Article Text

Abstract
Background Targeted eloquence-based tissue reperfusion within the primary motor cortex may have a differential effect on disability as compared with traditional volume-based (thrombolysis in cerebral infarction, TICI) reperfusion after endovascular thrombectomy (EVT) in the setting of acute ischemic stroke (AIS).
Methods We explored the impact of eloquent reperfusion (ER) within primary motor cortex (PMC) on clinical outcome (modified Rankin Scale, mRS) in AIS patients undergoing EVT. ER-PMC was defined as presence of flow on final digital subtraction angiography (DSA) within four main cortical branches, supplying the PMC (middle cerebral artery (MCA) – precentral, central, postcentral; anterior cerebral artery (ACA) – medial frontal branch arising from callosomarginal or pericallosal arteries) and graded as absent (0), partial (1), and complete (2). Prospectively collected data from two centers were analyzed. Multivariate analysis was conducted to assess the impact of ER-PMC on 90-day disability (mRS) among patients with anterior circulation occlusion who achieved partial reperfusion (TICI 2a and 2b).
Results Among the 125 patients who met the study criteria, ER-PMC distribution was: absent (0) in 19/125 (15.2%); partial (1) in 52/125 (41.6%), and complete (2) in 54/125 (43.2%). TICI 2b was achieved in 102/125 (81.6%) and ER-PMC was substantially higher in those patients (P<0.001). In multivariate analysis, in addition to age and symptomatic intracranial hemorrhage, ER-PMC had a profound independent impact on 90-day disability (OR 6.10, P=0.001 for ER-PMC 1 vs 0 and OR 9.87, P<0.001 for ER-PMC 2 vs 0), while the extent of total partial reperfusion (TICI 2b vs 2a) was not related to 90-day mRS.
Conclusions Eloquent PMC-tissue reperfusion is a key determinant of functional outcome, with a greater impact than volume-based (TICI) degree of partial reperfusion alone. PMC-targeted revascularization among patients with partial reperfusion may further diminish post-stroke disability after EVT.
- thrombectomy
- stroke
- angiography
- blood flow
- brain
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Endovascular therapy (EVT) has emerged as a widely adopted and clinically proven treatment of acute ischemic stroke (AIS) due to anterior circulation large vessel occlusion (LVO) circulation.1–7 The success of EVT relies on rapid and efficient reperfusion of the salvageable ischemic brain tissue after revascularization of the occluded vessel. Since the inception of the first thrombectomy trials, various angiographic grading scales have been used for evaluation of the degree of ischemic tissue reperfusion, including arterial occlusive lesion (AOL), thrombolysis of myocardial ischemia (TIMI), and thrombolysis of cerebral ischemia (TICI).8–11 Given the significant heterogeneity among these scales, an expert panel established TICI scoring as an optimal angiographic assessment of cerebral reperfusion therapies with successful recanalization defined as perfusion with >50% distal branch filling (TICI 2b).12 Further iterations and expansions of this grading scale, adapted from the coronary circulation scoring system (TIMI) and applied to quantify cerebral reperfusion, consistently demonstrated incremental correlation between functional independence and higher volume of distal antegrade contrast flow on angiography.13–17 However, this volume-based reperfusion assessment undermines the complex functional organization of the human brain and does not take into consideration reperfusion of eloquent vascular territories, especially in patients who achieve incomplete/partial revascularization (TICI 2a or 2b).
Multiple studies have demonstrated significant correlation between infarct location (particularly within motor pathways) and post-stroke disability, emphasizing the importance of corticospinal tract damage as a primary driver of functional motor recovery after stroke.18–24 These fundamental principles of vascular neurology may, in part, explain the reason why some patients with favorable mismatch profile remain disabled despite “successful” reperfusion. Furthermore, as evidenced by exhaustive neurosurgical literature, identification of “eloquent” brain regions is a well-proven and long-established method for prediction of neurologic outcome after intracranial interventions.25 As such, more detailed angiographic assessment of reperfusion within the most eloquent cerebral vasculature supplying the motor cortex may optimize prediction of disability after EVT. Another oversimplified and widely utilized scale for measuring post-stroke disability is the modified Rankin Scale (mRS), which is largely based on motor function.26 It is therefore logical to conclude that acute stroke treatments targeting reperfusion of the primary motor cortex (PMC) are likely to be the most significant determinant of functional outcome after EVT. Based on these neuroanatomical and functional concepts, we used a refined approach, aiming to assess the degree of reperfusion within the eloquent PMC in conjunction with the widely used volume-based reperfusion (TICI). We hypothesized that in patients with incomplete revascularization, targeted eloquence-based reperfusion (ER) assessment may have a more significant correlation with post-stroke disability as compared with the traditional TICI reperfusion grading.
Methods
Study population
We performed a retrospective analysis of a prospectively collected database of consecutive patients with AIS, treated with EVT from two hospitals between 2013 and 2018. All patients with anterior circulation LVO (internal carotid artery (ICA), M1 or M2 middle cerebral artery (MCA) occlusion), who achieved partial reperfusion (TICI 2a or 2b) after EVT were included. Eligibility for EVT was determined based on multidisciplinary consensus between vascular neurology and interventional neuroradiology teams. The study design and analyses were approved by the institutional review board of each facility.
Data collection
We collected demographic, clinical, and neuroimaging data from all eligible patients, including age, sex, pre-morbid mRS score, vascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, and smoking), admission National Institutes of Health Stroke Scale (NIHSS) scores, baseline Alberta Stroke Program Early Computed Tomography Score (ASPECTS), use of intravenous thrombolysis, neurologic outcome within 24 hours measured by the NIHSS, discharge mRS score, and 3-month mRS score. TICI scores were reported by the physician who performed the procedure and adjudicated by two independent readers, blinded to functional outcome. TICI 2b was defined as reperfusion within >50% of the ischemic territory.12
Eloquent motor cortex reperfusion assessment
Neuroangiographic imaging before and after EVT was available for all included patients. Eloquent motor cortex angiographic reperfusion assessment was performed by two independent readers who were blinded to functional outcome, followed by consensus adjudication. Lateral projection angiography was used to identify the central (Rolandic) arterial region corresponding to PMC location within the cerebral hemisphere.27 Antegrade perfusion in distal cortical branches was evaluated, irrelevant of proximal anatomic features and variations. Eloquent reperfusion (ER) was defined as presence of antegrade flow on final digital subtraction angiography (DSA) within four main cortical branches, supplying the PMC (MCA – precentral, central (aka Rolandic), postcentral (aka anterior parietal); anterior cerebral artery (ACA) – medial frontal branch arising from callosomarginal or pericallosal arteries).28 ER-PMC grading scale is described in detail in table 1.
Eloquent reperfusion-primary motor cortex (ER-PMC) grading
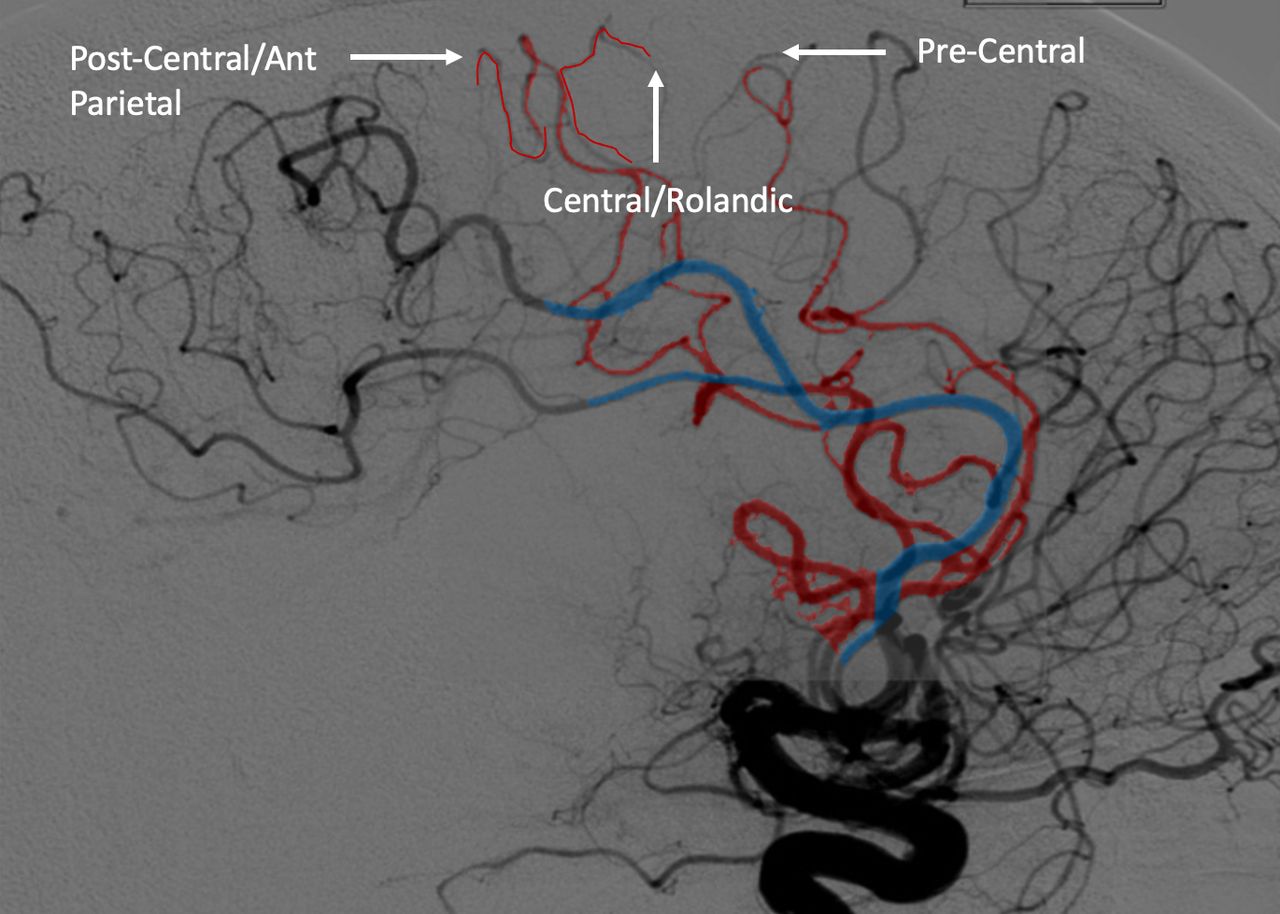
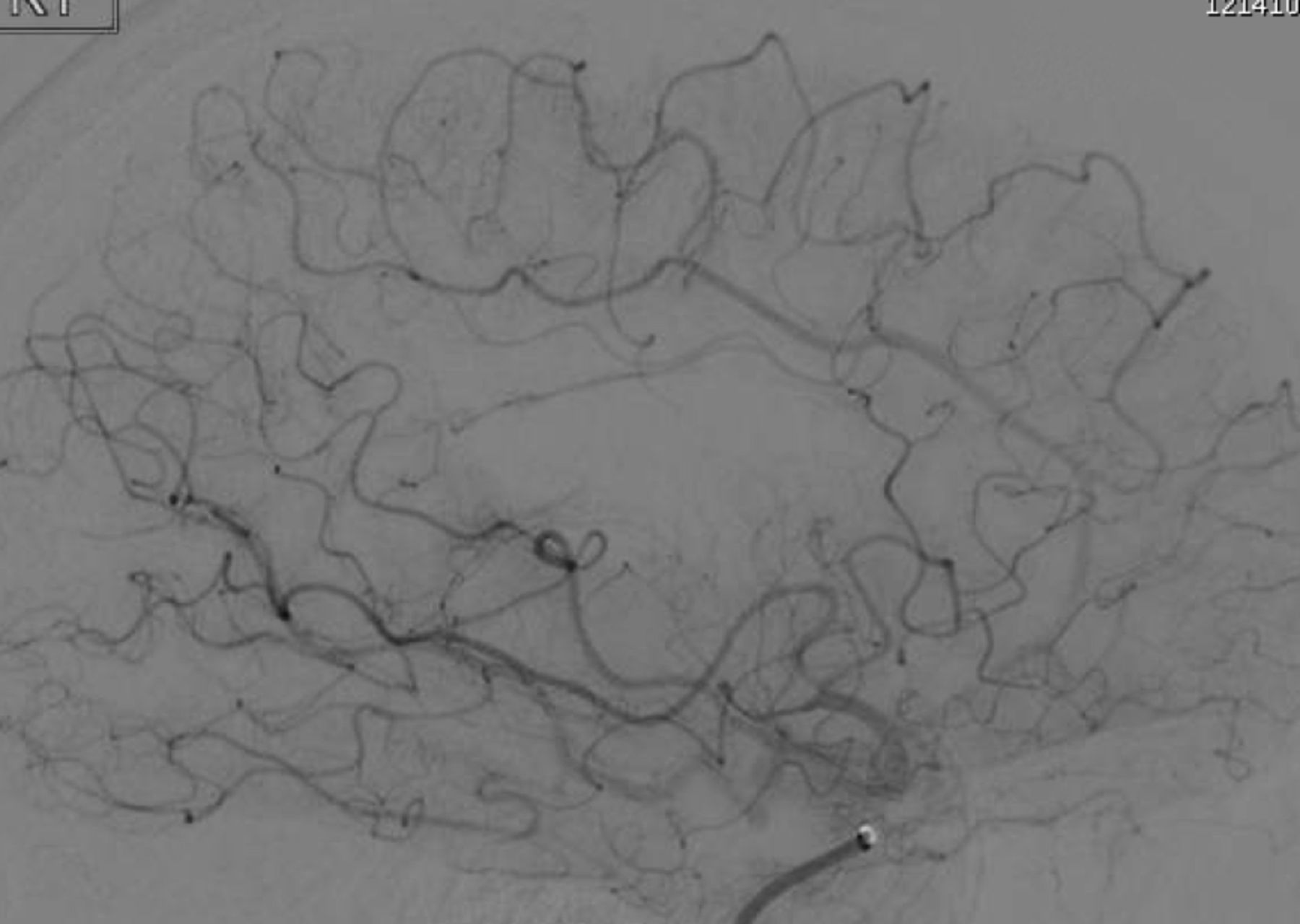
Examples of TICI 2a/ER-PMC 2, TICI 2b/ER-PMC 0, and TICI 2b/ER-PMC 1 are included in figures 1–3.

Example of patient with thrombolysis in cerebral infarction (TICI) 2a/eloquent reperfusion-primary motor cortex (ER-PMC) 2 after endovascular therapy for M1 occlusion. The middle cerebral artery (MCA) branches supplying the PMC are outlined in red, and the anterior cerebral artery (ACA) is outlined in blue. Patient had full motor recovery with mild residual difficulty with comprehension and short-term memory loss at 90 days (modified Rankin Scale (mRS) 1).

Example of patient with thrombolysis in cerebral infarction (TICI) 2b/eloquent reperfusion-primary motor cortex (ER-PMC) 0 after endovascular therapy for M1 occlusion. The PMC branches referenced in figure 1 are missing. Patient remained hemiplegic and wheelchair dependent at 90 days (modified Rankin Scale (mRS) 4).
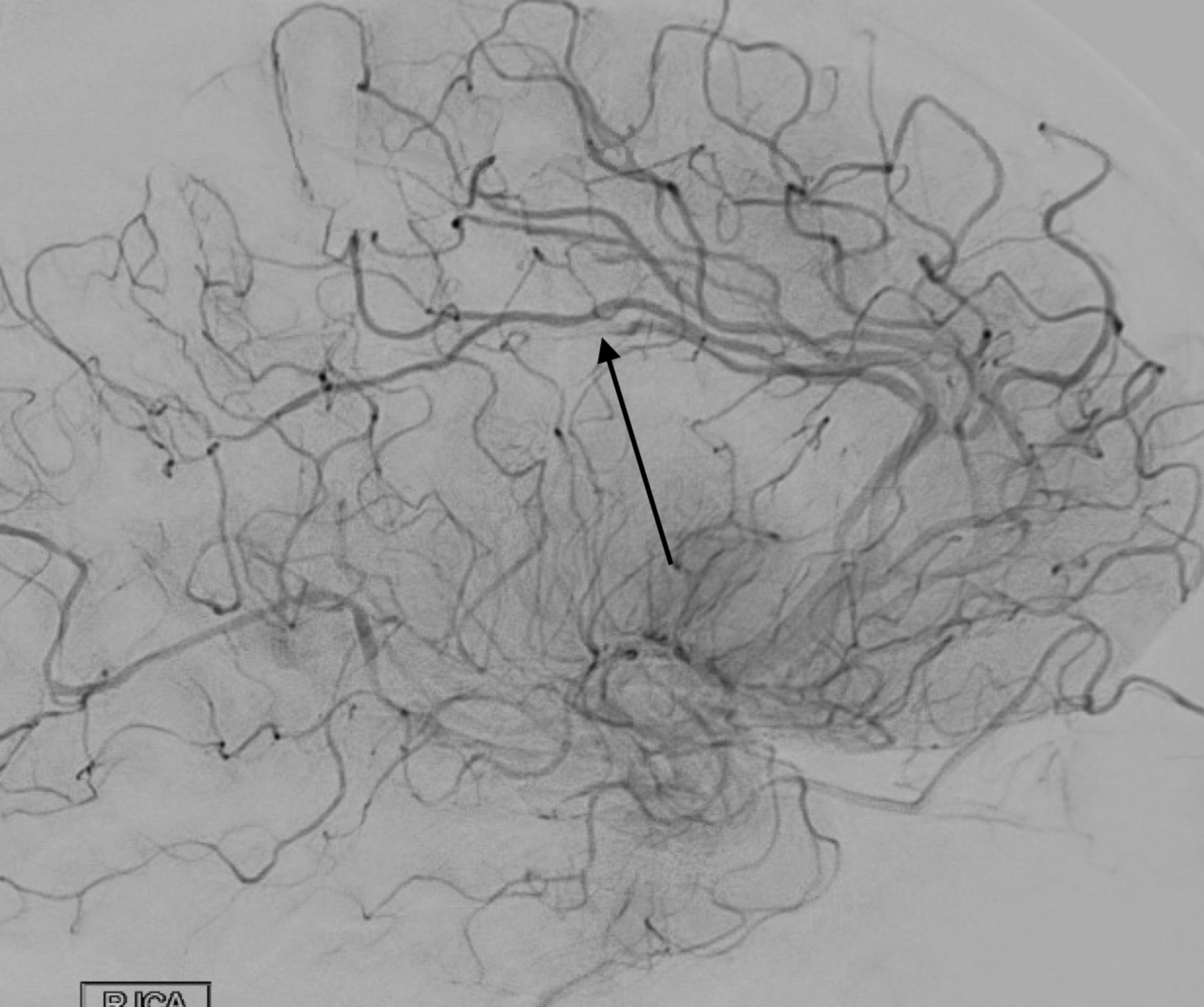
Example or patient with thrombolysis in cerebral infarction (TICI) 2b/eloquent reperfusion-primary motor cortex (ER-PMC)1 after endovascular therapy for internal carotid artery (ICA) T occlusion. All PMC middle cerebral artery (MCA) branches are patent, but there is a residual A3 occlusion (arrow). The patient had severe leg weakness and was unable to ambulate without assistance at 90 days (modified Rankin Scale (mRS) 3).
Statistical analysis
Data are presented as mean ± SD, median (IQR) or number (frequency), wherever appropriate. Continuous variables were compared with the Student’s t-test, categorical variables with the χ2 test and ordinal variables with the Mann–Whitney U test. Univariable analysis was performed to evaluate differential ER success (absent, partial, complete) among patients with partial reperfusion (TICI 2a and 2b). Multivariate logistic regression analysis was performed to evaluate key factors known to be associated with clinical outcome, including age, baseline NIHSS, baseline ASPECTS, symptomatic intracranial hemorrhage (sICH) after EVT, different ER grades (absent, partial, complete), and the extent of partial reperfusion (TICI 2b vs 2a) on 90-day disability (mRS) among patients with anterior circulation occlusion. Ordinal shift analysis across the entire range of functional disability (0–6) was used to estimate the effect on clinical outcome at 90 days.
Results
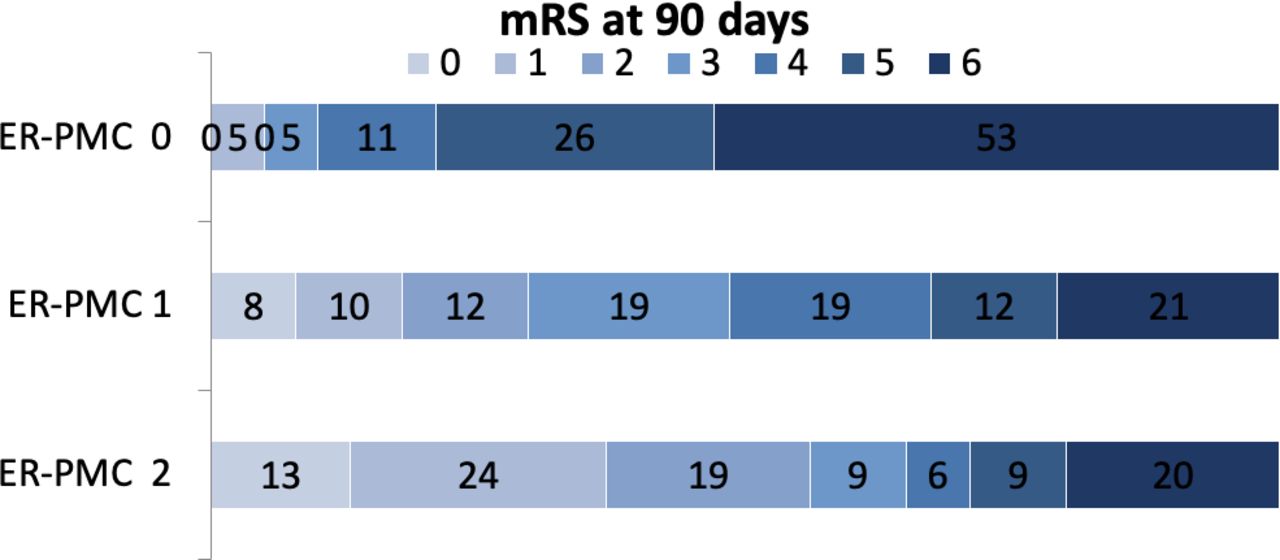
Table 2 shows the characteristics of the study population. Among the 125 patients who met the study criteria, median age was 73 years, median NIHSS was 16, median ASPECTS was 7, 48% (60/125) were female, and 36.8% achieved functional independence (mRS 0–2) at 90 days. The most common target occlusion location was M1, followed by ICA, M2, and tandem ICA/M1. All patients had hypoperfusion within the PMC prior to revascularization. All pre-intervention ER-PMC was scored as 0, including the M2 target occlusions. ER-PMC distribution was: absent (0) in 19/125 (15.2%); partial (1) in 52/125 (41.6%), and complete (2) in 54/125 (43.2%). Patients who had TICI 2b scores had substantially higher proportion of ER1 (78.8%) and ER2 (94.4%) in comparison to those who achieved TICI 2a (21.2%, and 5.6%, respectively) (P<0.001). However, the distribution of ER-PMC 0 reperfusion, was almost equal in patients with TICI 2a (47.4% (9/19) versus TICI 2b (52.6% (10/19) recanalization (P=0.74) (table 3). Furthermore, none of the patients with TICI 2b/ER-PMC 0 achieved functional independence (mRS 0–2) in 90 days as opposed to 15.2% of those with TICI 2a/ER-PMC 1 or 2 (P=0.01). In multivariate analysis, in addition to age and sICH, ER-PMC had a profound impact on 90-day disability (OR 6.10, P=0.001 for ER 1 vs 0 and OR 9.87, P<0.001 for ER 2 vs 0). In contrast, extent of total partial reperfusion (TICI 2b vs 2a) did not correlate to 90-day disability in this multivariate analysis (table 3). As demonstrated in figure 4, there is significant shift towards better functional outcome in patients with ER-PMC 1 and 2.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of 90-day modified Rankin Scale (mRS) according to eloquent reperfusion-primary motor cortex (ER-PMC) grading (0, 1, 2) following mechanical thrombectomy in patients with anterior circulation large vessel occlusion
Characteristics of the study population
Distribution of eloquent reperfusion-primary motor cortex (ER-PMC) grade per thrombolysis in cerebral infarction (TICI) score and results of the multivariate analysis
Discussion
The findings of our study provide a refined and more comprehensive prediction of procedural success, highlighting the importance of neurovascular anatomical localization in EVT for AIS. In this analysis, we observed a robust association between eloquence-based reperfusion and functional outcomes following EVT of AIS. Patients with complete or partial reperfusion within the PMC were much more likely to achieve functional independence as compared with those with absent antegrade PMC flow, irrespective of the level of partial TICI reperfusion (TICI 2a or 2b). These findings confirmed our hypothesis that detailed assessment of angiographic reperfusion within the most eloquent vascular territories supplying the PMC more reliably predicts disability as compared with the traditional volume-based reperfusion.
The ultimate goal of any endovascular procedure aimed at revascularizing an acutely occluded vessel is to improve clinical outcome through rapid flow restoration within the ischemic territory. Successful revascularization, measured by a widely applicable and standardized grading scale, is a well-established biomarker of procedural success in both coronary and cerebral circulation.9 12 Unlike the TIMI revascularization scale, which has not been modified since its inception, the cerebral revascularization grading methodology continues to evolve. The initially proposed term “recanalization”, defined as re-establishing patency of the occluded vessel, has been replaced with the distinctly different ischemic tissue “reperfusion” as a more reliable predictor of clinical outcome.29 30 The description of distal flow perfusion before and after revascularization therapy, first introduced in the TIMI scoring system, has served as a benchmark for development of the currently accepted TICI grading system.11 Although seemingly similar to TICI and historically used in multiple AIS trials, the TIMI scoring is inferior to TICI for prediction of clinical outcome after cerebral revascularization.31 The most substantial differentiating criteria separating both scales is the extent of partial reperfusion, wherein TICI 2a to TICI 2b (ie, substantial reperfusion in greater than half of the target downstream territory) or greater is defined as the optimal threshold for predicting 90-day independence and remains the universally accepted angiographic endpoint for procedural “success”. However, this dichotomized analysis fails to explain why a substantial proportion of patients with “unsuccessful” partial reperfusion (TICI 2a) achieve functional independence, exceeding 40% in some studies.16 Our findings highlight the importance of analyzing cerebral reperfusion based on territorial supply and question the concept of purely volumetric assessment of reperfusion (TICI) as the only marker of clinical outcome in AIS. In other words, both quantitative and qualitative assessments are needed.
As outlined by Rha and Saver, for a biomarker to serve as an auxiliary or surrogate procedural outcome measure, it must be tightly correlated with and causally related to functional clinical outcome.29 While the primary clinical outcome measure for coronary revascularization in acute myocardial infarct is mortality,32 the universally accepted outcome measure of endovascular therapeutic success in AIS is functional disability at 90 days, measured by the mRS. Though heavily criticized for its subjectivity and explicit focus on walking ability, yet underestimating crucial cognitive, behavioral, and psychosocial aspects of post-stroke stroke disability, this primarily motor-based scale remains the standard measure of therapeutic success of acute stoke therapies.33–35 In the context of the specific topographic localization of motor pathways within the cerebral cortex and their corresponding arterial supply, revascularization of these eloquent regions highly correlates with mRS as evidenced by our data. Furthermore, when applied in a multivariate model with eloquent motor cortex reperfusion, the TICI scoring did not show strong correlation with disability. Although the proportion of patients with partial (1) or complete (2) eloquent motor cortex reperfusion was substantially higher in patients who achieved TICI 2b, absence of ER-PMC flow was almost equal in TICI 2a versus TICI 2b. These findings clearly demonstrate that the simplistic volume-based assessment of cerebral reperfusion does not adequately predict disability. As such, ER-based territorial angiographic assessment in patients achieving partial reperfusion may provide a better prediction of clinical outcome after EVT.
Our findings also have practical implications. Eloquence-based lesion evaluation is a well-established method for optimal patient selection and prediction of outcome in the neurosurgical practice. Emanating from the early 1950s, the term “eloquent cerebral cortex” was initially introduced by Charles Drake in the context of neurosurgical approach to cerebrovascular disease and subsequently solidified by Spetzler and Martin.25 36 37 To date, the Spetzler–Martin grading scale remains the most widely used marker for periprocedural risk stratification in endovascular and surgical management of cerebral arteriovenous malformations (AVMs). In their original article, the authors defined the word “eloquent” to reference the area of the brain “that speak to readily identifiable neurologic function, that if injured, result in disabling deficit”. The areas considered eloquent in this seminal paper were the sensorimotor, language, and visual cortex; the hypothalamus and thalamus; the internal capsule; the brain stem; the cerebellar peduncles; and the deep cerebellar nuclei. Identification of these functional areas in relationship to the AVM is the surrogate marker for risk stratification and procedural planning. Similarly, detailed angiographic flow assessment within the eloquent vascular territories may guide decision making during EVT for AIS. In this analysis of anterior circulation occlusions, we used the PMC as an easily identifiable angiographic marker of eloquent reperfusion both for the purposes of prediction of disability and potential therapeutic implications. The results of our study suggest that more aggressive, PMC-targeted revascularization among patients with non-eloquent partial reperfusion may further improve post-stroke disability after EVT, while further revascularization attempts in patients achieving eloquent partial reperfusion may not be necessary. For instance, a TICI 2b/ER-PMC 0 angiographic result with persistent occlusion of the MCA precentral territory may require additional recanalization attempts, whereas the need for excessive attempts following a TICI 2a/ER-PMC 2 result with patent eloquent branches may be balanced by the risk of procedural complications. As evidenced by two large-scale registries, complete recanalization with a single thrombectomy device pass occurs in less than one-third of the treated patients, requiring additional passes in patients with partial or incomplete reperfusion.38 39 Although the number of stentriever passes has shown no correlation with hemorrhagic transformation in the proximal vasculature,40 successive revascularization attempts in the distal vessels may be associated with added risk. In addition, the optimal method of revascularization (pharmacologic or mechanical) of distal occlusions supplying eloquent territories remains unclear. Initial data from the SWIFT trial involving older-generation thrombectomy devices demonstrated significant risk of intracranial hemorrhage associated with intraarterial (IA) tissue plasminogen activator (tPA) administration as a rescue therapy after mechanical thrombectomy.41 However, a recent single-center retrospective study showed no evidence of increased hemorrhagic risk with IA tPA for treatment of residual distal occlusions after thrombectomy with newer-generation devices.42 Mechanical revascularization of distal arterial occlusions is also controversial. Mokin et al reported that vessel perforation in stent retriever thrombectomy most commonly occurred in distal occlusion sites.43 Conversely, Grossberg et al demonstrated the safety and efficacy of distal thrombectomy as primary treatment modality for AIS.44 Furthermore, newer devices designed specifically for smaller intracranial vessel distal arterial occlusion have demonstrated very promising results.45–47 As the methodology of distal thrombectomy evolves, eloquence-based angiographic assessment is crucial for optimal risk/benefit stratification in setting EVT for AIS.
Our study has several important limitations. First, this was a retrospective analysis of prospectively collected data. Second, the angiographic definition of ER was based on flow only within the cortical branches supplying the primary motor cortex, without taking into account the perforator supply of the subcortical motor tracts. Third, ER was defined as presence of antegrade flow within the PMC branches, without taking into account collateral supply from adjacent non-eloquent branches. Finally, the term “eloquence” in this article applies only to the PMC without including other important cortical areas within the anterior circulation responsible for key cognitive functions known to impact post-stroke disability, such as vision, memory, attention, and language.
Conclusions
Eloquence-based neuroanatomic reperfusion assessment is a much stronger predictor of functional outcome as compared with the traditional volume-based (TICI) assessment after EVT for treatment of AIS. Eloquent PMC is a key revascularization target among patients with incomplete total reperfusion.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors RR: (first author) interpreted the data, drafted a significant portion of the original manuscript, reviewed all suggestions provided by all co-authors, approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved, composed the final version of the manuscript and assumed responsibility for final review and submission as a corresponding author. DL: (senior author) provided a final overview of the paper and revised a substantial portion of the manuscript. HS: provided a substantial contribution to the interpretation of the provided data. JLS, JDH: provided a substantial contribution to the interpretation of the provided data and contributed with substantial revisions of the original draft. SB: contributed with statistical analyses and data interpretation. FV, GD, RJ, ST, VS, MN, GPC, LR, DK, MBH, LA, SS, RGN, NR: contributed with revisions to the original draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.