Article Text

Abstract
Background The dual-layer nitinol CASPER stent was designed to prevent plaque prolapse into its strut and periprocedural stroke.
Objective To conduct a clinical trial for government approval of the device in patients at either high or normal risk for carotid endarterectomy (CEA).
Methods Eligible patients had ≥50% symptomatic stenosis or ≥80% asymptomatic stenosis according to the North American Symptomatic Carotid Endarterectomy Trial methods (peak systolic velocity 130 and 230 cm/s on ultrasonography, respectively). The primary endpoint was the lack of major adverse events (MAEs), defined as death, stroke, and myocardial infarction within 30 days, and ipsilateral stroke within 1 year. The performance goal was set at 90.5%. MAE rates were also compared between the CEA high- and normal-risk groups.
Results 140 carotid artery stenting procedures, including 40% of patients at high risk and 60% at normal risk for CEA, were performed in 13 institutes. MAEs occurred in two cases (one intraprocedural and one postprocedural stroke), and the MAE rate was 1.4%. The non-MAE rate was 98.6% according to Kaplan-Meier analysis, which was superior to the previously set performance goal. The deployment success, target lesion revascularization (TLR), in-stent restenosis, and cerebrovascular event rates were 99.3%, 2.4%, 8.5%, and 7.2%, respectively. The MAE rate in patients with normal CEA risk was 1.2%, which was similar to the high-risk CEA group, with no significant difference due to the small number of MAEs.
Conclusions The MAE rate following use of the CASPER stent was low (1.4%). The MAE, deployment success, TLR, in-stenosis, and cerebrovascular event rates were similar to those of previous reports.
- angioplasty
- cervical
- stent
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Carotid artery stenting (CAS) was reported not to be inferior to carotid endarterectomy (CEA) in a large randomized controlled trial (RCT) in 20041 ; however, only patients with carotid stenosis considered to be high risk for CEA were eligible for this Stent and Angioplasty with Protection in Patients at High Risk for Endarterectomy (SAPPHIRE) trial. Of the devices employed in this study, both the Precise stent and Angioguard XP have previously been widely used for patients at high surgical risk with carotid artery stenosis. In 2010, the Carotid Revascularization Endarterectomy vs Stenting Trial (CREST) trial, conducted in patients without high risk for CEA,2 also found that the primary endpoint of CAS was not inferior to CEA, as in the SAPPHIRE trial. However other RCTs for CEA normal-risk patients, such as the SPACE,3 EVA-3S,4 and ICSS5 trials, failed to detect non-inferiority of CAS to CEA. Moreover, the primary endpoint in the SAPPHIRE and CREST trials, which demonstrated that CAS was not inferior to CEA, was the composite outcome of stroke, myocardial infarction (MI), and death; CAS was associated with a high risk of stroke and CEA had a high risk of MI. Given that about 30% of periprocedural strokes in the CREST trial occurred between days 1 and 30, these findings indicate that periprocedural stroke needs to be reduced in order to expand the indications of CAS, with the development of appropriate embolic prophylaxis and both intraprocedural and postprocedural stents.
The CASPER stent has a unique structure involving a dual-layer nitinol stent, with an outer layer suitable for close apposition and an inner layer to prevent plaque protrusion. We conducted a multicenter clinical trial to determine the ability of this stent to reduce periprocedural distal embolism in patients at high or normal risk for CEA. The study aimed to demonstrate the effectiveness and safety of the CASPER stent in patients at high and normal risk for CEA.
Methods
CASPER (TCD-15152) stent
The CASPER (TCD-15152) stent (Terumo Co., Tokyo, Japan) is a self-expandable nitinol stent with a dual-layer structure of tubular mesh. The outer layer consists of a braided closed-cell structure with close vessel wall apposition and good conformability, and the inner layer has a closed-cell design with a very small micromesh to limit plaque prolapse and embolic release. The two layers are connected by spirally woven tantalum wire.
Study design
This clinical trial was conducted at 13 highly experienced Japanese institutions between July 2016 and December 2017, with a planned number of cases of at least 138. The primary investigators had experience of at least 100 cases of CAS each. Eligible patients had ≥50% symptomatic stenosis resulting in ischemic stroke, transient ischemic attack (TIA), or amaurosis fugax within 180 days, or ≥80% asymptomatic stenosis, according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) methods. Instead of the NASCET method, we used carotid ultrasonography with peak systolic velocity 130 and 230 cm/s indicating 50% and 80% stenosis, respectively. The inclusion criteria were as follows: age ≥20 years; common carotid artery or internal carotid artery stenosis; target vessel diameter 3.5–9.0 mm; treatable by only one stent; possible to use any protection device; not pregnant; and written informed consent provided. The exclusion criteria were as follows life expectancy <1 year; premorbid modified Rankin Scale score ≥3; platelet count <1 00 000/mm3; heparin-induced thrombocytopenia type II, hypercoagulability with possibility of active bleeding, or patient unable to receive blood transfusion; allergy against the drugs and devices used, such as heparin, contrast medium, antiplatelet drug, and nitinol; severe renal or hepatic failure, or malignant hypertension; previous stent or graft placement in the target vessels; calcification or tortuosity resulting in difficult access; intracranial hemorrhage within 90 days; stroke or contralateral carotid stenosis to treat within 30 days; MI within 72 hours; mobile thrombus, occlusion, or string sign in the target vessel; tandem lesion; and mobile plaque or thrombus in the aortic arch.
This trial was registered with Pharmaceuticals and Medical Devices Agency as TCD-15152 and University Hospital Medical Information Network as UMIN000023562.
Procedure
Dual antiplatelet management was mandatory from day 5 before CAS to day 30 after CAS, followed by single antiplatelet administration. Although there were no limitations regarding predilatation and postdilatation, only one CASPER stent was used in each case and any protective devices were used simultaneously. We recommended using a stent that had a diameter that was 1 or 2 mm larger than that of the referenced vessel. The activated coagulation time was maintained such that it was over 250 s via bolus administration of heparin during the entire procedure.
Endpoints
Major adverse events (MAEs) were defined as the composite of death, stroke, or MI within 30 days, or ipsilateral stroke within 1 year after the procedure. The primary endpoint was the rate of non-MAEs. Secondary efficacy endpoints were treatment success, deployment success, and non-target lesion revascularization (TLR) rate. In this study, treatment success was defined as the target vessel treated by one CASPER stent with a stenosis degree ≤30% immediately after stenting by the NASCET method, and no MAE before discharge. Deployment success was defined as placement of the CASPER stent at the planned position and withdrawal. TLR was defined as an additional treatment such as revascularization, stenting, CEA, thrombolysis, and open surgery within 5 mm proximal or distal to the placed position. The secondary safety endpoints were as follows: adverse event (severe, important); device malfunction; in-stent restenosis (defined as ≥50% stenosis on angiography and ultrasonography between 5 mm proximal and 5 mm distal to placed stent); neurological death; cerebrovascular event (severe and mild stroke, TIA); and cranial nerve palsy.
Statistical analysis
All the results except for the frequency of adverse events, device malfunction, cranial nerve palsy, and deployment success, were analyzed using the Kaplan-Meier method and Greenwood’s formula. The performance goal was set at 90.5% based on the previous report of CEA and CAS with an MAE rate of about 6.5%,1 2 the difference in outcomes between CEA and medical treatment, and the clinical results of the approved devices. The main purpose of this trial was to demonstrate that the non-MAE rate of the CASPER stent was superior to this performance goal. We also compared non-MAE rates in subgroups according to age, CEA risk, and previous symptoms, and degree of stenosis in symptomatic cases. Patients with a high risk of CEA were defined as those who met at least one of the following criteria: congestive heart failure (class III/IV) and/or severe left dysfunction with left ventricle ejection fraction <30%; MI within 4 weeks; angina (Canadian Cardiovascular Society class III/IV); at least two coronary diseases with ≥70% stenosis and a history of angina; severe pulmonary disease (long-term oxygen therapy, rest partial pressure of oxygen ≤60 mm Hg, hematocrit ≥50%, or forced expiratory volume or carbon monoxide transfer factor ≤50% normal value); contralateral internal carotid artery occlusion; contralateral laryngeal paralysis; cervical spine ankyloses; tracheal fistula; postirradiation therapy; severe tandem lesion; restenosis after CEA; high or low position; and age ≥80 years.
Results
We obtained informed consent from 163 patients, of whom 140 met all the criteria and were finally registered and underwent CAS using a CASPER stent. The background and lesion characteristics of these 140 patients are shown in table 1. A total of 39.3% of patients were symptomatic, and CAS was performed following ischemic stroke in 32 cases, TIA in 13, and amaurosis fugax in 12 cases; 39.3% of them were in the high-risk group for CEA and the remaining 60.7% were in the normal-risk group.
Demographic backgrounds and lesion characteristics of the 140 enrolled patients
The CASPER device was placed using a protection device in all patients (table 1), including a distal balloon protection device (Carotid GuardWire PS; Medtronic Irvine, California, USA) in 57.1% of cases, a distal filter device (eg, FilterWire EZ; Stryker, Fremont, California, USA) in 17.9% of cases, and a proximal balloon protection device (Mo.Ma Ultra; Medtronic Irvine) in 5.7% of cases. Multiple protection devices (eg, Carotid GuardWire PS and Mo.Ma Ultra) were used in 19.3% of cases (table 1). The used stent was 6×30 mm in 0.7%, 7×25 mm in 2.9%, 7×30 mm in 1.4%, 8×20 mm in 6.4%, 8×25 mm in 7.9%, 8×30 mm in 21.4%, 8×40 mm in 3.6%, 9×20 mm in 8.6%, 9×30 mm in 25.7%, 10×20 mm in 3.6%, and 10×30 mm in 17.9%. Stents that were 5×20 mm, 5×30 mm, 5×40 mm, 6×16 mm, 6×25 mm, and 7×18 mm were not used.
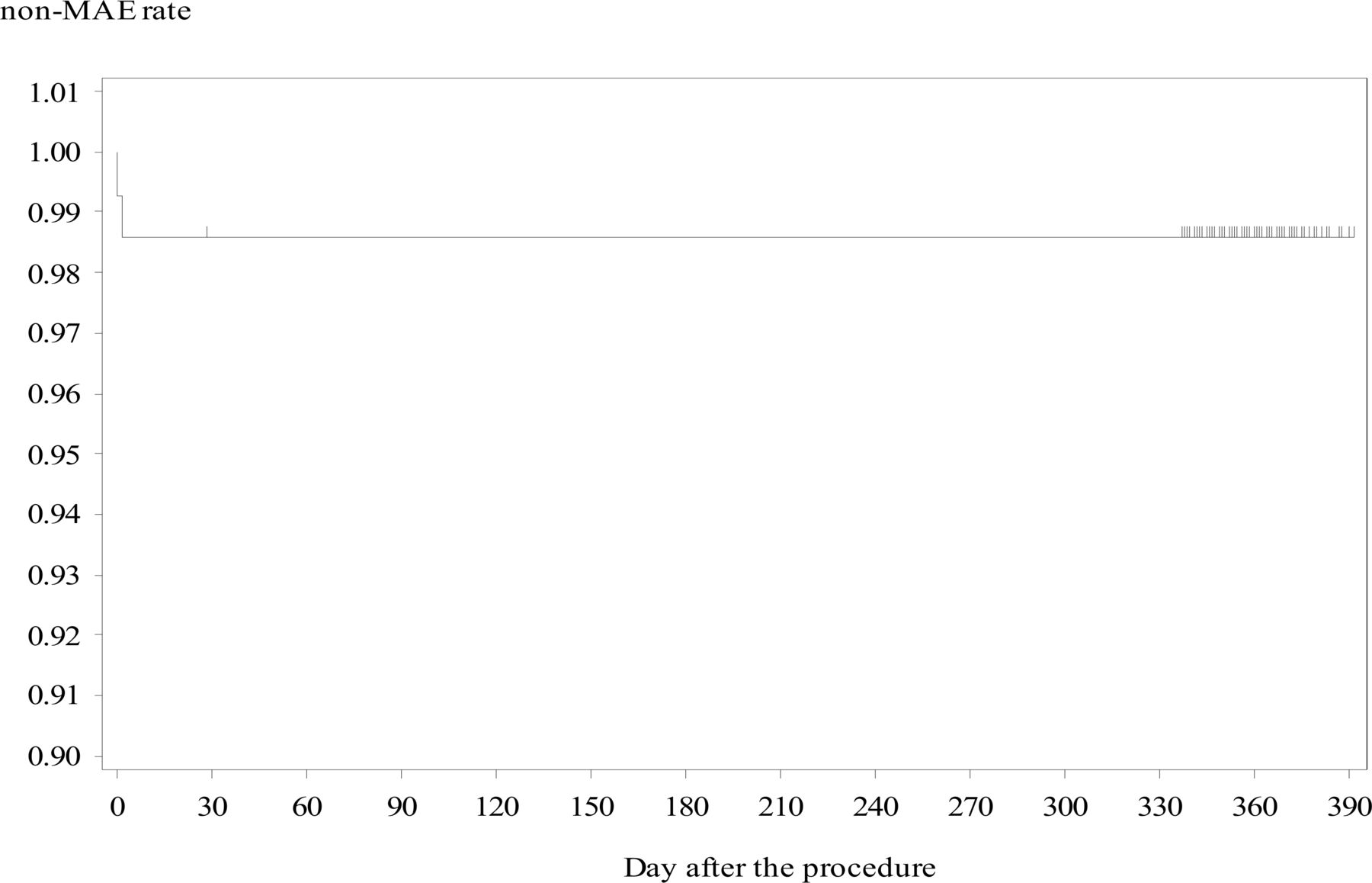
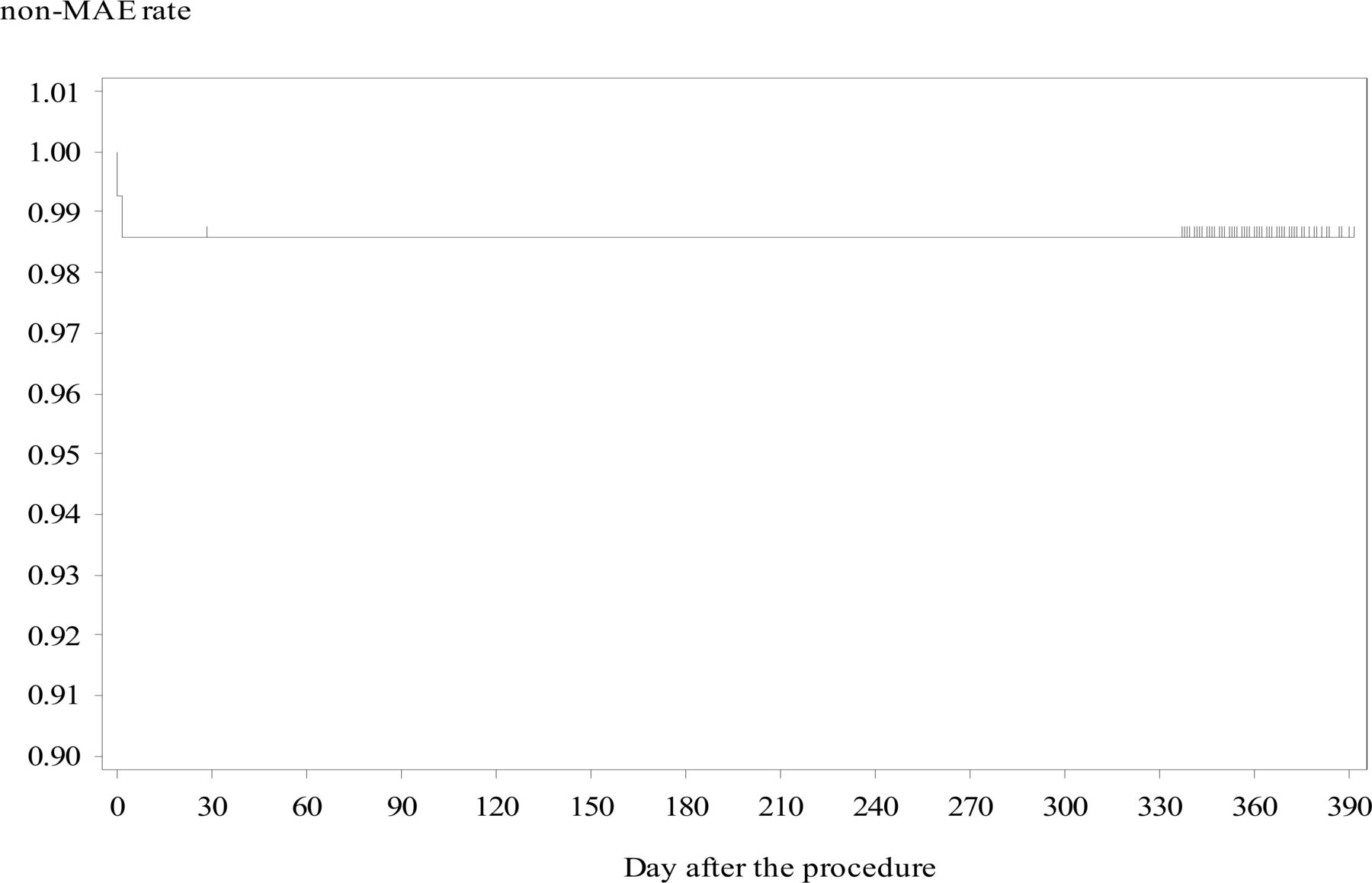
The deployment of the CASPER stent was successful in 99.3% of cases, except for one case in which it was accidentally placed distal to the planned position and an additional stent was needed (table 2). MAEs occurred in only two cases. Left hemiparesis occurred immediately after stent deployment in one, and the responsible infarction was revealed in the right frontal and occipital lobe. The procedure was completed without complications in the other, but the patient presented with left hemiparesis 1 day after CAS, and carotid ultrasonography revealed plaque protrusion within the stent, requiring additional stenting with percutaneous transluminal angioplasty the same day. There were no reports of death or MI within 30 days, and no ipsilateral stroke within 1 year after the procedure. The primary endpoint of non-MAE rate was 98.6% (95% CI 94.4% to 99.6%) (figure 1) according to the Kaplan–Meier method, which was superior to the predetermined performance goal of 90.5%.
{kind=link}
Kaplan-Meier analysis of non-major adverse events (MAE) rate. MAEs, including one intraprocedural stroke and one postprocedural stroke, occurred in two cases. The non-MAE rate was 98.6% (95% CI 94.4% to 99.6%).
Endpoints in all patients
The treatment success rate was 87.9%. The goal of the procedure was not achieved in 17 cases, including one with unsuccessful deployment and two cases with MAEs, as noted above. The degree of stenosis immediately after stenting by the NASCET method was >30% (95% CI 30.4% to 44.2%) in the remaining 14 cases. The TLR rate was 2.4%, and additional treatments were performed 180–365 days after stent placement in two cases and 1 day after in one case (table 2).
There were no reports of death or device malfunction during the trial period. Cerebrovascular events occurred in 7.2% of cases according to Kaplan-Meier analysis, including ischemic stroke and TIA in 2 (1.4%) and 8 (5.7%) cases, respectively. Severe stroke resulting in neurological symptoms lasting >7 days and deterioration of the National Institutes of Health Stroke Scale (NIHSS) score ≥4 occurred on the day of the procedure in one case (0.7%). Minor stroke, which resolved within 7 days or presented with a deterioration in NIHSS score <4, was encountered within 1–30 days in one case (0.7%). No instances of ipsilateral stroke were recorded between 30 days and 1 year. TIAs occurred at any time, with 2 (1.4%), 3 (2.1%), and 3 (2.1%) TIAs occurring on the day of CAS, within 1–30 days, and between 30 days and 1 year, respectively (table 3). One patient had cranial nerve palsy, but this was a bilateral facial palsy unrelated to the stenting. No in-stent restenosis was revealed up to 30 days after the procedure, but occurred in two (1.4%) and 11 (8.5%) cases by 180 and 365 days, respectively. However, there was no carotid ultrasonography or angiography data in one case and ultrasonography but no angiography data in three cases, and these four cases were therefore classified in the in-stent restenosis group (table 2).
Summary of cases with adverse events
We also analyzed MAEs in relation to age, CEA risk, and preprocedural symptoms, and degree of stenosis in symptomatic lesions. There was no significant difference in MAEs between patients aged <70 years and ≥70 years, or between patients with symptomatic and asymptomatic lesions. We also compared MAEs between the CEA high-risk and CEA-normal risk groups. There was no significant difference in non-MAE rates between the normal-risk (98.8%, 1/85 cases) and high-risk groups (98.2%, 1/55 cases; online supplemental figure 1). The non-MAE rates in patients with <50%, 50–690%, and ≥70% symptomatic stenosis were 85.7%, 100.0%, and 100.0%, respectively. MAEs occurred only in one symptomatic patient in the <50% stenosis group, and there was no significant difference among these groups (table 4).
Supplemental material
Subgroup analyses of non-MAE occurrence
Discussion
Commonly used carotid artery stents involve a monolayer open-cell or closed-cell structure. In contrast, the CASPER stent used in the current trial was unique and was designed to prevent plaque protrusion and reduce distal emboli during the procedure. Although a large meta-analysis revealed no correlation between stent design and intraprocedural MAEs, postprocedural diffusion-weighted imaging detected subclinical ischemic lesions.6 In general, closed-cell stents such as the Carotid Wallstent have a smaller cell size and less plaque protrusion through the stent struts than open-cell stents.7 On the other hand, open-cell stents have better wall apposition8 and less thrombus formation outside the placed stent. The CASPER stent was expected to provide close apposition to the vessel wall as a result of its soft braided-nitinol outer layer, and less plaque prolapse due to the micromesh design of the inner layer with very small cell size. Use of Roadsaver, which is identical to the CASPER stent, has been reported in the CLEAR-ROAD study, which found an MAE rate of only 2%, but no intraprocedural stroke despite the use of protection devices in only 60% of cases.9 Overall, these previous and current results suggest that the CASPER stent is safe.
The MAE rate in the current trial was 1.4%, which was lower than in previous studies,1–5 10 and notably lower than in past RCTs that failed to demonstrate inferiority of CAS to CEA.3–5 This difference might be due to this newly designed stent, or because the trial was conducted at highly experienced and limited institutions, or due to differences in the use of protection devices among these studies; in the current trial, all patients received some protection device, as they did in the SAPPHIRE, CREST, and ACT-1 trials. Although the use of protection devices for CAS is acknowledged, the optimal method of protection remains unclear.11–15 Ongoing studies are examining this question, and the results of CAS combined with some protection have recently been reported.16 17 In addition, more studies are needed to evaluate the effects of the patient’s background or lesion characteristics on the appropriate choice of device. However, the incidence of strokes, especially minor strokes, was slightly more frequent in the current study than found with CEA, and developments, such as improved stent structure, are required to reduce the incidence of MAEs.
In this study, no instances of ipsilateral stroke, and only three TIAs (2.1%) occurred between 30 days and 1 year after the procedure. However, the CLEAR-ROAD study reported the rate of ipsilateral stroke to be 4.2% at a 12- month follow-up assessment. Although 1 month of dual antiplatelet therapy after the procedure was recommended in both studies, it continued for 6 months after CAS in over 60% of the patients in the current study. This may explain the difference between the two studies. As reported by Brousssalis et al,18 slightly longer-term dual antiplatelet therapy should be recommended after CAS using a CASPER stent. Considering the double-mesh stent structure with a large amount of metal, periprocedural dual antiplatelet therapy should be carefully conducted, and platelet function testing may be necessary. In the present study, eight TIAs occurred from the day of the procedure to day 307. There were no instances of in-stent restenosis in these eight cases. Although TIA occurred in three cases between 30 days and 1 year after the intervention, one of these patients did not take any antiplatelet drugs and one patient presented with arrhythmia.
In contrast to the CLEAR-ROAD and SAPPHIRE studies, the present trial included patients with normal CEA risk. The American Heart Association/American Stroke Association recommend CEA in patients with low risk of perioperative stroke, MI, and death,19 but because of its less invasive nature, the indication for CAS should ideally be expanded to include patients at normal risk of CEA. Only one MAE occurred in patients in the normal CEA risk group in our trial. It is important to demonstrate the superior or equivalent effectiveness of CAS in the current study and in the CREST, ACT-1, and ongoing CREST-2 trials, in which the target patients were considered to be CEA normal risk.20 21
Plaque prolapse into the stent is a risk factor for ipsilateral stroke both during and after the procedure, and in-stent protrusion was reported to be associated with postprocedural ischemic events.22 23 Slight in-stent protrusion was detected in the present trial, resulting in stroke 1 day after stenting. The closed-cell stent-in-stent technique has been reported to prevent plaque protrusion and postprocedural ischemia, even in patients with unstable stenosis.24 25 In this regard, the dual-layer structure of the CASPER stent could reduce postoperative ischemic events with no increase in periprocedural complications, because of its easier placement compared with the stent-in-stent technique. However, more evidence from studies using dual-layer carotid stents is needed.
In-stent restenosis is a concern for dual-layer stents because of the larger volume of metal compared with the usual single-layer stent. In the current trial, in-stent restenosis occurred in 8.5% of cases, and percutaneous transluminal angioplasty was performed as a TLR in two cases. No neurological symptoms were seen in any cases. Although the stenosis threshold was strict, the rate of in-stent restenosis (>50%) in the past report was 1.6–8.0%,26–28 which was similar to the present study. Additionally, the TLR rate was only 2.4%, which was also similar to the SAPPHIRE trial and CLEAR-ROAD study.29 Cilostazol has been found to be beneficial for reducing restenosis after carotid and coronary stenting.30 31 However, cilostazol was not administered in 10 of the 11 patients who exhibited restenosis in this study.
This study had some limitations. First, this was a single-armed study. We did not compare CAS and CEA in patients with normal CEA risk directly, although the MAE rates were similar in the high- and normal-risk groups. Second, the number of registered cases (n=140) was small because this was a government approval study. The number of MAEs was therefore too small to perform a subanalysis of MAE occurrence. More cases are also needed for postmarket surveillance of the comparison between patients with high and normal CEA risk. Moreover, we could not evaluate the association between ischemic events and plaque morphology. Finally, the follow-up period was short (1 year), and longer observation is needed to confirm the efficacy and safety of this new dual-layer micromesh stent accurately.
Conclusions
The current clinical trial of the dual-layer, self-expandable nitinol CASPER stent showed good results, with similar safety to results in previous reports. All the measured endpoints, including rates of deployment success, TLR, in-stent restenosis, and periprocedural and postprocedural ischemic events were acceptable. The MAE rates were comparable between patients at high and normal CEA risk, but this was probably due to the small sample size.
Acknowledgments
We thank the following investigators: Investigators (study center; name of physician) Kohnan Hospital; Yasushi Matsumoto Juntendo University Hospital; Hidenori Oishi Showa University Fujigaoka Hospital; Tomoaki Terada Kyoto University Hospital; Akira Ishii National Hospital Organization Osaka National Hospital; Toshiyuki Fujinaka National Cerebral and Cardiovascular Center Hospital; Hiroshi Yamagami Kobe City Medical Center General Hospital; Nobuyuki Sakai Okayama University Hospital; Kenji Sugiu Kyushu University Hospital; Koji Iihara Fukuoka University Chikushi Hospital; Toshio Higashi University of Tsukuba Hospital; Yuji Matsumaru Hyogo College of Medicine Hospital; Shinichi Yoshimura Nagoya University Hospital; Takashi Izumi Investigators (consultant, image evaluation, safety evaluation) Toyama University Hospital; Naoya Kuwayama Shinrakuen Hospital; Yasushi Ito Iwate Medical University Hospital; Kuniaki Ogasawara Dokkyo Medical University Saitama Medical Center; Akio Hyodo Toho University Medical Center Ohashi Hospital; Masato Nakamura We also thank Susan Furness, PhD, from Edanz Group (https://en-author-services.edanzgroup.com/) for editing a draft of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published Online First. The Non-MAE rate in Table 2 was corrected to 98.6%.
Contributors HI: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work. NS and others: revising the manuscript critically for important intellectual content.
Funding This clinical trial and study were funded and supported by Terumo Corporation (Tokyo, Japan). This trial was registered with Pharmaceuticals and Medical Devices Agency as TCD-15152 and University Hospital Medical Information Network as UMIN000023562.
Disclaimer All authors who are members of the Japanese Society for Neuroendovascular Therapy (JSNET) have registered online self-reported conflicts of interest disclosure statement forms through the website for JSNET members.
Competing interests HI received speakers’ bureau/honoraria from Medtronic Japan Co. and Stryker Japan Co. NS received speakers’ bureau/honoraria and research funding from Terumo Co. YM received speakers’ bureau/honoraria from GE Healthcare Co, Stryker Co, Medico’s Hirata Co, Medtronic Japan Co, Century Medical Co, Takeda Pharmaceutical Co, Otsuka Pharmaceutical Co, and Fuji Systems Co. HY received speakers’ bureau/honoraria from JIMRO Co, Terumo Co, Johnson & Johnson Co, Medtronic Japan Co, Medico’s Hirata Co, and Stryker Japan Co. SY received speakers’ bureau/honoraria from Terumo Co, Boehringer-Ingelheim Co, Daiichi Sankyo Co, Bayer Co, Bristol-Meyers Squibb Co, Stryker Japan Co, Medtronic Japan Co, Johnson & Johnson Co, Kaneka Medics Co, Otsuka Pharmaceutical Co, Biomedical Solutions Co, and Sanofi Co. AI received speakers’ bureau/honoraria from Medtronic Japan Co, Stryker Japan Co, Daiichi Sankyo Co, Otsuka Pharmaceutical Co, and Kaneka Medics Co. HO received speakers’ research funding from Terumo Co. TH received speakers’ bureau/honoraria from Stryker Japan Co, Johnson & Johnson Co, Kaneka Medics Co, and Terumo Co, and research funding from Stryker Japan Co. and Medtronic Japan Co. KI received research funding from the Japan Agency for Medical Research and Development, grants-in-aid, the Japan Ministry of Health, Labor and Welfare, KAKENHI grant from the Japan Society for the Promotion of Science, Otsuka Pharmaceutical Co, Eisai Co, and Kaneka Medics Co.
Patient consent for publication Not required.
Ethics approval This study has been approved by the institutional review board of Kobe City Medical Center General Hospital (permission number: E-15152-31). All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.