Article Text

Abstract
Background The feasibility of performing MRI first for patients with suspected hyperacute stroke in real-world practice has not been fully examined. Moreover, most past studies of reducing door-to-reperfusion time (DRT) in endovascular treatment (EVT) were conducted using CT. The aim of this study was to evaluate the feasibility of an MRI-first policy and to examine the effects of a quality improvement (QI) process for reducing DRT using MRI.
Methods From January 2013 to December 2018, consecutive patients with acute stroke who came to hospital directly and were treated with emergent EVT were prospectively enrolled into the present study. In principle, MRI was performed first for patients with suspected acute stroke. A step-by-step QI process for decreasing DRT was adopted during this period. Time metrics for EVT were compared between specific time periods.
Results A total of 180 patients (71 women; median age 76 years (range 69–64); National Institutes of Health Stroke Scale score 17 (range 10–23)) were included in the present study. More patients in the late phase were managed with the MRI-first policy (p<0.001). DRT (199 min in Phase 1, 135 min in Phase 2, 129 min in Phase 3, and 121 min in Phase 4, p<0.001) was significantly reduced across the phases. The percentage of patients with DRT <120 min increased significantly across time periods (p<0.001). Symptomatic intracerebral hemorrhage did not increase across phases (p=0.575).
Conclusion An MRI-first policy was feasible, and DRT decreased considerably with a step-by-step QI process. This process may be applicable to other hospitals.
- stroke
- MRI
- thrombectomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Time from symptom onset to reperfusion plays a critical role in managing ischemic stroke patients with emergent large vessel occlusion (ELVO),1–3 and urgent endovascular treatment (EVT) for reperfusion is recommended for most stroke patients with ELVO.4 Because the probability of a good functional outcome decreases as stroke onset to reperfusion time increases,1 3 guidelines or statements emphasize the importance of minimizing onset to reperfusion time.4 5 For in-hospital workflow, some time metrics have been proposed, such as door-to-imaging time (DIT), door-to-puncture time (DPT), and door-to-reperfusion time (DRT). In the ideal stroke process timelines suggested by the Society of NeuroInterventional Surgery statement, DPT should be <60 min and DRT <90 min.5 Various reports of reducing these time metrics using quality improvement (QI) processes have been published.6–9
In most past studies trying to reduce these time metrics, CT and/or CT angiography (CTA) was performed as a screening modality for hyperacute ischemic stroke. CT has some advantages, such as requiring a short time and availability at any time in almost all hospitals with an emergency department (ED). However, there is controversy about patient selection by CT/CTA or MRI. MRI-based patient selection has a potential to better screen patients for candidates for EVT in terms of their likelihood to benefit from immediate reperfusion therapy.10 Diffusion-weighted imaging (DWI) depicts the extent of the ischemic core lesion well,11 and easily shows patients with a large ischemic core. Moreover, MR angiography (MRA) can show the site of arterial occlusion without contrast medium injection, and such information may be beneficial for considering subsequent EVT. However, few institutions perform MRI as an initial examination for patients with suspected acute stroke12 because it is much more time-consuming than CT13 14 and is probably not always available, and the feasibility of performing MRI first for patients with suspected acute stroke in real-world practice has not been examined sufficiently.12
The aim of the present study was to evaluate the feasibility of an MRI-first policy in conducting EVT and to examine the effect of a step-by-step QI process for decreasing DRT using MRI as the routine screening modality.
Methods
The Nippon Medical School is a major general academic teaching hospital in central Tokyo. It is a tertiary general hospital and treats more than 10 000 patients per year through the ED, including >600 stroke admissions annually, and CT and MRI are available at any time.12
From January 2013 to December 2018, consecutive patients with acute ischemic stroke who were treated with emergent EVT at admission were retrospectively recruited from the prospective registry. Patients treated with EVT after admission (eg, for symptom progression) or patients who were attempted to be treated with EVT but with no procedure (eg, effective recanalization on first angiogram after intravenous tissue plasminogen activator (t-PA)) were excluded. EVT for ELVO patients was conducted generally based on, but not limited to, our domestic guideline (briefly, EVT was strongly recommended for stroke patients within 6 hours from symptom onset, with internal carotid artery or middle cerebral artery horizontal segment occlusion, Alberta Stroke Program Early CT Score (ASPECTS) ≥6, and National Institutes of Health Stroke Scale (NIHSS) score of ≥6; EVT was also recommended for patients within 24 hours from onset, with ASPECTS ≥7 and NIHSS ≥6).15 For candidate patients outside the guideline, EVT was conducted based on clinical-DWI mismatch, and generally there were no limits about time window, ASPECTS, NIHSS score, or the site of arterial occlusion (distal and/or posterior circulation).
This study was approved by the institutional ethics committee. Written informed consent for enrollment into the study and data collection was obtained from all patients or their next of kin.
Clinical characteristics of patients
Clinical background characteristics including sex, age, vascular risk factors, and time of arrival at the ED (with office hours defined as Monday to Friday, 08:30–16:00 hours) were recorded on admission. Stroke severity was assessed using the NIHSS. The site of arterial occlusion was determined using the first angiogram. Time metrics related to hyperacute stroke management such as DIT, DPT, DRT, imaging-to-puncture time (IPT), and puncture-to-reperfusion time (PRT) were also recorded. Successful reperfusion was defined as a modified Thrombolysis in Cerebral Infarction score16 of 2b or 3. Concomitant t-PA treatment and symptomatic intracerebral hemorrhage (sICH) were documented. For patients treated with intravenous t-PA, door-to-needle time was also recorded. sICH was defined as new parenchymal hemorrhage within 36 hours after EVT, corresponding to an increment in the NIHSS score of ≥4 points. Stroke etiology was determined using the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) criteria,17 and functional outcomes were classified by the modified Rankin scale (mRS) score18 3 months after stroke onset.
Step-by-step QI process for decreasing DRT
The step-by-step quality improvement process for decreasing DRT is shown in table 1.
Step-by-step quality improvement
Phase 1: January 2013 to February 2015
From January 2013, multimodal 1.5 T MRI (Echelon Oval, Hitachi Medical Systems, Tokyo, Japan) was performed first for patients suspected of having hyperacute stroke (<4 hours from onset at ED arrival) and who arrived at the hospital within office hours in principle; exceptions to the MRI-first policy were permitted at the attending neurologist’s discretion if the patient had contraindications to MRI, the general condition of the patient was poor, or MRI was unavailable due to its use for other patients. The patients were screened by a vascular neurology fellow or attending neurologist both during and outside office hours (throughout the following phases). DWI (TR/TE 6000/65 ms; b-values 0 and 1000 s/mm2; field of view 24 cm; acquisition matrix 128×128; and slice thickness 4.5 mm, with a 2.5 mm intersection gap, takes 55 s), time-of-flight MRA (330 s), fluid-attenuated inversion recovery (FLAIR, TR/TE 10000/120 ms; TI 2500 ms; field of view 24 cm; acquisition matrix 288×224; and slice thickness 4.5 mm, with a 2.5 mm intersection gap, 161 s), T1-weighted imaging (TR/TE 540/12 ms, 140 s), T2-weighted imaging (TR/TE 4200/117.52 ms, 173 s), and T2*-weighted imaging (TR/TE 480/18 ms; field of view 24 cm; acquisition matrix 256×204; and slice thickness 4.5 mm, with a 2.5 mm intersection gap, 136 s) were performed routinely in this phase. For patients screened with CT, additional imaging (CTA or MRA) could be performed, mainly to assess large vessel occlusion. Our stroke unit opened and pre-notification by the emergency medical service (EMS) for suspected acute stroke patients was started during this phase.
Phase 2: March 2015 to March 2016
The stroke management system was re-evaluated by a working group from neurology, emergency, radiology, and nursing. MRI was performed first for patients suspected of having acute stroke regardless of onset-to-door time and time of arrival (office hours or not). Routine MRI sequences were limited to DWI, MRA (faster protocol (200 s) was adopted), FLAIR, and T2*-weighted imaging, and rapid examination point-of-care tools to measure complete blood cell count (Celltac ES, NIHON KOHDEN Corporation, Tokyo, Japan), serum glucose, creatinine (ABL800 FLEX, Radiometer, Copenhagen, Denmark), and partial thrombin time-international normalized ratio (CoaguCheck XS, Roche Diagnostics, Rotkreuz, Switzerland) were introduced. In this phase, patients with ELVO having an indication for t-PA were transferred from the imaging room to the stroke unit and started on intravenous t-PA, and then delivered to the angiosuite.
The details of the QI processes in Phases 1 and 2 have also been described elsewhere.12
Phase 3: April 2016 to August 2017
From April 2016, the hyperacute stroke management system had further improved for reducing DPT. Patients with ELVO were directly transferred to the angiosuite from the imaging room, and t-PA was started wherever. A pre-hospital scale that could predict ELVO was introduced with cooperation of the EMS during this phase.19 Multidisciplinary staff meetings were held to review past cases or to familiarize them with the stroke management system for suspected ELVO patients through role play.
Phase 4: September 2017 to December 2018
Stent retrievers and large (0.068 inch) inner lumen aspiration catheters were introduced as on-label in our institution from September 2017.
Statistical analyses
First, the clinical characteristics of the patients including the proportion of patients who received MRI first, time metrics, and the ratio of cases with DRT <90 or <120 min of the included patients were compared among the phases. For this purpose, the time of the final angiogram was set as the time of reperfusion when reperfusion was not achieved. Because patients with ELVO stroke transferred from a primary stroke center (confirmed ELVO diagnosis, always with pre-notification, and skip head imaging and laboratory tests in our hospital) or patients with in-hospital onset (essentially onset-to-door time (ODT) is zero and never pre-notified) have distinct characteristics from patients who come directly to our hospital20 (see online supplementary table l), only cases who came directly to our hospital were assessed in the present study. Univariate analyses were performed using the χ2 test, Fisher’s exact test, the Kruskal–Wallis test, or the Mann–Whitney U test, as appropriate. The data are presented as median (IQR) or numbers (%). Second, differences in time metrics were evaluated according to several subgroups: arrival timing, EMS pre-notification, and first imaging modality. Finally, factors affecting DRT in Phases 3 and 4 were analyzed using multiple linear regression analysis with a backward stepwise selection procedure. Sex, age, risk factors, etiology, EMS pre-notification, arrival timing, ODT, severity, first imaging modality, major artery occlusion, and t-PA use were included in the model. All statistical analyses were performed using PASW for Windows version 17.0 software (SPSS, Chicago, Illinois, USA). Results were considered significant at p<0.05.
Supplemental material
Results
From January 2013 through December 2018, 2344 patients with acute (<7 days from onset) ischemic stroke were admitted to our stroke center: 706 in Phase 1, 442 in Phase 2, 638 in Phase 3, and 558 in Phase 4. During this period, a total of 355 EVTs (41 (1.6/month) in Phase 1, 48 (3.7/month) in Phase 2, 117 (6.9/month) in Phase 3, and 149 (9.3/month) in Phase 4) were conducted and, of these 355 EVTs, 326 were for ELVO. The rate of patients treated with EVT of those with acute stroke was significantly different among the phases (5.8% in Phase 1, 10.9% in Phase 2, 18.3% in Phase 3, and 26.7% in Phase 4, p<0.001). The online supplementary table shows the clinical background characteristics of the patients with ELVO who received EVT. The prevalence of risk factors, premorbid mRS score (p=0.002), time metrics of EVT, the proportion of skip head imaging (p<0.001), major artery occlusion (p=0.016), and concomitant t-PA therapy (p=0.006) were different among patients with ELVO who arrived at our hospital directly, those transferred from a primary stroke center, or those who had in-hospital onset. Therefore, only patients with ELVO who came to our hospital directly (n=180: 71 women; median age 76 (69–84) years; NIHSS score 17) were included in the present study.
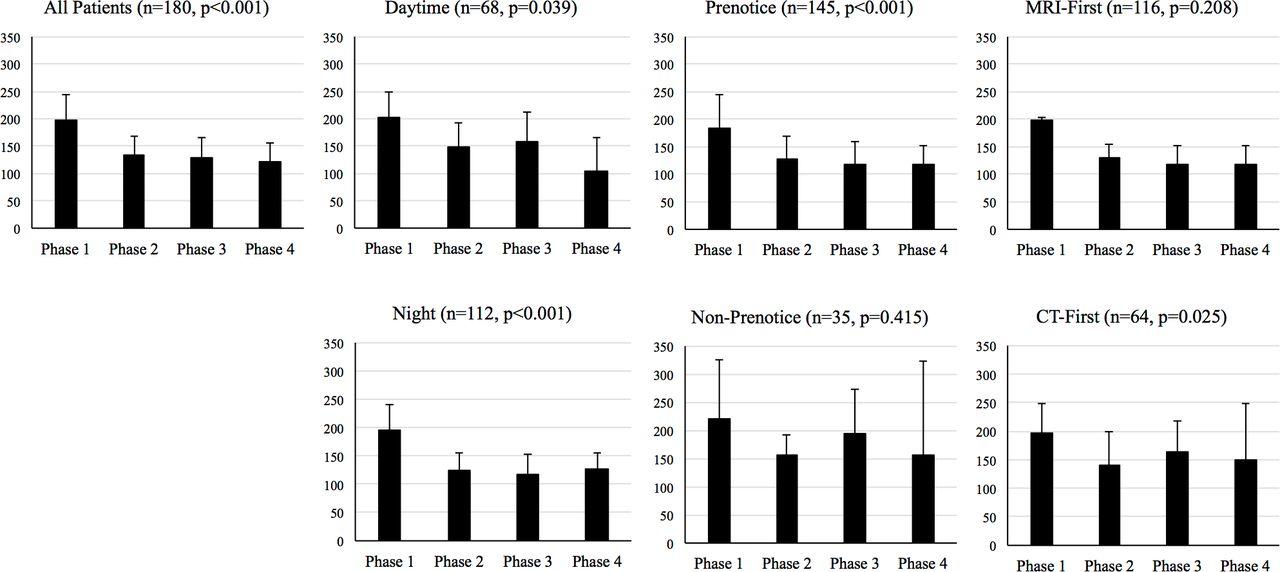
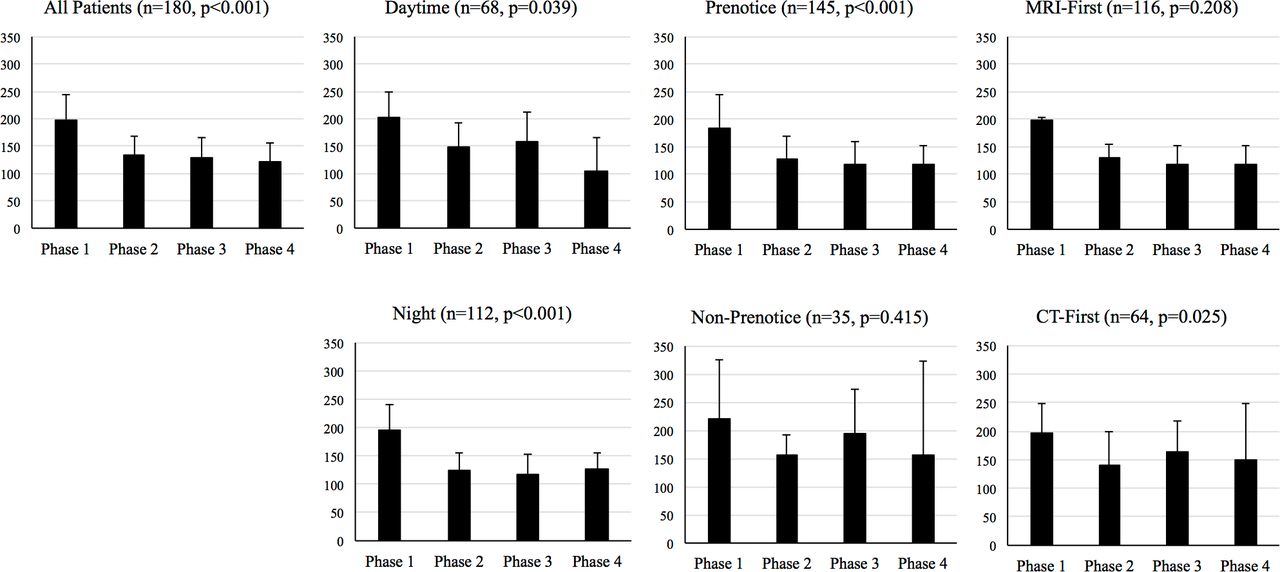
Table 2 shows the clinical background characteristics of the included patients. Sex, age, the rates of EMS pre-notification and of patients who arrived at the ED during office hours, and ODT did not differ between the four phases. In the late phase, fewer patients had major artery occlusion (p=0.002) and cardioembolic stroke (p=0.025). More patients were managed with the MRI-first policy in the late phase (p<0.001). The main reason for not following the MRI-first policy, especially in the early phase, was the unavailability of MRI due to examining other patients. There was no adverse event due to an MRI-first policy, such as a metal absorption-associated accident. DRT was significantly decreased across the phases (199 min in Phase 1, 135 min in Phase 2, 129 min in Phase 3, and 121 min in Phase 4, p<0.001, figure 1). Both IPT (p<0.001) and PRT (p=0.003) decreased across the phases: IPT and PRT in Phase 4 were roughly half of those in Phase 1. The percentage of patients with DRT <90 min or DRT <120 min increased across the time periods, especially DRT <120 min (4% in Phase 1, 37% in Phase 2, 49% in Phase 3, and 50% in Phase 4, p<0.001). sICH did not increase across the phases (p=0.575). These results in time metrics did not change significantly even when only patients with successful reperfusion (n=146) were evaluated.
{kind=link}
Door-to-reperfusion time (black boxes) in phases 1–4 according to various subgroups. Boxes and bars show median values and IQR.
Clinical characteristics of the included patients
Figure 1 shows DRT in several subgroups. DRT decreased irrespective of arrival time or first imaging modality. However, in patients with ELVO without pre-notification by EMS, DRT did not change across the phases. DRT in patients screened using MRI seemed to decrease, but the reduction was not statistically significant (p=0.208), probably due to the extremely small number of MRI-screened patients in Phase 1 (table 2). On multiple linear regression analysis, EMS pre-notification (standardized coefficient −0.409, p<0.001), ODT (standardized coefficient 0.256 per 60 min increase, p=0.001), and cardioembolism (standardized coefficient −0.175, p=0.026) were the independent predictors of DRT in Phases 3 and 4 (table 3). There were no variables with a variance inflation factor (indicator of multicollinearity) >2.
Multiple linear regression analysis for independent predictors of the door-to-reperfusion time in phases 3 and 4
Discussion
The results of the present study show that an MRI-first policy for patients suspected of having acute stroke is feasible. In addition, a step-by-step QI process decreased DRT. Although the QI process effectively reduced DRT in most patients with ELVO, there seemed to be room for improvement for patients without EMS pre-notification.
The feasibility of an MRI-first policy for patients with suspected acute stroke and ELVO in a tertiary general academic teaching hospital is not well known, probably because few institutions perform MRI as an initial examination for patients with suspected acute stroke.21 An MRI-first policy was feasible; more than 80% of the included patients were screened with MRI, and half of those were treated with EVT <120 min after arrival in Phase 4 of the present study. Moreover, time metrics such as DPT were comparable to those of a real-world multicenter registry.22 An MRI-first policy could be adopted without an increment in serious adverse events or time metrics about EVT.
MRI takes a slightly longer time than CT,23 but it clearly depicts the extent of the ischemic lesion on DWI. DWI can delineate small and/or brainstem lesions. In this respect MRI is superior to CT, especially in hospitals where various levels of physicians may manage patients with suspected hyperacute ischemic stroke, as in our institution. Moreover, MRA can show the site of arterial occlusion without contrast medium injection, and this is a huge advantage of MRI, particularly in Japan because written consent is generally needed before using contrast medium in Japan. For patients with hyperacute stroke, DWI hyperintensity brings an accurate and clear diagnosis of ischemic stroke and plain radiological indications and contraindications for EVT. Indeed, the rate of sICH was gradually reduced from 11.5% in Phase 1 to 3.6% in Phase 4, which may have been in part because the ratio of patients screened by MRI increased (8% in Phase 1 through 82% in Phase 4).
DRT was decreased by 78 min with a step-by-step QI approach. This result was in line with past studies which showed that a QI process could shorten DRT using CT as a screening modality,6 7 but there are few reports on reducing DRT using MRI as a screening modality. Moreover, the DRT reduction was recorded in most subgroups, including both during and outside office hours. The time metrics of EVT were longer outside office hours than during office hours in past reports,24 25 and a systematic protocol reduced DRT but had no effect outside office hours.8 26 Screening of patients by a vascular neurology fellow or attending neurologist both during and outside office hours, along with a step-by-step approach, may facilitate shortening DRT in various scenarios in large hospitals.
EMS pre-notification was an independent predictor for DRT, and DRT in patients without EMS pre-notification did not decrease over time. The reason for the lack of improvement is clear, as such patients come to hospital by themselves or with EMS, are examined first by doctors in the ED or physicians from a department other than neurology, and then neurologists are called. DRT in patients with ELVO without pre-notification tended to be longest among various subgroups (figure 1); therefore, education and explanation of symptoms suggestive of ELVO19 or rapid response to possible ELVO cases by EMS or all staff in the ED is critically and urgently needed.
This study has some limitations that need to be addressed. First, the DRT in patients screened using MRI did not change during the study period, and the ideal DRT could not be achieved when MRI was used as a first-line screening modality, at least with the protocol used in the present study. Although the time metrics in the present study were comparable to a real-world registry,22 our workflow may need further improvements. Second, the present study is a retrospective study from a prospective real-world registry, and all the patients who arrived directly at the hospital and received emergent EVT were recruited from the registry. Patients with acute stroke outside the definite evidence (late time window, distal artery occlusion, or posterior circulation stroke) were also included, especially in the late phase. In addition, the proportion of patients treated with stent retrievers was not high (50% even in Phase 4), and modern automated post-processing software (such as RAPID) is not adopted in our institution. DRT between Phases 3 and 4 or functional outcome 3 months after stroke did not improve in the present study, probably due to such limitations. Third, the number of patients included in the present study was relatively small. Some subgroup analyses (especially patients screened with MRI) may be statistically underpowered due to the small number of subgroup patients. Fourth, the hardware had also changed during the study period (the stroke unit was opened during Phase 1). The QI process included an intervention for stroke care, the MRI acquisition protocol, and patient logistics. In addition, the number of EVT procedures increased steeply during the study period (from 1.6/month to 9.3/month). DRT reduction in the present study should be achieved by these changes,27 but the present study could not analyze these effects separately. Fifth, the present study was conducted in a single tertiary general academic teaching hospital, and its results may not be generalizable to all hospitals.
Conclusion
An MRI-first policy was feasible in a tertiary general academic teaching hospital. DRT was decreased substantially in most subgroups with a step-by-step QI process, probably along with an increment in the number of EVT procedures per month. Notification regarding patients with suspected ELVO both in the pre-hospital and in-hospital stage is needed for further DRT reduction and patient benefit.
Acknowledgments
The authors would like to express their deepest gratitude to all members of the stroke unit and radiology and emergency departments. They would also like to thank Chie Ushiki for her assistance with database registration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YS framed the study concept, collected data, wrote and revised this manuscript. KS, AA, JA, TK, YT, TK, and AK performed the endovascular procedure, collected data, and offered scientific advice. SS, YN, and CN offered scientific advice for the concept, data collection, and interpreting data. KK offered scientific advice for the concept, data collection, interpreting data, and revision of the manuscript.
Funding This work was partly supported by JSPS KAKENHI Grant Number JP19K23985.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.