Article Text

Abstract
In-stent stenosis (ISS) triggered by a metal-induced allergic reaction of Pipeline embolization device (PED) placement is extremely rare. The present report describes a patient who presented with delayed parent artery occlusion and refractory ISS after PED placement due to cobalt allergy. A patient in her 70s underwent PED placement for a right internal carotid artery (ICA) large aneurysm; 4 months later, the patient presented with left-sided hemiparesis, and MRI revealed right ICA occlusion even though antiplatelet therapy was optimal. She underwent mechanical thrombectomy, and successful recanalization was achieved. However, follow-up angiography 6 months after the thrombectomy revealed severe ISS, and the patch testing showed a positive reaction for cobalt. As a result of long-term administration of oral steroids and antihistamine, progression of ISS was suppressed. It was supposed that a delayed hypersensitivity reaction to cobalt might induce refractory ISS after PED placement.
- flow diverter
- inflammatory response
- thrombectomy
- angioplasty
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Delayed ischemic events secondary to in-stent stenosis (ISS) are serious complications of intracranial stent implantation and have not been completely understood and characterized. Apart from the lack of antiplatelet effect or stent malapposition, allergic reaction to the metal device might be associated with ISS.1 However, to our knowledge, ISS and thrombosis associated with metal allergy after intracranial stent implantation have not yet been reported. We describe a case of in-stent thrombosis and refractory ISS after a Pipeline embolization device (PED, Medtronic/Covidien, Irvine, California, USA) placement for an internal carotid artery (ICA) large aneurysm, possibly associated with cobalt allergy.
Case presentation
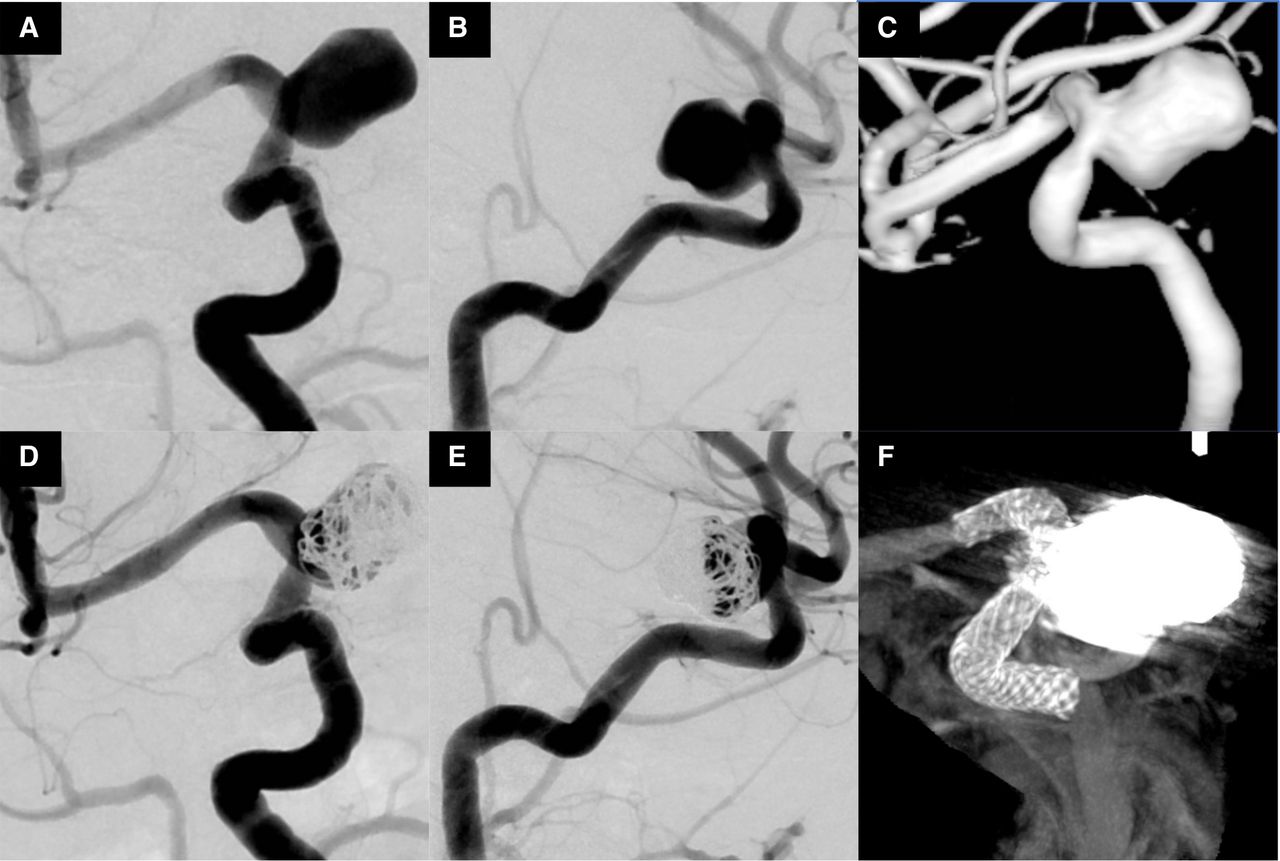
A patient in her 70s was incidentally found to have a large right ICA aneurysm on MRI. She had dyslipidemia and osteoporosis. Her past medical history confirmed that she had no drug allergy; her metal allergy was not seen prior to PED placement. Digital subtraction angiography showed a right paraclinoid large ICA aneurysm, 15 mm in diameter (figure 1A–C). She elected to undergo endovascular treatment with a PED.

(A,B) Right carotid angiogram and (C) three-dimensional reconstruction demonstrating unruptured large aneurysm at the C2 portion. (D, E) Immediate postoperative angiography and (F) cone-beam computed tomography (CT) showing Pipeline embolization device across the internal carotid artery and coil insertion.
Treatment
She received dual antiplatelet therapy with acetylsalicylic acid (100 mg/day) and clopidogrel (75 mg/day), 2 weeks before the procedure. Antiplatelet activity was checked using VerifyNow assay (Accumetrics, San Diego, California, USA) the day before the procedure, and antiplatelet effects were confirmed to be optimal. The procedure was performed under general anesthesia and systemic heparinization. After deployment of PED, coil embolization was additionally performed using bare platinum coil (figure 1D–F). She was discharged on day 7 without any neurological deficits, and dual antiplatelet therapy was continued.
Outcome and follow-up
Four months postoperatively, she presented with acute onset of left-sided hemiparesis. Diffusion-weighted imaging showed hyperintense lesions in the corona radiata and MR angiography revealed ICA occlusion (figure 2A–C). Cerebral angiography confirmed the in-stent thrombosis with right ICA occlusion (figure 2D). Mechanical thrombectomy was performed using the stent-retriever device, and the clot was retrieved. Although recanalization was achieved, ISS remained. Next, percutaneous transluminal angioplasty was performed, and complete recanalization was achieved (figure 2D). Antiplatelet effects were confirmed to be optimal. Blood tests were normal. Following cerebral angiography, 1 week after the procedure, complete recanalization and stent patency was maintained (figure 3A). She was referred to a rehabilitation center owing to slight left-sided hemiparesis 4 weeks postoperatively, with a modified Rankin scale score of 3. Six months after thrombectomy, the modified Rankin scale score was 0. However, follow-up cerebral angiography demonstrated severe ISS (figure 3B). To investigate the cause of the ISS, her medical history was rechecked, revealing a flare reaction in the area of contact with metal jewelry, and a patch test was performed. Metals of PED (nickel, cobalt, platinum, chromium, etc) and powder of PED were included in the patch test. A positive result was seen for the cobalt reagent, and slightly positive results for PED stent reagents (figure 4) With cobalt-induced ISS suspected, oral administration of steroids (prednisolone; initial dose: 40 mg/day for 2 days, tapering for 7 days, maintenance dose: 2.5 mg/day) and antihistamines (fexofenadine 120 mg/day) was initiated. Cerebral angiography was performed 7, 9, and 14 months after thrombectomy (figure 3C–E). Fourteen months later, progression of ISS was confirmed to be suppressed. Oral administration of steroids and antihistamines was completed, and close observation has been continued.
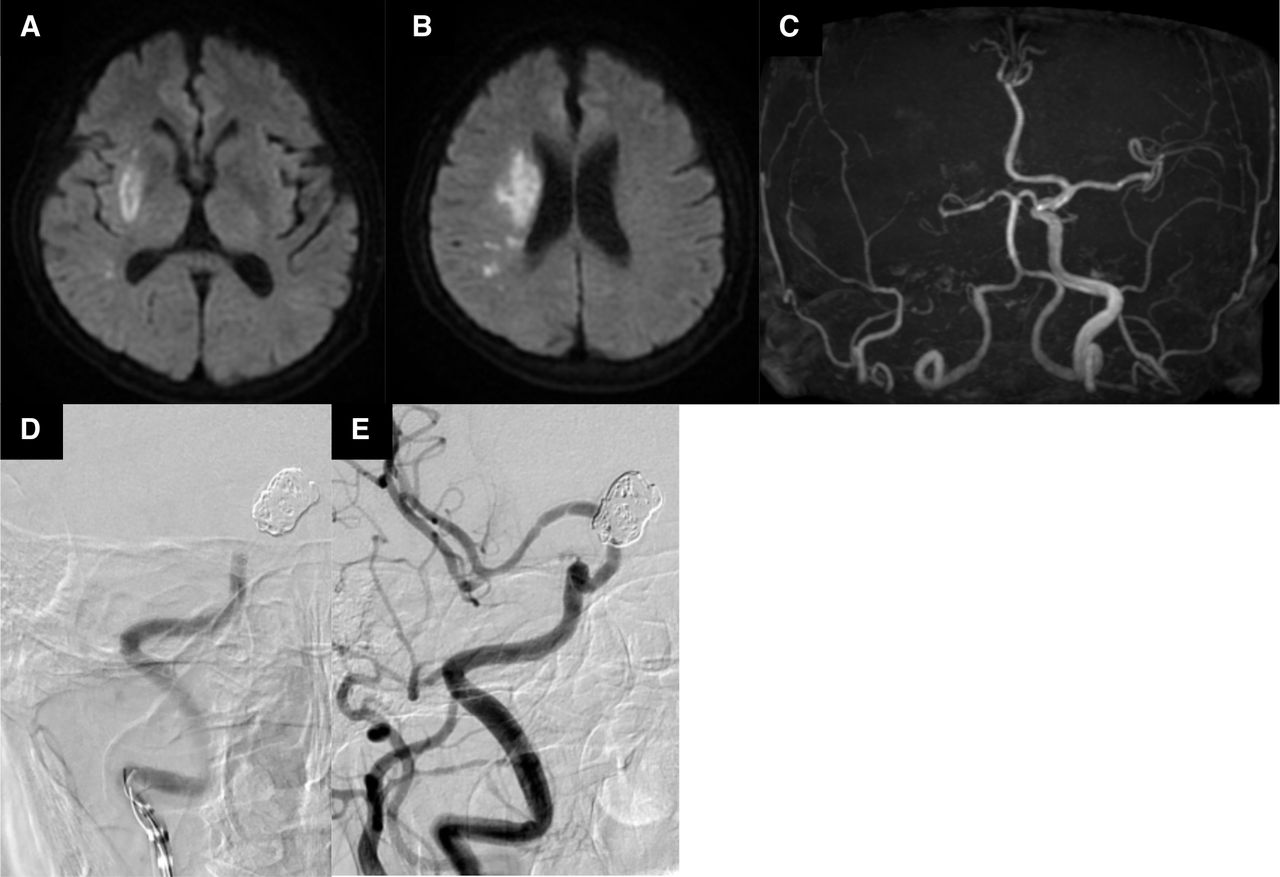
(A) Diffusion-weighted images showing hyperintense lesions at the right corona radiata. (C) Magnetic resonance (MR) angiography revealing the absence of the right carotid artery. (D) Right carotid angiography revealing the occlusion of proximal side of Pipeline embolization device. (E) The right internal carotid artery is completely recanalized.
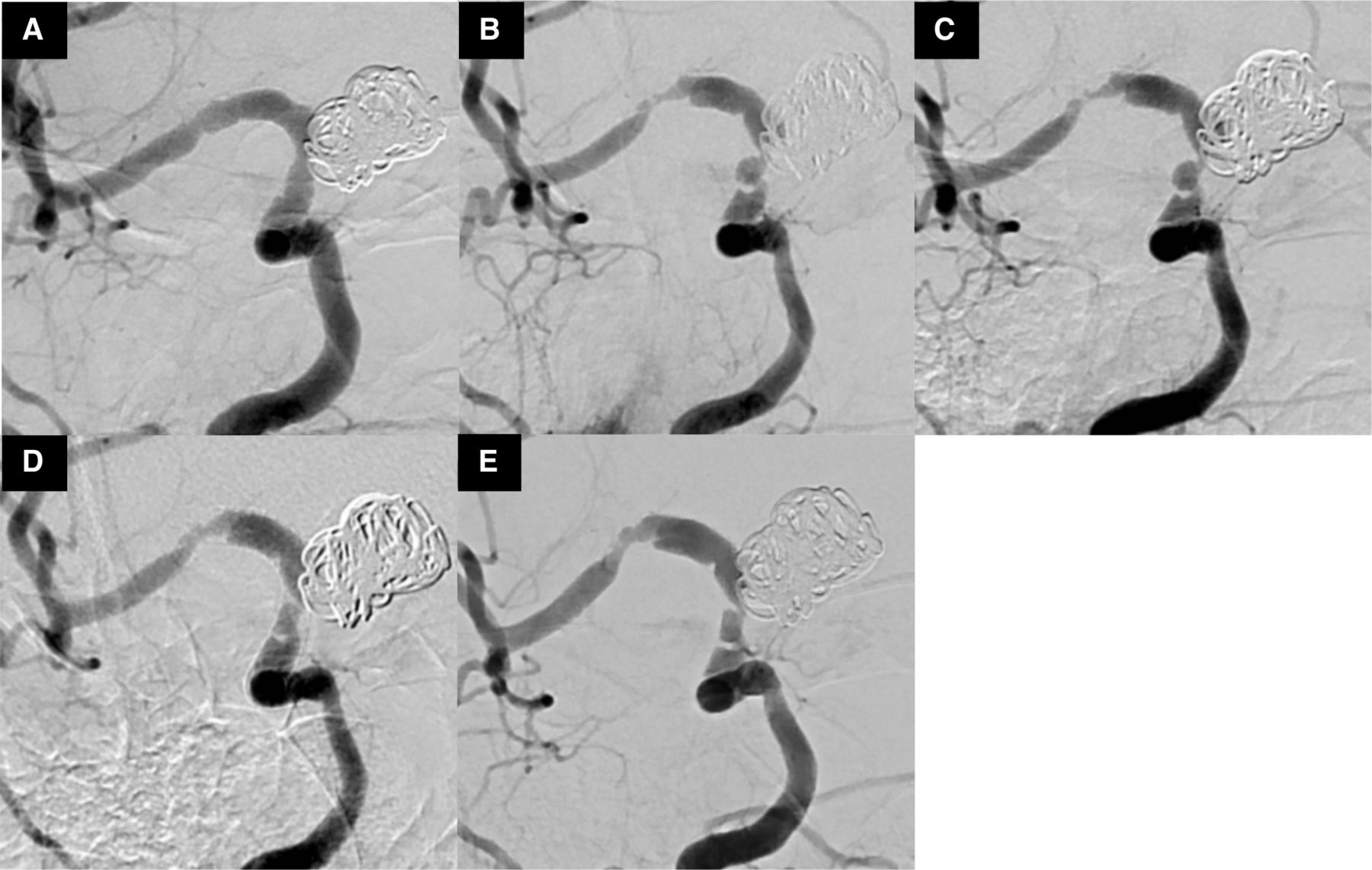
Right carotid angiography after thrombectomy. (A) At 1-week follow- up, (B) at 6-months' follow-up, (C) at 7- months' follow-up, (D) at 9-months' follow-up, and (E) at 14-months' follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical photograph showing positive patch test reaction for cobalt.
Discussion
Clinical symptoms of contact dermatitis are secondary to the inflammation caused by delayed-type hypersensitivity reaction (DTR) to the metal. With metal ions released into the circulation, intracranial metal device implantation might induce DTR, such as allergic dermatitis, encephalopathy, and reversible parenchymal changes.2–4 ISS is also reported as DTR to coronary stents, and inflammatory cell activation, and excessive proliferation occur within implanted metal stents.1
We encountered delayed parent artery occlusion after PED placement and ISS recurrence. Antiplatelet activity was optimal, and patch testing showed a positive reaction for cobalt in the PED. After administration of oral steroids and antihistamines, progression of ISS was suppressed, and no other findings suggested causative disease. Thus, we considered that delayed parent artery occlusion and ISS recurrence were associated with cobalt allergy. As there is no report of cobalt allergy with PED placement and no evidence for long-term outcomes for medical treatment of DTR to metal device implantation, close clinical and angiographic monitoring are warranted.
If unusual skin symptoms are observed in the area of contact with metal jewelry or precious metal, metal allergy is suspected, and patch testing is performed. Most reports that described the association between DTR and metal implants suggest that patch testing is positive for implanted metals and useful for diagnosis.1–3
For metal allergy, removal of potential causes is the most effective treatment. However, removal of a metal device placed in the intracranial blood vessel was impractical, thus medical treatment was considered as first option for DTR to metal implants. Previous studies have shown that administration of oral steroids is effective and relieves various symptoms.2 3 5 We selected the dose of corticosteroid according to the dose of contact dermatitis. As the regimen, 5 to 7 days of prednisone, 0.5–1 mg/kg daily is recommended. After this initial therapy, the dose may be reduced by 50% for the next 5 to 7 days.6 Although antihistamines are generally not effective for contact dermatitis,6 some reports showed that oral administration of antihistamines was effective for DTR to metal implants,2 5 and therefore we initiated oral antihistamines. Additionally, because past study has shown that cilostazol prevents in-stent stenosis,7 a switch to, or addition of, cilostazol might be a treatment option.
Common metal substances that cause DTR include nickel and cobalt. PED and other flow diverter stents, such as Silk (Balt Extrusion, Montmorency, France), the flow redirection endoluminal device (FRED; MicroVention, Tustin, California, USA), the p64 flow-modulation device (Phoenix, Arizona, USA), and the Surpass flow diverter (Surpass; Stryker Neurovascular, Fremont, California, USA), contain either nickel or cobalt. Therefore, if ISS occurs after PED or other flow-diverter stent placement, and the cause is unidentified, medical history related to allergy should be examined and patch testing performed. Before endovascular surgery, if the patient has a strong allergy to the metal in the stent, other treatment options should be considered.
Learning points
We describe a rare case of delayed parent artery occlusion and in-stent restenosis after Pipeline embolization device (PED) placement associated with cobalt allergy; administration of oral steroids and antihistamines suppressed the progression of in-stent stenosis.
Despite being rare, delayed-type hyper-reaction to metal device implantation may induce inflammatory cell activation and excessive proliferation and in-stent stenosis after PED placement.
If in-stent stenosis after PED placement occurs, and the reason for this is unclear, we should suspect metal allergy and recheck past medical history related to allergy and perform patch testing.
Supplemental material
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors I certify that neither this manuscript nor one with substantially similar content under my authorship has been published or is being considered for publication elsewhere. KS and SF planned this case report, and SF took the lead in writing the manuscript. SN, KM, SH, KF, and HY provided critical and important feed back.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.