure time) are to be considered as causative factors as well. Further studies of the safety and efficacy of the Comaneci device, in addition to those of Gupta et al21 and Lawson et al,4 are needed.
Current technical drawbacks of the Comaneci that require addressing are the need for a comparatively large microcatheter and the somewhat jerky reaction of the device to the manipulation of the slider. A smaller version of the Comaneci, compatible with a 0.0165 inch microcathter, has been introduced since we carried out our study. The potential risk of endothelial injuries might be reduced by a modification of the surface of the device by using smoother wires.
Limitations of the study
Our study has a number of limitations, mainly due to its retrospective design. Log data on the total duration of each treatment, including the number of inflation and deflation maneuvers of the Comaneci inside the target artery, would have been valuable, especially against the background of potential endothelial injuries.
The absence of a control group treated by BAC and/or SAC impedes a final estimation of the remodeling capability of the device compared with established treatment modalities.
Conclusion
Our study demonstrates that coil occlusion of wide-necked aneurysms assisted by the Comaneci device is feasible and effective. A prospective trial including a comparison of long-term obliteration rates achieved with the Comaneci and with BAC would help to identify the significance of this new device in the existing and future armamentarium of neurovascular tools.
References
Footnotes
Preliminary data from this series were presented during the 2016 ABC-WIN seminar in Val d′Isere/France and during the 2016 annual meeting of the German Society of Neurosurgery in Frankfurt/Germany.
Contributors SF: conception and design of the work, data acquisition, analysis and interpretation, writing of the manuscript. AW and AC: critical review of the work. FD and FG: data acquisition, critical review of the work. WW: conception and design of the work, final approval of the manuscript.
Competing interests SF: support for travel to meetings—travel expenses for the meeting of the German Society of Neurosurgery 2016.
Ethics approval Ethics committee of Ruhr University Bochum, Germany.
Provenance and peer review Not commissioned; externally peer reviewed.