Article Text

Abstract
Background Flow diversion of acutely ruptured intracranial aneurysms (IAs) is controversial due to high treatment-related complication rates and a lack of supporting evidence. We present clinical and radiological results of the largest series to date.
Methods This is a nationwide retrospective study of acutely ruptured IAs treated with flow diverters (FDs). The primary outcome was the modified Rankin Scale (mRS) score at the last available follow-up time. Secondary outcomes were treatment-related complications and the aneurysm occlusion rate.
Results 110 patients (64 females; mean age 55.7 years; range 12–82 years) with acutely ruptured IAs were treated with FDs between 2012 and 2020 in five centers. 70 acutely ruptured IAs (64%) were located in anterior circulation, and 47 acutely ruptured IAs (43%) were blister-like. A favorable functional outcome (mRS 0–2) was seen in 73% of patients (74/102). Treatment-related complications were seen in 45% of patients (n=49). Rebleeding was observed in 3 patients (3%). The data from radiological follow-ups were available for 80% of patients (n=88), and complete occlusion was seen in 90% of aneurysms (79/88). The data from clinical follow-ups were available for 93% of patients (n=102). The overall mortality rate was 18% (18/102).
Conclusions FD treatment yields high occlusion for acutely ruptured IAs but is associated with a high risk of complications. Considering the high mortality rate of aneurysmal subarachnoid hemorrhage, the prevention of rebleeding is crucial. Thus, FD treatment may be justified as a last resort option.
- Aneurysm
- Flow Diverter
- Hemorrhage
- Subarachnoid
- Stroke
Data availability statement
Data are not available for public, however upon a reasonable request it may be provided.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Surgical clipping and endovascular coiling are well-established methods of treating acutely ruptured intracranial aneurysms (IAs). The International Subarachnoid Aneurysm Trial and the Analysis of Treatment by Endovascular Approach of Non-ruptured Aneurysms study have demonstrated the efficacy and safety of endovascular coiling in the treatment of intracranial aneurysms.1 2 Some specific types of aneurysms, such as blister-like and dissecting aneurysms, are challenging to treat with conventional endovascular and surgical methods. When ruptured, these types of aneurysms also carry a higher risk of rebleeding than saccular-shaped intracranial aneurysms.3 4 Conventional treatment methods for blister-like, dissecting, and fusiform aneurysms are the sacrificing of the parent artery, aneurysm wrapping, and bypass. However, such techniques are often associated with a high risk of complications.5
Flow diverters (FDs) have emerged as a versatile endovascular treatment for intracranial aneurysms, particularly for unruptured aneurysms of the internal carotid artery (ICA). FDs disturb the intrasaccular blood flow of the aneurysm, leading to remodeling and complete shrinkage. Intracranial aneurysms treated with FDs have shown a complete occlusion rate of as high as 90%.6–8 However, FD treatment carries a higher risk of thromboembolic and hemorrhagic complications than coiling.8 Use of FDs has increased in the treatment of acutely ruptured IAs, even though the treatment carries a high risk of complications.9 10 In the case of acutely ruptured IAs, remodeling of the aneurysm after FD treatment requires weeks, even months, before complete occlusion can be achieved. Therefore, during remodeling there is a non-negligible risk of rebleeding.8 Another challenge in FD treatment is the necessity of dual antiplatelet therapy (DAPT) in order to prevent thromboembolic complications, which increases the risk of hemorrhagic complications. Especially in the treatment of acutely ruptured IAs with FDs, both hemorrhagic and ischemic complications are more frequent than with conventional coiling, mostly because of the risk attributed to DAPT.9 10 DAPT may cause difficulties, especially in the treatment of patients with acutely ruptured IAs, which often require surgery such as placement of the external ventricular drain (EVD). Some hemorrhagic complications after treatment of acutely ruptured intracranial aneurysms with FDs could be avoidable by placing the EVD before FD placement.10 11 Overall, data on the use of FDs in the treatment of acutely ruptured IAs are still limited.
The aim of our study is to evaluate clinical and radiological outcomes as well as treatment-related complications of patients treated with FDs for acutely ruptured IAs.
Methods
Study design
This is a multicenter retrospective study including all consecutive patients treated with FDs for acutely ruptured IAs between January 2012 and December 2019. All university hospitals providing neuroendovascular services participated in this study.
Decisions on FD treatment were made at the discretion of the participating centers. At all of the centers, treatment decisions were made by multidisciplinary neurovascular teams. FD treatment for an acutely ruptured IA was only considered as a last option when other open surgical and endovascular methods were not suitable.
Neurointerventions
All interventions were performed under general anesthesia. Pre-procedural, procedural, and post-procedural antiaggregant and anticoagulant medicines were reported. Use of antiplatelet drugs varied widely. The most commonly used peri-procedural antiaggregant medicine was abciximab, which was administered as a bolus and infusion after deployment of the FD. Most of the patients received heparin during the neurointerventions in order to double the activated clotting time from the baseline. During the procedure, aspirin 250 mg or 500 mg was administered intravenously to nearly all patients. Due to possible hyporesponders and non-responders to clopidogrel in the population, prasugrel was administered as a second antiaggregant in a 60 mg loading dose followed by a 5 mg or 10 mg maintenance dose. All centers tested platelet function with Multiplate® (Roche Diagnostic, Mannheim, Germany) or VerifyNow® (Accumetrics, San Diego, CA) test. Multiplate-platelet adenosine diphosphate (MPADP) <30U and 60–200 P2Y12 reaction-units (PRU) were considered a sufficient response. Prasugrel and clopidogrel were continued for at least 3 to 6 months unless there was a life-threatening hemorrhage. A dose of 100 mg of aspirin per day was continued for at least 6 to 12 months. At one of the centers, post-procedural low molecular weight heparin (LMWH) was used as a second antithrombotic medicine in addition to aspirin 100 mg. At most of the centers, the duration of the DAPT was decided on the basis of the first imaging follow-up.
Complications
All peri- and post-procedural complications thought to be possibly intervention related were reported. Complications were classified as intracranial hemorrhagic, intracranial ischemic, extracranial hemorrhagic, and other (eg, external ventricular drain occlusion). Any new intracranial hemorrhage or expansion of an existing intracranial hemorrhage (subarachnoid, parenchymal, or intraventricular) after treatment was considered a treatment-related complication; additionally, any ischemic lesion within the vascular territory of the FD-treated aneurysm, excluding those caused by delayed cerebral ischemia (DCI), detected with post-procedural CT or MRI was considered a treatment-related complication. Any major bleeding (eg, epistaxis, groin hemorrhage, gastrointestinal, or retroperitoneal hemorrhage) was classified as an extracranial complication.
Clinical and radiological follow-up
All patients were scheduled for a postoperative clinical and radiological follow-up after the intervention. The radiological follow-up, in terms of imaging modality and frequency, after FD treatment varied somewhat in the participating centers. The first radiological follow-up after FD treatment was at 3 or 6 months with digital subtraction angiography (DSA) or magnetic resonance angiography (MRA). Data regarding the functional clinical outcome were assessed based on clinical follow-up visits and reported according to a modified Rankin Scale (mRS) score. The last recorded clinical follow-up was reported. An mRS ≤2 was considered a favorable functional outcome and an mRS ≥3 an unfavorable functional outcome. Aneurysm occlusions were evaluated according to the O’Kelly Marotta (OKM) classification, as follows: complete occlusion, near complete occlusion (>50%), partial occlusion (<50%), and total filling of the aneurysm.
Statistical analysis
Descriptive statistics were used. Categorical variables are presented as numbers and percentages. Continuous variables are presented as mean and range.
Ethical aspects
Each participating center was granted a permit from the local institutional review board for medical studies. Local institutional review boards waived the need for formal consent for this retrospective registry study.
Results
Patient, aneurysm, subarachnoid hemorrhage and FD characteristics
One hundred and ten patients (58% female) with 110 acutely ruptured intracranial aneurysms were treated with FDs; 27% of the aneurysms were saccular (n=30), 14% were fusiform (n=15), 43% were blister-like (n=47), and 16% were dissecting (n=18). Sixty-four percent of the aneurysms (n=70) were located in the anterior circulation. The mean maximal diameter of the aneurysms was 4.8 mm (range 2–25). Three percent of the aneurysms (n=3) had been initially treated with coiling due to a previous subarachnoid hemorrhage (SAH). The mean age of patients was 55.7 years (range 12–82 years). The mean time from ictus to the treatment was 3.8 days (range 1–41 days). Patient, SAH, and aneurysm characteristics are summarized in table 1.
Patient and aneurysm/subarachnoid hemorrhage characteristics
Aneurysms were treated with the following types of FDs: 14 Pipeline embolization devices (PED; Medtronic, Minneapolis, MN), 62 PEDs with shield technology (Medtronic, Minneapolis, MN), seven Surpass Stream Lines (Stryker Neurovascular, Fremont, CA), 20 FREDs (MicroVention, Tustin, CA), 19 FRED JRs (MicroVention, Tustin, CA), two Derivos (Acandis, Pforzheim, Germany), two Surpass Evolves (Stryker Neurovascular, Kalamazoo, MI), and two SILKs (Balt, Montmorency, France). Sixteen percent of aneurysms (n=18) were treated with multiple FDs, and in 5% of aneurysms (n=5) coils were used in order to secure the occlusion. Types of FDs and treatment characteristics are summarized in table 2.
Type of flow diverters and treatment characteristics
Clinical and radiological outcome
Follow-up data were available for 93% of patients (n=102/110). The mean duration of clinical follow-up was 8 months (range 1–60 months). A favorable functional outcome (mRS 0–2) was seen in 73% of patients (n=74/102), whereas an unfavorable functional outcome (mRS 3–6) was seen in 27% of patients (28/102). The overall mortality rate was 18% (n=18/102), and the treatment-related mortality rate was 5% (n=5).
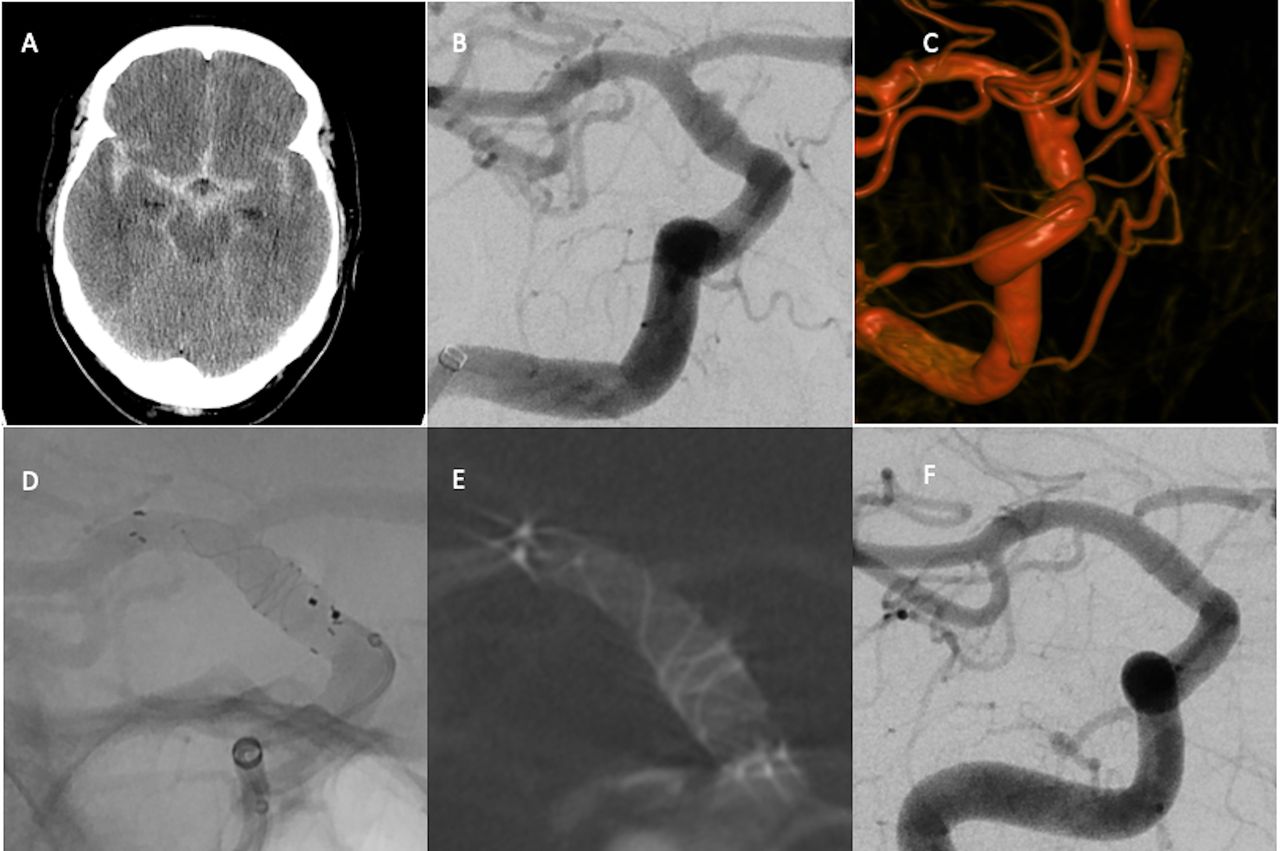
The mean duration of radiological follow-up was 11 months (range 1–60 months). Radiological follow-up data were available for 80% of patients (n=88/110). Of these, 63% of patients (n=55/88) underwent DSA, and 37% of patients (n=33/88) underwent either MRA or CT angiography follow-up imaging. In 90% of patients (n=79/88), complete occlusion of the aneurysm was achieved (O’Kelly Marotta Aneurysm occlusion class D). In 3% of patients (n=3/88) entry remnant was noted, and in 6% of patients (n=5/88) subtotal filling of the aneurysm was noted. In 1% of patients (n=1/88) complete filling of the aneurysm was seen. Clinical and radiological outcomes are summarized in table 3 and an illustrative case is presented in figure 1.
Clinical and radiological outcomes

{kind=link}
NECT image showing diffuse SAH (A). Three-dimensional rotational image and DSA showing a 1×2 mm ruptured blister-like aneurysm in right ICA (B, C). DSA captured during the deployment of FRED 4.0/18/12 mm (D). Dyna-CT showing good opposition of FD (E). DSA image showing complete occlusion of the aneurysm 4 months after the treatment (F). DSA, digital subtraction angiography; FD, flow diverter; FRED, flow re-direction endoluminal device; ICA, internal carotid artery; NECT, non-enhanced CT, SAH, subarachnoid hemorrhage
External ventricular drainage and shunt
In 46% of patients (n=51), an EVD was placed before the FD treatment. Additionally, 8% of patients (n=9) needed an EVD after the FD treatment. External ventricular drain occlusion was noted in 17 patients, and, as a consequence, the EVD was needed to be changed. A total of 28% of patients (n=31) needed a shunt for post-SAH hydrocephalus.
Complications
No intraoperative ruptures occurred. The rebleeding rate was 3% (n=3). Rebleeding occurred on the seventh, 12th and 65th day after treatment with a FD. No coils were used in the re-bled aneurysms. Two of the three re-bled aneurysms were dissecting and one was blister-like. Of these patients, one (1%) died due to rebleeding and two others had favorable functional outcomes at last follow-up.
A total of 45% of patients (n=49) had treatment-related complications. A postoperative intracranial hemorrhage was seen in 40% of patients (n=44). Of these, a new intracerebral hemorrhage (ICH) or expansion of an existing ICH was seen in 17% of patients (n=19). ICHs are summarized according to etiologies in table 4. Of patients with a post-procedural ICH or an expansion of a pre-procedural ICH, 47% (n=9/19) had an unfavorable functional outcome. Other hemorrhagic complications occurred: a groin hemorrhage was seen in 2% of patients (n=2), serious epistaxis in 1% of patients (n=1), and upper gastrointestinal bleeding in 1% of patients (n=1).
Postoperative intracerebral hemorrhages and etiologies
Ischemic complications (reported as not caused by DCI) were detected with CT and/or MRI in 29% of patients (n=32) after the FD treatment, and 34% of patients (n=11/32) with postoperative ischemic changes detected with CT and/or MRI had an unfavorable outcome (mRS 3–6).
In-stent thrombosis was seen in 8% of patients (n=9); as a consequence of this adverse effect, four patients died and five patients recovered with favorable functional outcome. Treatment-related mortality was 5% (n=6) and overall mortality was 18% (n=18/102). Types and frequencies of complications are summarized in table 5.
Types and frequencies of complication
Discussion
In this nationwide multicenter retrospective study, we included 110 Finnish patients with acutely ruptured intracranial aneurysms treated with FDs. In total, 73% of the patients had a good clinical outcome (mRS 0–2) and total or near total aneurysm occlusion was achieved in 92% of the aneurysms. However, hemorrhagic and/or ischemic complications were seen in 45% of patients.
Even though the overall rate of functional outcomes in the study by ten Brinck et al was 45% (n=20), aneurysm occlusion rates in the same study (93% vs 92% in our study) were similar to our study.10
In our study, almost half of the ruptured aneurysms were either the blister-like or dissecting type. In the case of blister-like, dissecting, and perforator aneurysms in posterior circulation, reconstructive treatment with FDs has been shown to be effective with an occlusion rate as high as 76%.3 12 In our study, the complete occlusion rate of blister-like aneurysms was 92% (43/47). In a study by Rouchaud et al, patients with an SAH from a blister-like aneurysm treated with reconstructive treatment had a similar good clinical outcome rate (76% vs 73% in our study).3
In this study, the overall procedure-related complication rate was 45%. In their multicenter observational study of 44 patients, ten Brinck et al reported a similar overall complication rate (45%).10 In our study, the ischemic complication rate was 29%, which is notably higher than in previous reports. In a meta-analysis of 20 studies by Cognazzo et al, the rate of ischemic complications was reported as 8%.9 The high ischemic complication rate was seen in our study is probably due to the fact that the participant centers reported all ischemic changes detected postoperatively, regardless of whether they were symptomatic or asymptomatic. Of those with an ischemic complication, approximately only one third had an unfavorable functional outcome. Yet, this does not mean that these ischemic complications are irrelevant. Overall, there is a need for studies looking at the quality of life and neuropsychological outcome of endovascularly treated SAH patients with clinically silent ischemic lesions, as there may be consequences of silent ischemic lesions that may lead to chronic diseases such depression and epilepsy.13 14
In previous studies, the rates of rebleeding were 5% and 11%, respectively.9 10 In this study, rebleeding occurred in only 3% of patients. Madaelil et al found that acutely ruptured aneurysms >2 cm are associated with a higher risk of rebleeding after FD treatment.15 However, none of the re-bled aneurysms in this study were larger than 2 cm. In fact, the average diameter of the aneurysms that rebled was 5.3 mm. One effective strategy in FD treatment for acutely ruptured IAs can be ‘plug and pipe’, which can be described as subtotal coiling in the acute phase and FD treatment in the recovery phase. Howard et al showed in their series that ‘plug and pipe’ could be an effective and safe strategy.16
Apart from the size of an aneurysm, certain blood-thinning medications may increase the risk of rebleeding. Manning et al reported in their study that rebleeding from the target aneurysm occurred in patients who had received heparin postoperatively after FD treatment for acutely ruptured IAs.17 In our series, rebleeding from the target aneurysm occurred in three patients who received LMWH after FD treatment. All were treated with aspirin and LMWH post-procedurally. Our results suggest LMWH is associated with high risk of rebleeding after FD treatment for ruptured IAs.
The 17% rate of post-treatment ICH in our series is higher than the rates reported in the meta-analysis.9 This difference could be explained by the fact that the participating centers in our study reported any new ICH or the enlargement of an existing ICH postoperatively as a postoperative complication, regardless of whether the ICH was symptomatic. In addition, an ICH related to an EVD placement after the intervention was also considered a treatment-related complication in our study. Forty-seven percent of patients with a new ICH or expansion of an existing ICH had an unfavorable functional outcome, which highlights the need for further strategies for reducing postoperative hemorrhagic complications. Kung et al found that placing an EVD or ventriculoperitoneal shunt raises the risk of radiological ICH by 3.42 times for patients receiving DAPT compared with patients without DAPT.11 One readily available strategy could be to insert EVDs with a low threshold before interventions for patients who are going to be treated with an FD.
As we have shown in our study, the hemorrhagic and ischemic complication rates of FD treatment of acutely ruptured IAs are not negligible; however, conventional treatments of acutely ruptured blister-like, fusiform and dissecting aneurysms are challenging. Without treatment, the mortality rate of rebleeding is as high as 90%.18 Further research should focus on hemorrhagic and ischemic complications of FD treatment for acutely ruptured IAs. Development of antiplatelet therapy and low thrombogenic FDs could help to reduce complication rates. Although a few studies showed hydrophilic-coated FDs remain patent with a single antiplatelet treatment,19 20 the evidence of using such FDs in the treatment of acutely ruptured IAs is limited. There is still a need for large and prospective studies because of the weak amount of supporting evidence.
Study limitations
There are limitations of our nationwide study. First, its retrospective design has inherent limitations such as absence of data on follow-ups. However, a large homogenous population as well as the large size of the subgroup of aneurysms treated in our study alleviate its inherent limitations. Another limitation of our study is the non-structured use of postoperative DAPT and heterogenous FD choice which may have affected the rate of complications, but in daily practice peri- and/or postoperative management of DAPT and choice of FDs differ in every neurointerventional clinic and response to each antiplatelet medication differs in each patient.
Conclusion
Flow diversion treatment of acutely ruptured intracranial aneurysms yields a high rate of long-term occlusion with a relatively low rate of aneurysm rebleeding. Despite the high complication rates in our study, the rate of favorable clinical outcome was significantly higher than previously reported. The high mortality rate of SAH and the challenging morphology of treated aneurysms in our study could justify FD treatment for acutely ruptured intracranial aneurysms.
Data availability statement
Data are not available for public, however upon a reasonable request it may be provided.
Ethics statements
Patient consent for publication
Ethics approval
The study permission was approved by the local institutional review boards of Turku University Hospital (T011/014/18), Tampere University Hospital (R16619), Kuopio University Hospital (166/2016), Oulu University Hospital (215/2018) and Helsinki University Hospital (HUS/125/2018). Local institutional review board waived the need for formal consent for this retrospective registry study.
References
Footnotes
Twitter @neurosurgeryfi, @rahulbrraj
Presented at Some results of the study were presented at ESMINT congress on 8 September 2020 in a plenary session.
Contributors Author contributions: KA, AL, RRaj, TH, JMI: study design, data collection and data analysis. KA: drafting of the manuscript and final revision of the manuscript. MS, JN, JPP, PS, JS and KP: data collection. RR and RP: study design and supervision. KA, TH, AL, RR, RP and JMI: critical revision of the draft. All authors give final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KA has received personal research grants from Turku University Foundation and Maire Taponen Foundation. RRaj has received personal research grants from Finska Läkaresällskapet and Medicinska Understödsföreningen Liv & Hälsä. RR is consultant for Microvention, Stryker and Medtronic.
Provenance and peer review Not commissioned; externally peer reviewed.