Article Text

Abstract
Background Endovascular treatment (EVT) for basilar artery occlusions (BAO) is associated with a higher rate of futile recanalization compared with anterior circulation procedures. We aimed to identify the incidence and predictors of poor clinical outcome despite successful reperfusion in current clinical practice.
Methods We used data from the ETIS (Endovascular Treatment in Ischemic Stroke) registry, a prospective multicenter observational registry of stroke treated with EVT in France. Patients undergoing EVT for acute BAO from January 2014 to May 2019 successfully treated within 8 hours from onset were included. Predictors of 90-day poor outcome (modified Rankin Scale (mRS) 4–6) were researched within patients with successful (modified Thrombolysis In Cerebral Infarction (mTICI 2b-3)) and excellent (mTICI 2c-3) reperfusion.
Results Among 242 patients treated within 8 hours, successful reperfusion was achieved in 195 (80.5%) and excellent reperfusion in 120 (49.5%). Poor outcome was observed in 107 (54.8%) and 60 (50%) patients, respectively. In patients with successful early reperfusion, age, higher initial National Institutes of Health Stroke Scale (NIHSS) score, lower posterior circulation Alberta Stroke Programme Early CT Score (pc-ASPECTS), and absence of prior intravenous thrombolysis were independent predictors of poor outcome. The only treatment factor with an independent predictive value was first-pass mTICI 2b-3 reperfusion (adjusted OR 0.13, 95% CI 0.05 to 0.37, p<0.001). In patients with excellent early reperfusion, independent predictors were age, initial NIHSS score, first-pass mTICI 2c-3 reperfusion, and hemorrhagic transformation on post-interventional imaging.
Conclusions Early successful reperfusion with EVT occurred in 80.5% of patients, and the only treatment-related factor predictive of clinical outcome was first pass mTICI 2b-3 reperfusion. Further research is warranted to identify the optimal techniques and devices associated with first pass reperfusion in the posterior circulation.
- Stroke
- Thrombectomy
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Key messages
What is already known on this topic
The proportion of patients with basilar artery occlusion who achieve favorable clinical outcome after endovascular therapy remains relatively low, despite high rates of arterial recanalisation within the early time window.
What this study adds
First pass reperfusion is a strong predictor of clinical outcome after endovascular treatment of basilar occlusions. In this study, it was the only treatment related factor with independent predictive value.
How this study might affect research, practice or policy
Further research is warranted to identify the optimal techniques and devices associated with first pass reperfusion in the posterior circulation.
Introduction
Basilar artery occlusion (BAO) stroke is associated with high rates of functional dependency and mortality.1 2 Endovascular treatment (EVT) is the standard of care for large vessel occlusion in the anterior circulation; however, conclusive evidence of clinical benefit in posterior circulation strokes is still lacking because these patients were excluded from the pivotal thrombectomy trials.3
Two randomized clinical trials4 5 failed to demonstrate a clinical benefit of EVT for BAO. In both of these trials—BASICS (Basilar Artery International Cooperation Study) and BEST (Basilar Artery Occlusion Endovascular Intervention Versus Standard Medical Treatment)—there was a relatively low proportion of good clinical outcome despite treatment in the early time window (up to 6 hours from symptom onset in BASICS, up to 8 hours in BEST) and relatively high reperfusion rates achieved in the EVT arms (Thrombolysis In Cerebral Infarction (TICI) 2b-3: 72% in BASICS, 71% in BEST). Good outcome, defined as 90-day modified Rankin Scale (mRS) score 0–3, was obtained in 44.2% and 44% of cases, respectively.
Similar clinical results have been observed in retrospective studies. Zi et al 6 reported a large prospective multicentric cohort including 647 patients treated with EVT for BAO. Most patients were treated in the early time window (71.6% within 6 hours, 87.1% within 9 hours), and TICI 2b-3 reperfusion was obtained in 80.7% of patients; however, a good outcome was observed in only 32% of cases.
Moreover, when compared with anterior circulation procedures, EVT for BAO could be associated with a higher rate of futile recanalization.7 Therefore, a better understanding of baseline and procedural factors associated with futile recanalization could potentially improve patient selection for future clinical trials and provide guidance in current clinical practice.
The ETIS (Endovascular Treatment in Ischemic Stroke) registry is a prospective multicentric observational cohort of patients treated with EVT for acute stroke in French comprehensive stroke centers. We aimed to investigate the incidence and predictors of poor outcome despite successful reperfusion of BAO with EVT, with or without prior thrombolysis, in patients treated within 8 hours after onset.
Methods
Data were extracted from the ETIS (NCT03776877) registry, a prospective, open, multicenter, observational registry for endovascular stroke interventions performed at 18 participating tertiary stroke centers in France. Patients were selected for EVT using local institutional protocols, without prespecified inclusion or exclusion criteria. Patients who underwent EVT for acute BAO from January 2014 to May 2019 were included in the study if: (1) BAO was angiographically proven; (2) femoral puncture was performed within 480 min from symptom onset; and (3) successful reperfusion was achieved at the end of EVT. Early treatment window was defined as the time from symptom onset to femoral puncture ≤8 hours. Successful reperfusion and excellent reperfusion were defined as modified TICI (mTICI) scales of 2b-3 and 2c-3, respectively, at the end of the procedure. Procedures and follow-up were carried out using standard-of-care recommendations. Patients’ baseline clinical and radiologic characteristics, procedure details, and outcomes were collected using standardized definitions.
Outcomes
The primary outcome was clinical status at 90 days. Poor outcome was defined as mRS 4–6. Hemorrhagic transformation at day 1 was quantified according to ECASS criteria (European Cooperative Acute Stroke Study). Functional outcome at 3 months was assessed by board-certified vascular neurologists during a routinely scheduled clinical visit or by a study nurse certified in administering the mRS during a standardized telephone interview if the patient was unable to attend a clinic visit. Imaging variables, including mTICI scores, were adjudicated by interventionists in the respective centers.
Statistical analysis
Quantitative variables are expressed as mean (SD) in case of normal distribution or median (IQR) otherwise. Categorical variables are expressed as numbers (percentage). Patients with successful reperfusion at the end of the procedure were divided into two groups according to clinical outcome at 3 months (mRS 4–6 vs mRS 1–3). Baseline characteristics were compared between these study groups using the Student t-test for Gaussian continuous variables, the Mann-Whitney U test for non-Gaussian continuous variables, or the χ2 test (or Fisher exact test when the expected cell frequency was <5) for categorical variables, as appropriate. For identification of outcome predictors, multiple regression models were fitted using the Akaike and Bayesian information criterion (AIC and BIC). All baseline characteristics and procedural metrics were included in the multivariable analyses.8 The same analyses were then performed in the group of patients with excellent reperfusion. Statistical testing was conducted at the two-tailed α level of 0.05. Data were analyzed using STATA software version 17 (StataCorp, TX).
Results
Population
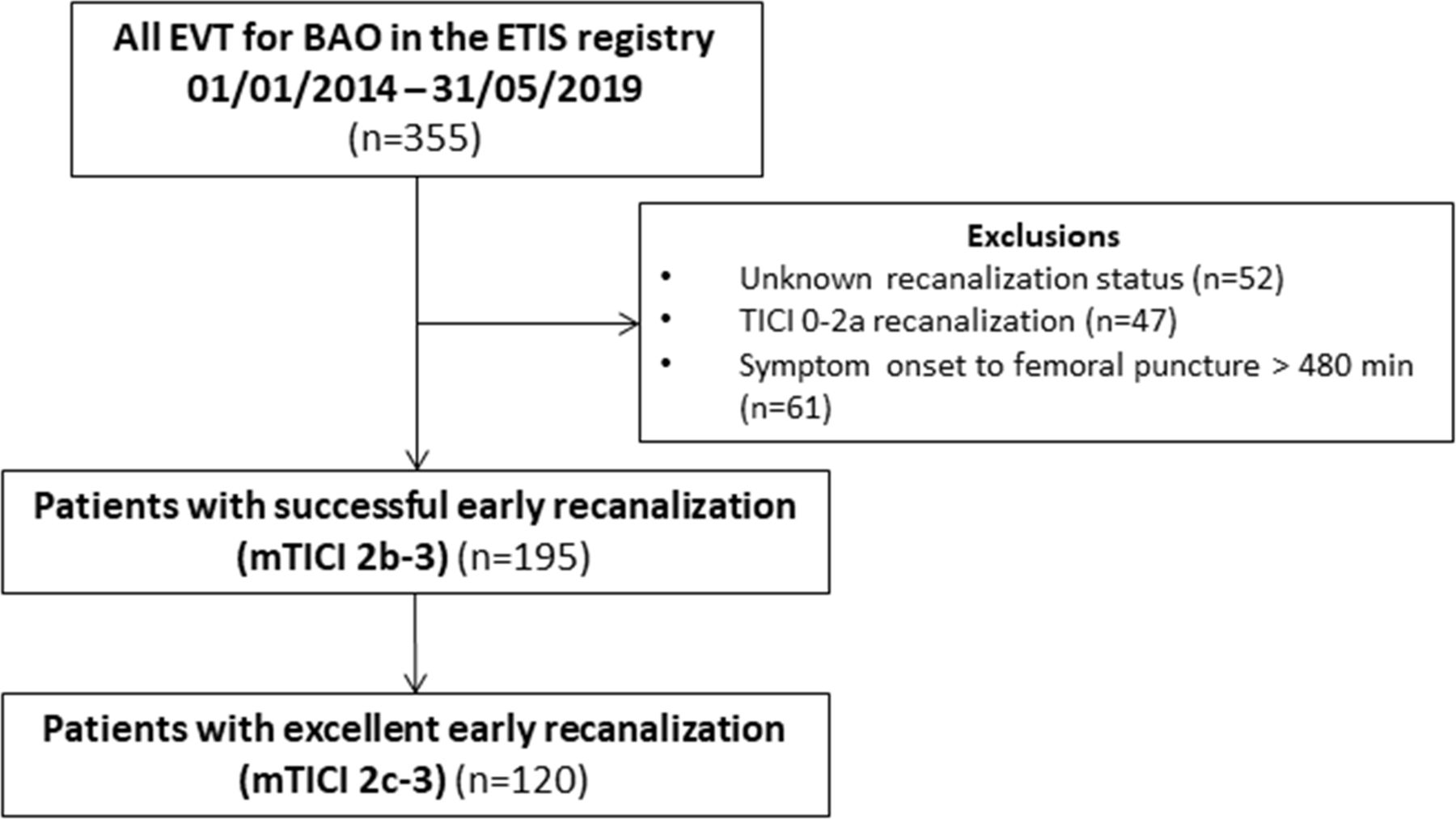
During the studied period, 355 patients who underwent EVT for BAO were identified in the ETIS registry. Figure 1 illustrates the flow chart of patient selection. Among patients with known reperfusion status, successful reperfusion was achieved in 84.4% (256/303). Successful reperfusion led to improved clinical outcomes: 45.1% of patients had favorable clinical outcome at 3 months compared with only 21% in case of failed (mTICI 0 to 2a) reperfusion (p=0.006). The rate of favorable clinical outcome was numerically lower in patients with mTICI 2b reperfusion compared with patients with excellent reperfusion (37.3% vs 50%); however, the difference did not reach statistical significance (p=0.103).
{kind=link}
Patient selection flowchart. BAO, basilar artery occlusions; ETIS, Endovascular Treatment in Ischemic Stroke; EVT, endovascular treatment; mTICI, modified Thrombolysis In Cerebral Infarction.
Contact aspiration was used as first line technique in the majority of cases (72.1%). Clinical outcome at 3 months was not significantly different according to the first line thrombectomy strategy: 44.1% favorable clinical outcome in the contact aspiration group versus 56.2% for stent retriever and 51.5% for combined technique (p=0.538).
EVT was initiated in the early time window (within 8 hours from symptom onset) and resulted in successful reperfusion in 80.5% (195/242) and excellent reperfusion in 49.5% (120/242). These two patient groups were included in the present study.
Baseline characteristics and procedural metrics according to clinical outcome are listed in table 1 for patients with successful reperfusion and in table 2 for patients with excellent reperfusion. Poor outcome was observed in 107 (54.8%) patients with successful early reperfusion and 60 (50%) patients with excellent early reperfusion. Mortality rates in the two groups were 73/195 (37.5%) and 42/120 (35%), respectively. Predictors of poor outcome in patients with successful and excellent reperfusion groups are detailed in table 3.
Baseline characteristics and procedural metrics in patients with successful reperfusion (mTICI 2b-3)
Baseline characteristics and procedural metrics in patients with excellent reperfusion (mTICI 2c-3)
Predictors of poor outcome despite early reperfusion
Predictors of poor outcome
In patients with successful early reperfusion, the following baseline characteristics were identified as independent predictors of poor clinical outcome: increasing age, higher initial NIHSS score, lower pc-ASPECTS score and absence of prior intravenous thrombolysis. The only treatment factor with independent predictive value was first pass mTICI 2b-3 reperfusion.
In patients with excellent early reperfusion, the following baseline characteristics were identified as independent predictors of poor clinical outcome: increasing age and higher initial NIHSS score. The only treatment factor with independent predictive value was first pass mTICI 2c-3 reperfusion. In addition, hemorrhagic transformation on post-interventional imaging was predictive of poor outcome in this group of patients.
Discussion
In the present large cohort of patients treated with early EVT, first pass mTICI 2b-3 reperfusion was the only treatment-related factor identified as an independent predictor of clinical outcome, in addition to several unmodifiable baseline characteristics.
The ETIS collaboration recently explored the effect of first pass reperfusion in posterior circulation strokes. In a multicentric cohort of 280 patients, Aubertin et al 9 showed that both first pass mTICI 2b-3 and mTICI 2c-3 reperfusion were associated with improved clinical outcome, compared with cases where the same degree of reperfusion was obtained after multiple passes or with the help of adjunctive treatments. Abdullayev et al 10 studied a small retrospective cohort of 56 patients with complete (TICI 3) reperfusion and observed that first pass reperfusion was an independent predictor of favorable clinical outcome.
These previous studies were designed to specifically assess the effect of first pass reperfusion, whereas in the present study we employed a different approach. In order to identify predictors of poor clinical outcome despite successful reperfusion, all available baseline variables were included, without prespecified criteria. In addition, the analysis was focused exclusively on patients treated within the early time window, in order to reduce the influence of time to treatment on clinical outcomes. By fitting multiple regression models, which included all baseline and procedural variables, we aimed to evaluate the relative importance of these factors and retain the ones with the best predictive value. The fact that first pass reperfusion emerged as the sole procedural factor with independent predictive value reinforces the role of this metric for EVT of BAO.
Of note, first pass complete (mTICI 3) reperfusion (also called true first pass effect) was included in our initial univariate analyses, but did not add additional predictive value compared with first pass mTICI 2b-3 and mTICI 2c-3 reperfusion, when the subsequent multivariable models were constructed.
One previous study7 researched predictors of futile recanalization (defined as mRS 3–6 at 3 months despite successful reperfusion) in a multicentric cohort of 165 patients treated with EVT for BAO. Age, baseline NIHSS score, and intracranial stenting were identified as independent predictors, whereas the number of device passes and pc-ASPECTS score did not remain significant in the multivariate analysis, possibly due to the smaller cohort size. Rates of first pass reperfusion were not reported and thus the predictive value of this variable was not explored.
The detrimental effect of repeated retrieval attempts on functional outcome has not yet been explained. Possible explanations include less distal emboli, intimal lesions, or the introduction of thrombus into perforator vessels.11 Pending the results of the future pc-ASTER trial, to date, data in the literature are insufficient to support a technical recommendation for a specific thrombectomy technique which might improve first-pass reperfusion rates. For anterior circulation occlusions, a recent large multicentric study12 found significantly higher first pass excellent reperfusion rates when combined stent retriever (SR)+contact aspiration (CA) technique was used as a frontline strategy, in conjunction with a balloon guide catheter, but this result was not replicated in other retrospective studies13 14 nor in the two ASTER (Contact Aspiration vs Stent Retriever for Successful Revascularization) randomized clinical trials (ASTER115 and ASTER216). For posterior circulation thrombectomies, a recently published multicentric cohort of 128 patients17 compared outcomes according to front-line technique (SR, CA, combined SR+CA). The highest numerical proportion of first pass complete reperfusion (mTICI 3) was observed in the combined SR+CA group; however, the differences did not reach statistical significance. The rates of first pass successful or excellent reperfusion were not reported in this study.
In a large multicentric cohort of 345 patients with posterior circulation occlusions,18 the use of CA was associated with higher rates of functional independence (mRS 0–2) compared with SR or combined techniques; however, the rates of first pass reperfusion were not reported. In the present study we did not find a significant correlation between first line thrombectomy technique and clinical outcomes.
There were several differences in predictors of outcome between the groups of patients with successful versus excellent reperfusion. Intravenous thrombolysis and pc-ASPECTS score did not remain significant in the group of patients with excellent reperfusion. It is possible that the importance of these variables was reduced by the achievement of excellent reperfusion in the early time window in this specific subgroup of patients. Conversely, one post-procedural factor emerged as significant predictor—the presence of hemorrhagic transformation on post-interventional imaging. This is concordant with previous studies both for posterior19 and anterior20 circulation thrombectomies.
The two main strengths of the present study are a dataset acquired through a multicentric registry of consecutive thrombectomy procedures, and the systematic independent 90-day follow-up with adjudication of clinical outcomes. There are, however, several limitations: the analysis was conducted retrospectively, treatment protocols and patient selection criteria varied between participating centers, and imaging data (including mTICI scoring) were not adjudicated by an independent core laboratory.
Conclusion
In this large cohort of BAO successfully treated with early EVT, the sole treatment-related factor predictive of clinical outcome was first pass reperfusion. Further research is warranted to identify the optimal techniques and devices associated with first pass reperfusion in the posterior circulation.
Supplemental material
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. We used data from the ETIS Registry (ClinicalTrials. gov Identifier: NCT03776877). Local institutional review boards in all participating centers approved data collection and analyses. Participants gave informed consent to participate in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RaoulPop25, @jildazz
Collaborators ETIS Registry Investigators: The names of all investigators are listed in the Appendix.
Contributors RP, SNF, BG: conception and design of the work, analysis and interpretation of data, drafting the manuscript, final approval of the version to be published, agreement to be accountable for all aspects of the work. CA, ME, ON, JD, FC, SR, GM, RB, IS, CD, RB, BL, AC, FE, SV, JC, CD, MB, MG, AR, FM, CR, GT, OO-W, J-FA, ALB, SE, VW, ST, J-CG, FB, LV, CP: acquisition and interpretation of data, critical revision of the manuscript, final approval of the version to be published, agreement to be accountable for all aspects of the work. Guarantor: BG.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests FC: Consulting fees from Medtronic, Stryker, Balt. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Penumbra, Balt, Medtronic. Participation on a Data Safety Monitoring Board or Advisory Board – Clinsearch. J-CG: Consulting fees from Medtronic, Stryker, Balt. Support for attending meetings and/or travel from Balt. Participation on a Data Safety Monitoring Board or Advisory Board – Intradys. AR: Consulting fees from Balt. IS: Consulting fees from Sanofi Synthé-Labo, Servier, Boheringer Ingelheim, Astra-Zeneca, Novonordisk, Medtronic. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Sanofi Synthé-Labo, Medtronic, Boheringer Ingelheim, Astra-Zeneca, BMS-Pfizer. GM: Consulting fees from Stryker. Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Medtronic, Microvention.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.