Article Text

Abstract
We report the usefulness of revision balloon kyphoplasty (re-BKP) and vertebra-pediculoplasty using cannulated screws (VPCS) for osteoporotic vertebral fractures (OVF) following cement dislodgement of conventional BKP. Between 2015 and 2020, three patients with OVF developed symptomatic cement dislodgement following BKP and underwent re-BKP. All three patients showed a loose cemented mass and spinal instability. Balloon inflation was performed in the gap between the loosened cemented mass and the remaining cortical bone rim, and this extended gap was filled with cement. To prevent re-dislodgement of the cement mass, a cannulated screw was inserted into the cemented mass through the pedicle. All patients achieved early pain relief, and improved vertebral stability of the fractured vertebra and all related symptoms, with no perioperative complications. Re-BKP and VPCS are innovative concepts and could be an effective minimally invasive treatment for OVF following cement dislodgement of conventional BKP treatment.
- Spine
- Trauma
- Technique
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Balloon kyphoplasty (BKP) was developed as a minimally invasive surgical technique for percutaneous vertebroplasty in patients with osteoporotic vertebral fractures (OVF) refractory to conservative treatment.1 However, cement dislodgement is reportedly a rare and vexing complication for clinicians. If it develops and becomes symptomatic, posterior fusion or a highly invasive combined anterior and posterior instrumentation surgery may be required.2
We report a new concept and method of revision BKP (re-BKP) and vertebra-pediculoplasty using cannulated screws (VPCS), wherein the fractured vertebral body is refilled with cement using a cannulated screw to stabilize the additional cement in the vertebral body, in cases of symptomatic cement dislodgement or refracture with instability after conventional BKP.
Case presentation
Case 1
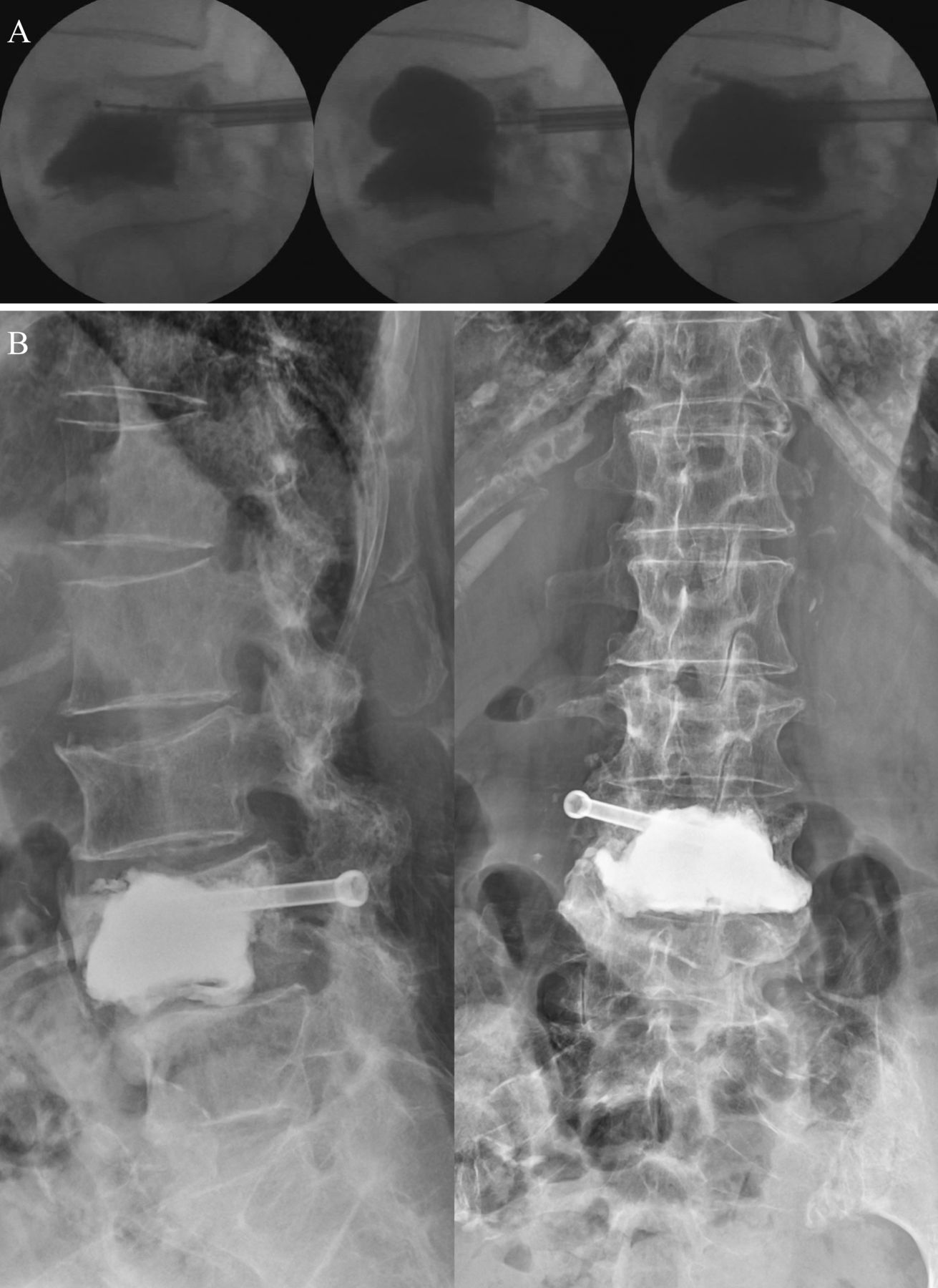
A patient in their 70 s developed a traumatic T11 OVF. BKP was performed 16 days after the injury. However, he developed worsening back pain. The treated vertebra showed residual instability on radiographs, and the CT scan showed a clear zone around the cement (figure 1). Re-BKP was performed under fluoroscopic control (figure 2). The balloon was inserted into the clear zone around the cement and dilated (right: 4 mL, left: 4 mL) to generate space for more cement. Cement was then filled from both sides for a total of 10.3 mL (see online supplemental video 1).
Supplementary video
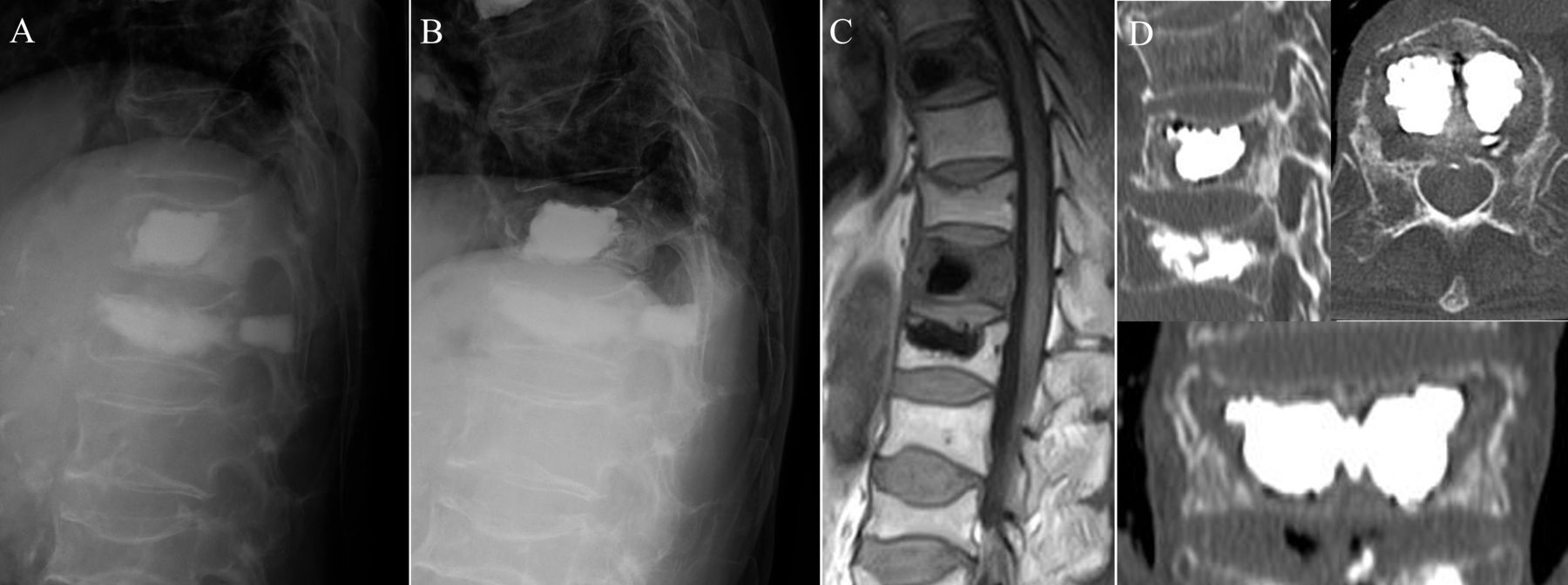
Case 1: images taken 18 days after the initial surgery. (A, B) Radiographs showing residual vertebral instability (A: supine, B: sitting). (C) Magnetic resonance T1-weighted image. (D) CT image showing a clear zone around the cement.

Case 1: intraoperative X-ray fluoroscopic images. (A) A balloon was inserted into the clear zone around the cement. (B) The balloon was expanded to make space for the cement. (C) Insertion of 10.3 mL of cement was performed. (D) CT scan taken 3 months postoperatively. (E) Seated radiographs taken 5 years postoperatively.
Case 2
A patient in their 70s sustained an L4 OVF after falling. BKP (using 10.4 mL of cement) was performed 3 weeks after the injury, with symptom resolution. Radiographs at 2 months postoperatively showed no vertebral instability (figure 3A). However, 4 months postoperatively, the patient experienced multiple falls, with subsequent back pain worsening. Radiographs and CT scan revealed a refracture of L4 and cement dislodgement (figure 3B,C). Re-BKP and VPCS was performed 2 weeks after the injury. The balloon was inserted into the clear zone around the cement and dilated. To prevent cement re-dislodgement, a 6.5 mm cannulated screw was replaced with a guide pin, and a total of 16 mL cement was introduced through the screw hole. Before the cement hardened, the cannulated screw was inserted into the vertebral body (figure 4A, see online supplemental video 1). As the cement hardened, the screw thread and cement were integrated.

Case 2: (A) Radiographs taken 1 week (left) and 2 months (right) after the initial surgery. (B) Radiographs 4 months after the initial surgery (left: supine; right: sitting position). (C) CT scan 4 months after the initial surgery.
Case 2: (A) Intraoperative X-ray fluoroscopic image. The balloon was expanded to make space for the cement, and 16 mL of cement was introduced. (B) Radiographs taken 1 year after the revision surgery (sitting position).
Case 3
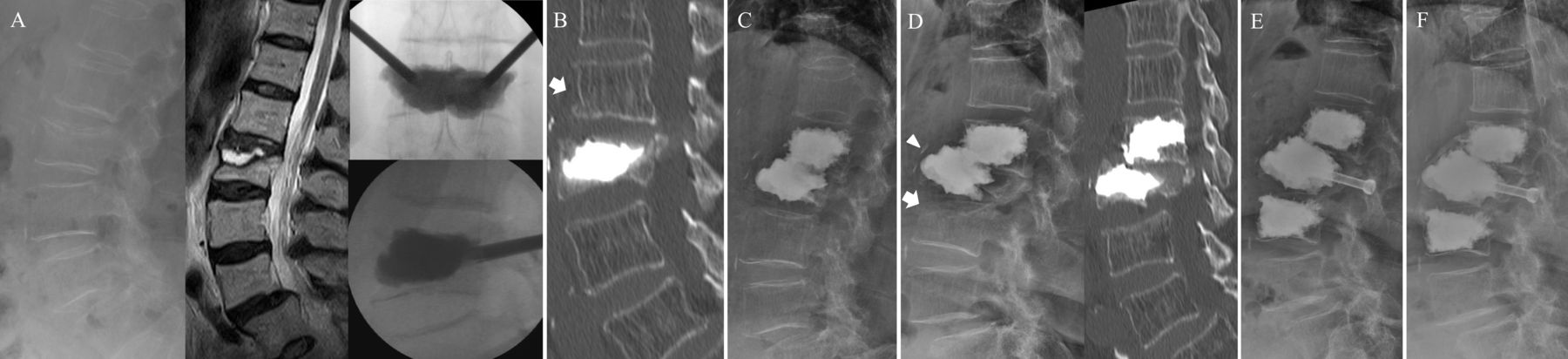
A patient in their 80s with Parkinson’s disease, developed spontaneous lower back pain without obvious trauma. L2 OVF was diagnosed, and BKP was performed 2 weeks after symptom onset (figure 5A). Three days postoperatively, she developed an L1 adjacent OVF (figure 5B). A second BKP was performed 1 week after the initial surgery with subsequent pain improvement (figure 5C). However, 2 months postoperatively, the patient complained of back and right thigh pain. Radiographs showed an adjacent OVF at L3 and cement dislodgement at L2 (figure 5D). Three months after the initial surgery, re-BKP and VPCS at L2 was performed with 10.5 mL of additional cement with screw augmentation (figure 5E, see online supplemental video 1). L3 BKP was also performed using 13.5 mL of cement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 3: (A) Preoperative radiograph, MRI image, and intraoperative X-ray fluoroscopic image at initial surgery. (B) CT image taken 3 days after initial surgery. CT revealed L1 adjacent vertebral fracture (white arrow). (C) Radiograph taken 6 weeks after second balloon kyphoplasty (BKP). (D) Radiograph (left) and CT image (right) taken 2 months after second BKP. L3 adjacent vertebral fracture (white arrow) and cement dislodgement (white arrowhead) was observed. (E) Radiograph taken 5 months after the third surgery. (F) Radiograph taken 2 years after the third surgery. Bridging callus formation and a well-stabilized spine were observed.
Outcome and follow-up
In all patients, the pain improved after the revision surgery with no postoperative complications. All patients were able to walk independently after surgery. Postoperative radiographs showed a well-reconstructed and stable vertebra with bone union and bridging callus formation after 5 years in case 1 (figure 2E), 1 year in case 2 (figure 4B), and 2 years in case 3 (figure 5F).
Discussion
‘Vertebra-pediculoplasty’, in which the vertebral pedicle is reconstructed with an artificial screw in addition to vertebroplasty was reported in 2006 and since then similar concepts of the procedure have been reported.3–6 In 2018, a new procedure using vertebral body stenting with screws was reported by Cianfoni et al with a concept similar to VPCS. In their report, percutaneous stent screw-assisted internal fixation (SAIF), whereby the vertebral body stenting/cement complex was anchored with pedicular screws to the posterior vertebral elements, was reported as a minimally invasive internal fixation technique.7 This technique is biomechanically advantageous over vertebral augmentation in significantly decreasing the strain distribution on the superior endplate and cortical wall, thus reducing refracture risk of the middle column at the treated level.8 The advantage of SAIF and VPCS is that by forming the vertebral pedicle, the cement mass is stabilized in the vertebral body with the lamina and pedicle as stoppers. This allows the cement to stabilize within the fractured vertebra even under load stress, thus preventing secondary cement dislodgement. This method is very effective for minimally invasive stabilization of complex fractured vertebrae where vertebroplasty alone does not provide early stability of the fracture. This method is innovative in that it can preserve the intervertebral space and does not cause adjacent segmental disorders, which may occur in spinal fusion surgery. Although this procedure could also be performed with a less costly vertebroplasty, the BKP system was used for revision surgery as it allowed the surgeon to evaluate the loosening of the cement mass, secure the cement filling space, and predict the cement filling volume based on the balloon expansion volume, as shown in our cases.
Learning points
Revision balloon kyphoplasty and vertebra-pediculoplasty using cannulated screws could become an excellent and practical technique to stabilize the affected vertebral body in osteoporotic vertebral fractures with cement dislodgement. This surgical procedure could be a useful way to avoid highly invasive instrumentation surgery.
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but In this study, written consent for surgery was obtained for each individual patient. The treatment methods used in this case report are methods that have already been reported in the past. The ethics committee determined that there was no need for them to review and apply for this surgery, as it is an application of a surgical procedure that has already been established in the past. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards, which exempted this study. Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YY: conceptualization, methodology, project administration, formal analysis, investigation, supervision, writing - review and editing. NY: Writing - original draft. YK, TY, and YK: Investigation. SD: writing - review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.