Article Text

Abstract
Background Endovascular thrombectomy (EVT) for ischemic stroke (IS) beyond 6 hours has been proven effective in randomized controlled trials. We present data on implementation and outcomes for EVT beyond 6 hours in Sweden.
Methods We included all cases of anterior circulation IS caused by occlusion of the intracranial carotid artery, and the M1 or M2 segment of the middle cerebral artery, registered in two nationwide quality registers for stroke in 2015–2020. Three groups were defined from onset-to-groin-puncture (OTG) time: early window (<6 hours), late window (6–24 hours) known onset, late window last seen well (LSW). Favorable outcome (modified Rankin Scale (mRS) 0–2) and all-cause mortality at 90 days were the main outcomes, and symptomatic intracerebral hemorrhage (sICH) was the safety outcome.
Results Late window EVT increased from 0.3% of all IS in 2015 to 1.8% in 2020, and from 17.4% of all anterior circulation EVTs in 2015 to 32.9% in 2020. Of 2199 patients, 76.9% (n=1690) were early window EVTs and 23.1% late window EVTs (n=509; 141 known onset, 368 LSW). Median age was 73 years, and 46.2% were female, with no differences between groups. Favorable outcome did not differ between groups (early window 42.4%, late window known onset 38.9%, late window LSW 37.3% (p=0.737)) and remained similar when adjusted for baseline differences. sICH rates did not differ (early window 4.0%, late window known onset 2.1%, late window LSW 4.9% (p=0.413)).
Conclusion Late window EVTs have increased substantially over time, and currently account for one third of anterior circulation treatments. Early and late window patients had similar outcomes.
- Stroke
- Thrombectomy
- CT perfusion
- Thrombolysis
Data availability statement
Data are available upon reasonable request. Requests to access an anonymized dataset supporting the conclusions may be obtained with an appropriate ethics approval.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The penumbra concept was formulated in experimental stroke research as functionally impaired but salvageable ischemic brain tissue sustained mainly through pial collateral blood flow.1 2 Imaging of the penumbral tissue by CT or MRI perfusion3 4 has shown that the transition from ischemia to infarction varies considerably between patients,5 6 suggesting that a portion of patients may benefit from revascularization beyond the established time window of 6 hours for endovascular thrombectomy (EVT). This principle was proven in the DAWN (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) and DEFUSE 3 (Endovascular Therapy Following Imaging Evaluation for Ischaemic Stroke 3) trials, demonstrating a substantial benefit of EVT within an extended treatment window up to 24 hours of onset.7 8 These trials have led to a rapid introduction of new guideline recommendations for patient selection by CT or MRI perfusion in the late time window.9 10 In Sweden, EVT in the 6–24 hour interval using CT perfusion (CTP)-based patient selection was introduced in the national stroke guidelines in 2019 with recommendations reaching the highest priority.11 The guideline does not detail a minimum volume of salvageable tissue or mismatch ratio, leaving such decisions up to the treating teams. It is not well known how the new guidelines have been implemented on a nationwide level and how the results from late window EVT in routine clinical care compare to the randomized controlled trials (RCTs).
The aims of this study were to describe the implementation of late window EVT in routine healthcare on a national level and to describe patient, process, and treatment characteristics, as well as prognosis in late window EVT patients, and compare them to early window EVT patients treated during the same period.
Methods
Study design
This was a nationwide prospective, observational study on the implementation and outcome of EVT treatment for anterior circulation large vessel occlusion (LVO) stroke beyond 6 hours of onset in Sweden in 2015–2020.
Setting and data sources
The study was based on two nationwide, hospital-based quality registers for stroke care in Swedish routine healthcare. Riksstroke has served as Sweden’s quality register for stroke care since 1994. It collects extensive data regarding patient demographics, risk factors, functional status, stroke characteristics and treatments. Data are entered into the register by licenced healthcare personnel. The EVAS (the Swedish EndoVAscular treatment of Stroke) register collects detailed data on pre-hospital triage, process times, imaging, and endovascular treatment details. Data are entered into EVAS by nurses, neurointerventionalists and neurologists. No core-lab assessment is used; data are reported by the treating center. Both registers cover >90% of Swedish hospital-admitted stroke patients and EVT patients, respectively. We created a merged database of the two registers. Dates of death were obtained from the Swedish Causes of Death Register which has >99% coverage. Sweden, with its relatively small population of 10.3 million and half of the population concentrated around three urban areas, has seven comprehensive stroke centers (CSCs) offering EVT 24/7, and 65 primary stroke centers (PSCs) offering intravenous thrombolysis (IVT). Mode of triage (direct triage vs secondary transport from PSCs) is highly dependent on local and geographical conditions and varies throughout the country. All PSCs and CSCs (n=72) contribute to Riksstroke and all seven CSCs contribute to EVAS.
Patient selection
We included all patients with anterior circulation large vessel occlusion acute IS, defined as occlusion of the intracranial portion of the internal carotid artery or the M1 or M2 segment of the middle cerebral artery on digital subtraction angiography (DSA), who were registered in both Riksstroke and EVAS from January 1, 2015 to December 31, 2020 and had groin puncture with the intention of EVT, were pre-stroke independent defined as modified Rankin Scale (mRS) score of 0–2, and had registered onset-to-groin (OTG) times.
Main variables and outcomes
Three groups were defined by the time from stroke OTG puncture: (1) early time window group was defined as OTG time between 0–6 hours; (2) late window known onset group was defined as OTG time in the 6–24 hour interval from a known time of onset; and (3) late window last seen well (LSW) group was defined as OTG time in the 6–24 hour interval from LSW.
Data from Riksstroke included demographics and baseline characteristics: age, sex, pre-stroke functional status, vascular risk factors, and treatments. Onset-to-needle (OTN) and door-to-needle (DTN) times were calculated from source data. Data from EVAS included National Institutes of Health Stroke Scale (NIHSS) score before EVT and after 24 hours, intracranial occlusion location on CT angiography (CTA) or DSA, and technical variables for the procedure. All process times specific to the EVT procedure were calculated from source data. Complications in the EVAS registry are divided into procedural and post-procedural complications (online supplemental table 1). Recanalization rate was defined using the modified Treatment In Cerebral Infarction (mTICI) scale into successful recanalization (mTICI 2b–3) and failed recanalization (mTICI 0–2a). Functional outcome across the mRS (0–2, 3, 4, 5, 6) was collected through Riksstroke at 90 days. The mRS was estimated using a validated algorithm based on variables on dressing, toileting, mobility, living situation and need of help or support from next of kin, which has shown good accordance with objectively assessed mRS.12
Supplemental material
Missing data
Missing data included patients not returning the follow-up questionnaire, and missing or incomplete data for individual variables in registered patients. Since data on death were complete, not followed up patients were alive but with unknown functional status.
Statistics
We used IBM SPSS version 25. Descriptive statistics were presented as simple proportions and medians with IQRs and groups were compared using χ2 test, Mann-Whitney U test or Kruskal-Wallis test. Kaplan-Meier life tables were used to calculate mortality and groups were compared using the log-rank test. We used multiple imputation (MI) techniques (further described in the online supplemental appendix) to replace missing values for functional outcome in patients who were alive but lost to 90-day follow-up. The odds ratio (OR) with 95% confidence interval (95% CI) of achieving a favorable functional outcome was calculated using multivariate logistic regression analysis with and without adjustment for differences in baseline and treatment characteristics.
Results
EVT rate in Sweden within or beyond 6 hours
Between 2015 and 2020, the total number of IS cases registered in Riksstroke decreased from 19 750 to 17 243, while the total number of EVTs increased from 423 to 1022. The proportion of patients treated with EVT out of all patients with IS in Sweden is shown in figure 1A and was 5.9% in 2020. Early time window treatments increased from 1.4% of all IS in 2015 to 3.4% in 2020, corresponding to one EVT in every 30 IS patients. In the late time window (6–24 hours) the absolute increase is smaller, 0.3% of all IS in 2015 compared with 1.8% in 2020. EVT in late window patients with a known time of onset in the 6–24 hour interval increased from 0.1% of all IS in 2015 to 0.4% in 2020, and EVT in the late time window in patients LSW in the 6–24 hour interval increased from 0.2% of all IS in 2015 to 1.3% in 2020. In 2020, late window EVT was done in one in every 55 (1.8%) IS patients. A total of 14.7% of EVT patients had no registered time of onset or time of LSW and was therefore only included in the total EVTs in figure 1A.

Development of EVT in 2015–2020 in Sweden. (A) Proportion EVTs of all ischemic strokes. (B) EVTs in the early and late time window. (C) CTP use in the late time window patients with direct triage to CSC. (D) CTP use in late time window patients transferred from a PSC. CSC, comprehensive stroke center; CTP, CT perfusion; EVT, endovascular thrombectomy; IS, ischemic stroke; LSW, last seen well; PSC, primary stroke center.
Participants
A total of 2199 patients with anterior circulation LVO stroke in 2015–2020 were included for analysis (online supplemental figure 1). Late window patients accounted fo 23.1% (509/2199): 141 with a known time of onset, and 368 who were LSW in the 6–24 hour interval. During 2015–2020, 1690 (76.9%) patients were treated within 6 hours of onset, referred to as an early time window reference population.
Descriptive data of late window EVT in Sweden 2015-2020
Patients characteristics are shown in table 1. Median age was 73 years and 46.2% were female, without significant group differences. The rates of vascular risk factors did not differ significantly between the three groups: hypertension (55.5–60.9%), atrial fibrillation (41.8–46.7%), diabetes (15.5–16.7%), and previous stroke (10.8–12.9%).
Patient characteristics in 2199 patients with anterior circulation LVO stroke treated in the early (<6 hours) and late (6–24 hours) time windows. Missing data were <2% for all variables
In total, 38.5% (847/2199) were directly transported to a CSC and 61.3% (1347/2199) were transferred from a PSC. Most late window patients with a known time of onset (92.2%, 130/141) arrived by secondary transport from a PSC, and approximately half (52.5%) of the group received IVT, indicating that many arrived at a PSC within 4.5 hours.
At first imaging (CT and CTA in all cases), there was no difference in occlusion location between groups, but on DSA late window patients with known onset more commonly presented with M2 occlusions (late window known onset 39%, early window 29.4%, late window LSW 25%; p=0.039). They also presented with lower NIHSS score before the intervention (late window known onset 12, early window 16, late window LSW 15; p<0.001). Partial recanalization, defined as a more distal occlusion site on DSA than on CTA, was most common in late window known onset patients (17.7%, early window 14.9%, late window LSW 7.1%; p<0.001). Partial recanalization was significantly more common in IVT patients (19.3% (227/1175) vs 7.3% (75/1024); p<0.001), but without differences between the time window groups (p=0.513). While EVT technique did not differ between groups, use of general anesthesia was more common in late window patients with known onset (48.1%, early window 35.3%, late window LSW 38.6%; p=0.006).
Median 24 hour NIHSS score showed a small difference between groups, favoring early time window patients (6, late window known onset 7, late window LSW 8; p=0.002). The delta NIHSS score (pre-treatment–24 hours post-treatment) was 7 in early window patients, 2 in late window known onset patients, and 5 in late window LSW patients (p<0.001).
All-cause 90-day mortality and sICH rates did not differ between groups. Post-procedural complications (online supplemental table 1) occurred more often in early time window patients (31.8%, late window known onset 29.6%, late window LSW 22.9%; p=0.01), but procedural complications did not differ between groups.
Implementation of anterior circulation late window EVT
The proportion of late time window treatments increased from 17.4% (19/109) of all anterior circulation LVO EVTs in 2015 to 32.9% (174/528) in 2020 (figure 1B).
Of 509 patients treated beyond 6 hours, 134 (26.3%) arrived directly at a CSC, and 375 (73.7%) arrived by secondary transport from a PSC. In direct triage patients, CTP use in the late time window was high with a small decrease from 100% in 2015 to 90.2% in 2020 (figure 1C). At PSCs (n=375 patients), only a minority of late window patients had CTP (9.1% in 2015 and 16.4% in 2020), but a proportion may have arrived at the PSC within 6 hours. On arrival at the CSC after secondary transport, CTP was used in 72.3% of late window patients in 2015 and 52.3% in 2020 (figure 1D). In total, CTP was used for patient selection in 89.5% (17/19) in 2015 and 72.4% (126/174) of late window cases in 2020, whereas non-contrast CT was used in the remainder.
All-cause mortality
There was no difference in 90-day mortality between groups (p=0.854) (figure 2): early time window 15.8% (267/1690), late window known onset 14.2% (21/141), and late window LSW 16.3% (60/368). Overall, 90-day mortality was 15.7% in the late time window.
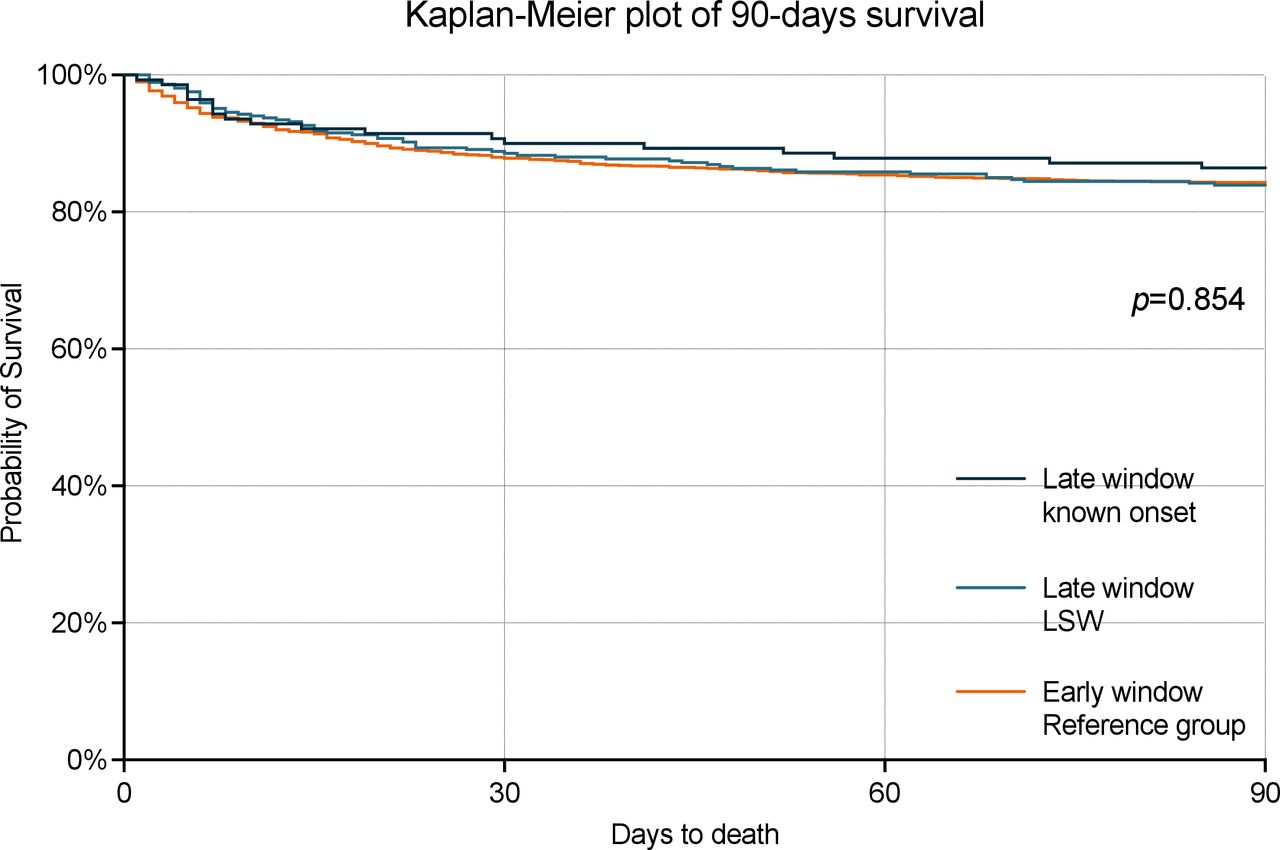
Mortality stratified by time window with no significant difference between groups (p=0.854). LSW, last seen well.
Functional outcome of late window EVT
The number of followed up patients was 1768/2199 (80.4%); 431/2199 (19.6%) were lost to follow-up. Baseline and treatment variables in followed up versus not followed up 90-day survivors are shown in online supplemental table 2. Patients lost to follow-up were on average 2.5 years younger and had less atrial fibrillation, otherwise there were no differences in patient or stroke characteristics between groups. Median 24 hour NIHSS was higher in those lost to follow-up (8 vs 6, p=0.005)
The distribution on the mRS at 90 days with missing data replaced by imputed values is shown in figure 3, and without imputed values in online supplemental figure 2. There was no significant difference in functional outcome between groups. A favorable clinical outcome was seen in 42.4% in the early time window, compared with 38.9% in late window known onset patients, and 37.3% of late time window LSW patients (p=0.737). The total rate of functional independence in the late time window was 37.8%. Compared with the early time window (reference group), the OR of achieving a favorable outcome in the late time window was similar (known onset 0.863, 95% CI 0.598 to 1.247; LSW 0.809, 95% CI 0.630 to 1.040). When adjusted for variables that were unevenly distributed between groups, but not directly associated with the time aspect but possibly with prognosis (occlusion location, NIHSS pre-treatment and type of anesthesia), the OR of achieving a favorable outcome remained similar between the early (reference group) and late time windows (known onset 0.681, 95% CI 0.463 to 1.003; LSW 0.781, 95% CI 0.602 to 1.013).

{kind=link}
{kind=link}
{kind=link}
90-day functional outcome stratified by time window. There was no significant difference between groups (p=0.737). Loss to follow-up (19.6%) were replaced by imputed values. LSW, last seen well.
Discussion
We report nationwide prospective observational data on the implementation of late time window EVT over the period 2015–2020. This dynamic period in stroke treatment started with the successful RCTs of early time window EVT13 and covers the first years after the DAWN and DEFUSE 3 trials7 8 followed by the introduction of CTP-based patient selection for late window EVT patients in guidelines.9 10 During this period, late time window EVT increased substantially in Sweden—from 17% of all anterior circulation stroke EVT procedures in 2015 to 33% in 2020—illustrating a readiness to accept the late window paradox.6 In 2020, 5.9% of all Swedish IS cases were treated with EVT, and approximately one third of those (1.8% of all IS) were treated in the late time window, contributing significantly to the expansion of EVT in general.
Most late window treatments (72%) were performed in patients with unknown time of symptom onset, LSW in the 6–24 hour interval, whereas most late window treatments in patients with known time of onset were attributed to long secondary transports from PSCs. Direct triage to CSCs in stroke patients with a high probability of LVO has been successfully implemented in parts of Sweden, which has led to shorter time to EVT without delaying IVT treatment.14 However, due to both geographical and infrastructural challenges, most Swedish EVT patients still arrive at the CSCs by secondary transport leading to a spill-over effect of patients presenting at PSCs in the early time window, but subsequent long transports result in late window EVTs.
The capacity at CSCs to select cases beyond 6 hours based on CTP in direct triage patients is high (>90%). In contrast, CTP is currently only used in a minority of late window cases (16%) at the PSCs and is subsequently used in approximately half of secondary transport patients on arrival at the CSC. It appears that the delay in introducing CTP in the workup at PSCs has partly been compensated for by a wide use of non-contrast CT only for late time window patient selection. Despite the introduction of new guideline recommendations for EVT in the late time window,9 10 CTP use decreased from 89.5% to 72.4% (−17.1%) between 2015 and 2020, a trend that is mainly explained by less repeated imaging in secondary transport patients arriving at comprehensive stroke centers. That, in turn, could be explained by the fact that repeated imaging causes delays,15 which may translate into poorer outcomes. The need for CTP in selecting patients for EVT in the late time window has been questioned in a recent study comparing patient selection based on CTP versus non-contrast CT only,16 showing no difference in 90-day clinical outcomes between groups selected based on CTP versus non-contrast CT only. Also, a comparison of aggregated data from the ESCAPE NA-1 (Safety and Efficacy of Nerinetide (NA-1) in Subjects Undergoing Endovascular Thrombectomy for Stroke) trial using non-contract CT-based patient selection, with the DAWN and DEFUSE 3 trials that used core-penumbra mismatch imaging, showed similar outcomes.17 In our study, the mRS distribution did not differ between patients selected by CTP and by non-contrast CT only (data not shown). MR CLEAN-LATE (a multicenter randomized clinical trial of endovascular treatment of acute ischemic stroke in The Netherlands for late arrivals) is currently evaluating the benefit of EVT in the late time window based on wider inclusion criteria.18
There was no significant difference in the proportion achieving a favorable outcome at 90 days between patients treated in the early and late time windows (42.4% vs 37.8%). When adjusting for baseline imbalances not directly associated with time from onset to groin puncture, the OR of achieving a favorable outcome remained similar between the early and late groups. In addition, there was no difference in all-cause mortality at 90 days after treatment between the early and late groups (15.8% vs 15.7%), or the proportion of sICH (4% vs 4.1%).
Our results show that treatment outcomes in nationwide routine clinical practice are well in keeping with the RCTs7 8 as well as the recent individual-level data AURORA (Analysis of Pooled Data from Randomized Studies of Thrombectomy More Than 6 Hours After Last Known Well) meta-analysis.19 The rate of functional independence in the AURORA meta-analysis EVT arm was 45.9%,19 while the corresponding rates in observational studies ranged from 24.5–62%.20–27 One recently published study on 53 702 EVTs in US clinical practice reported an equal proportion of late window EVTs (33%) to our nationwide material,28 while two other comparable studies presented lower proportions of late window treatments (10.7–11%).20 22 Contrary to our study, the US study found large baseline differences between groups and poorer outcomes in terms of in-hospital mortality and ambulation at discharge in late time window cases, although mRS at 90 days was not evaluated.
We observed that occlusion location did not differ between early and late window patients on first imaging (CTA) but did differ on DSA, where more distal occlusions were seen in late window patients with known onset, of whom 92% arrived by secondary transport and half were treated with IVT. In general, partial recanalization was significantly more common in patients treated with IVT. The time between start of IVT and groin puncture (NTG) may be an important factor for recanalization.
Limitations
We acknowledge that our study has several limitations. Loss to follow-up of 19.6% resulted in a high risk of attrition bias. Loss to follow-up patients were younger and with less atrial fibrillation but had a marginally higher 24 hour NIHSS score (8 vs 6). Replacement of missing data using MI (figure 3) compared with extrapolation of data from followed up survivors to those lost to follow-up (online supplemental figure 2) resulted in similar proportions of independent patients but slightly higher proportions of patients with severe dependency. It is expected that patients with severe dependency are less likely to be able to participate in follow-up. With the use of MI, any residual effect of attrition on the results is limited. Another limitation is that 14.7% of all EVTs had no registered OTG time and were therefore only included in the overall analysis on EVT in Sweden. Further limitations are that even though CTP was used in many cases, it is unknown to what extent it guided treatment decisions and which cut-offs were used, and that the recanalization rate is evaluated by the treating site and not by core-lab assessment. Finally, functional outcome was self-reported, making the results vulnerable to known limitations associated with self-reports, although self-reported functional outcome in Riksstroke has shown good accordance with objectively assessed mRS.12
Conclusions
This nationwide prospective observational study on implementation and current practice for late time window anterior circulation EVT, with >90% coverage, shows that treatment outcomes obtained in recent RCTs and meta-analyses are also achieved in routine clinical practice on a nationwide scale.
Our study demonstrates how quality registry data can be used to evaluate how the rapid development of stroke treatment research transfers into nationwide 24/7 routine care.
Supplemental material
Data availability statement
Data are available upon reasonable request. Requests to access an anonymized dataset supporting the conclusions may be obtained with an appropriate ethics approval.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Swedish ethical review authority; ethics approval ID: 2019/00678. Patients are informed of their participation in the quality registers including that data may be used for research purposes. Since the data were already collected and de-identified, the Swedish Ethical Review Authority therefore waived the need for individual patient consent.
Acknowledgments
We thank the Swedish Endovascular Stroke Treatment Collaboration, especially Åke Holmberg at EVAS and Fredrik Jonsson at Riksstroke. We are grateful to patients, caregivers, and staff for providing data in the registries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TU, MvE, PW, JW, FA, BN and TA researched the literature and conceived the study. TU is guarantor. TU and JW were involved in protocol development, gaining ethical approval. TU was responsible for data analysis. TU and JW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding This study was funded by regional ALF grants, the Crafoord Foundation and by SUS Stiftelser och Fonder.
Competing interests BN has received honoraria from AstraZeneca for serving on the DSMB for the THALES trial. TU has received honoraria from AstraZeneca for an expert group assignment. JW is a shareholder for UmanSense AB. FA has received grants from Stryker and Cerenovus. MvE receive honoraria from the Committee for Clinical Therapy Research. TA received honoraria from Anaconda, Cerenovus, Stryker. TA also received honoraria for serving on the DSMB for the Excellent registry, SPERO and Solonda studies, and is a shareholder on Rapid Medical and Ceroflo. PW is a clinical adjudication member in Portico 1 and Portico IDE phase IV studies supported from Abbott.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.