

- Hospital El Cruce Néstor Kirchner, Florencio Varela, Buenos Aires, Argentina
- Hospital de Clínicas José de San Martín, CABA, Argentina
Correspondence Address:
Javier Goland
Hospital de Clínicas José de San Martín, CABA, Argentina
DOI:10.4103/sni.sni_393_16
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Javier Goland, Gustavo Fabián Doroszuk, Silvia Lina Garbugino, María Paula Ypa. Transradial approach to treating endovascular cerebral aneurysms: Case series and technical note. 10-May-2017;8:73
How to cite this URL: Javier Goland, Gustavo Fabián Doroszuk, Silvia Lina Garbugino, María Paula Ypa. Transradial approach to treating endovascular cerebral aneurysms: Case series and technical note. 10-May-2017;8:73. Available from: http://surgicalneurologyint.com/surgicalint-articles/transradial-approach-to-treating-endovascular-cerebral-aneurysms-case-series-and-technical-note/
Date of Submission
08-Oct-2016
Date of Acceptance
09-Feb-2017
Date of Web Publication
10-May-2017
Abstract
Background:Several benefits have been described over the years of the transradial versus femoral endovascular approach to cardiac interventions. Consequently, its use has become habitual at most centers that perform cardiac catheterizations. This paper details a right transradial approach, incorporating a variety of coils or flow diverters, which can be utilized for the endovascular treatment of different cerebral aneurysms.
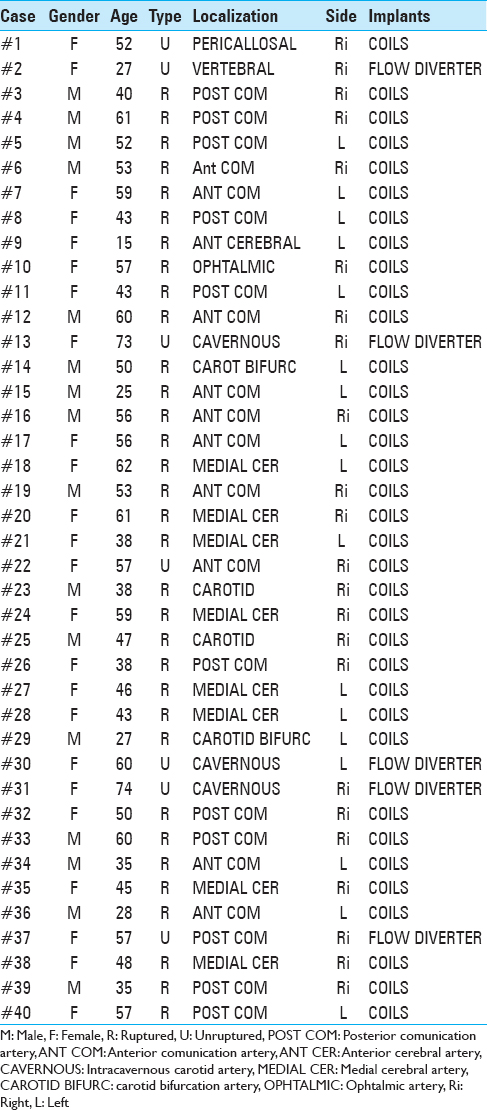
Methods:From 2014 to 2016, we performed 40 endovascular procedures to treat cerebral aneurysms adopting the same right transradial approach. Five aneurysms were treated with flow diverters and 35 were treated with coils. Seven of these aneurisms were asymptomatic, whereas 33 had already ruptured.
Results:Satisfactory treatment was achieved in all cases through the same approach in the absence of any complications.
Conclusions:A right transradial approach may be satisfactory for the endovascular treatment of different cerebral aneurysms, including aneurysms in either hemisphere. This is the largest series of cerebral aneurysms treated through a transradial approach.
Keywords: Cerebral aneurysms, embolization, transradial approach
INTRODUCTION
Endovascular treatment of cerebral aneurysms with coils constitute a recommendation type 1 class B in high volume centers for ruptured and unruptured aneurysms. The approach used in most medical centers for endovascular diagnosis and treatment of aneurysms is femoral puncture due to familiarity with this route.[
A retrospective study comparing cardiac catheterization through femoral artery vs radial artery found significant differences in the incidence of pseudoaneurysms in those performed via femoral artery vs radial artery punctured. Complications associated to femoral approach, both in diagnosis and therapy, are described in several articles, including bruising at the puncture site (1.3%), retroperitoneal hematomas (0.4%), pseudoaneurysm at the puncture site (0.1%), and arterial dissections (0.3%). A higher rate of complications were described in patients with anticoagulant and antiplatelet therapy. Furthermore, the presence of stenosis or atheromatosis aneurysms at iliac or aorta arteries hinder its catheterization through them. Once the procedure is completed, the manual compression of the groin is required in femoral approached patients for at least 10–20 minutes with subsequent pressure bandage, complete rest for 4 hours, and relative rest for 24 hours with the bandage. Despite these measures, other complications associated with this approach include, in addition to those previously mentioned, back pain, arteriovenous fistulas at the puncture site, femoral nerve injuries, chronic lower limb ischemia, and thromboembolism.[
Transradial approach for coronary angiography was described in 1989. Many benefits of this approach have been described against the femoral over the years, which generated the habitual use of it in most centers for cardiac angiography.[
There are several reports of series of cases of this approach for cerebral angiography and some reports of cases of acute ischemic stroke and aneurysms approached transradial because of impossibility of the femoral approach; however, there is no series of transradial approach for endovascular aneurysms treatment.[
We describe the technique utilized in a series of 40 cerebral aneurysms of diverse topographies through a right radial approach treated with coils or flow diverters at two medical centers. This is the largest series of endovascular aneurysms treatment done through a transradial approach described in neurosurgical literature.
MATERIALS AND METHODS
Under general anesthesia, 35 cerebral aneurysms were treated with coils and 5 aneurysms with flow diverters. The procedures were performed between 2014 and 2016 in two public hospitals situated in Buenos Aires. Patients with aneurysms amenable to be treated only with coiling or flow diverter device through a 6fr guide catheter or smaller were included in the study. Thirty-eight treatments were performed by two of the authors (JG and GD) in center 1 and the other two were performed by the authors (JG, SG and PY) in center 2. All patients were approached through a right radial artery puncture. 8 aneurysms had been diagnosed on a previously study and an angiography and embolization were performed at the same study on the others 32. There were 33 symptomatic aneurysms and seven unruptered aneurysms [
All patients signed informed consent or responsible family if they were unable to do so before the study.
We performed Allen Test in half of the cases of our serie to evaluate collateral circulation. From June 2015, we discontinued the test because studies revealed no significant differences in safety regardless of the Allen's Test result.[
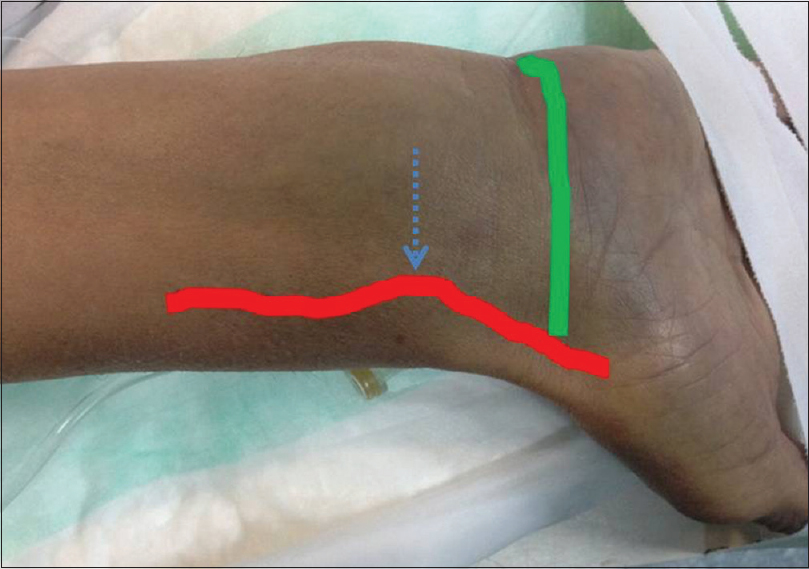
Under general anesthesia, we performed a Seldinger double-wall technique at a point located 3 cm proximal to the wrist, using a 21-gauge micropuncture needle [

A Simmons II catheter (Merit Medical Systems, Utah, USA) was used to perform three vessel studies previous to treatments. Some arteries approached directly with the guide without forming Simmons catheter [

Figure 3
Right vertebral and carotid arteries approached directly with guidance. (a) the guide wire inside the right vertebral artery; (b) contrast injection indicates the right vertebral artery; (c) the guide wire inside the right external carotid artery; (d) contrast injection inside the right common carotid artery
After diagnosis, an exchange on a 260 cm hydrophilic guide were done in the corresponding external carotid artery for aneurysm to treat. For adressing aneurysms through the right vertebral artery we entered directly with the guide catheter to the right vertebral artery. No aneurysms addressed by left vertebral artery in our series. We utilized three trademarks of guide catheters for these serie: DAC 5F (Concentric Medical, Mountain View, CA, USA), Fargomax 6F (Balt Extrusion, Montmorency, France) and Guider Softip XF 6F (Stryker, Neurovascular Fremont, Ca).
Using fluoroscopic and roadmap guidance, a 6Fr guide catheter was advanced over an angled glidewire into the propper artery and then the microcatheter was advanced up to the aneurysm. Four different microcatheters were used depending on the type of coil or flow diverter used: Headway 17 and 27 (MicroVention Inc., Tustin, CA), Excelsior SL10, (Stryker, Neurovascular Fremont, Ca), Vasco 27 (Balt Extrusion, Montmorency, France). Coils used were: GDC (Stryker, Neurovascular Fremont, Ca), Barricade coil system (Blockade, Irvine CA). Flow diverters used were Fred (MicroVention Inc., Tustin, CA), Surpass (Stryker, Neurovascular Fremont, Ca), Silk (Balt Extrusion, Montmorency, France), and Derivo (Acandis GmbH & Co KG Pforzheim, Germany).
Once the procedure was concluded, radial sheat was removed without reversing heparin, leaving a direct compression over the puncture site after irrigation through the side via the same with 5cc of Nitroglycerin (200 μg/mL).[

RESULTS
Thirty-nine anterior circulation aneurysms and one vertebral aneurysms were treated through this approach; 23 right and 17 left aneurysms. Twenty-four of the patients undergoing transradial approach were women. The average age was 48.5 years [
DISCUSSION
Radial approach for coronary procedures is widespread worldwide. There are large series of transradial cerebral angiographies and some case reports of endovascular treatments of posterior circuit aneurysms. The systematic use of this approach for endovascular treatment of anterior circuit intracranial aneurysms has not yet achieved the same acceptance than coronary studies. There are many advantages of transradial access with respect to the transfemoral approach; radial artery is more superficial than femoral and liable location of it and its adjacent structures has no risk of injury. Radial artery is easily compressible, with less risk of bleeding post-procedure, and this approach was associated with fewer complications.[
There are reports of hand ischemia occurring following cannulation of the radial artery for hemodynamic monitoring in critically ill patients for more than 20 hours; however, this complication has not been reported thus far after transradial coronary procedures. Documentation of patent ulnar artery and palmar arch has been tested performing Allen Test. Maniotis et al. presented a prospective data collection of 1035 consecutive patients who had underwent transradial approach procedures performed irrespective of the results of Allen's test, and no significant differences in clinical evolution with or without radial thrombosis were observed.[
Radial approach allows early ambulation and diminished costs in cardiac catheterizated patients.[
In our study, we were able to treat different aneurysms from diverse topographies and both sides with a high rate of efficiency and without complications [

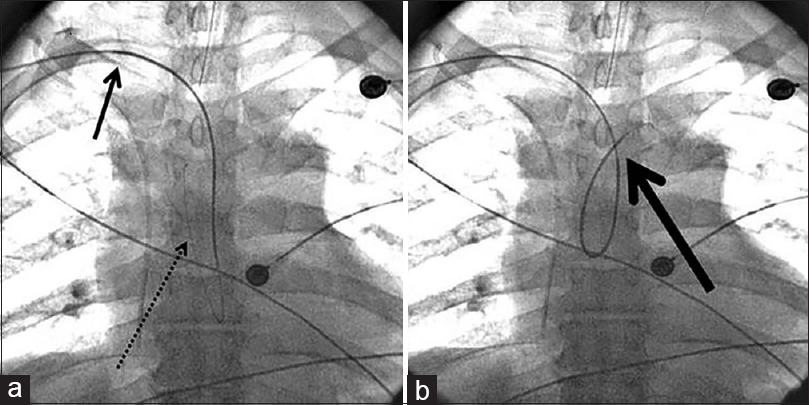
Figure 6
Final control angiography in two cases. Large arrows indicate the brachial approach of the catheter guide in both cases. (a) (case #16): The thin arrow indicates a right anterior communicating artery aneurysm treated with coils. (b) (case #18) The thin arrow indicates a left medial cerebral artery aneurysm treated with coils
Moreover, as remarkable features of this study, procedures were performed with different trademarks materials showing the versatility of this approach.
CONCLUSIONS
Transradial approach was utilized for endovascular treatment of multiple cerebral aneurysms with a satisfactory result. These treatments were performed with several trademarks catheter systems for both flow diverter and coils treatment. We did not observe arterial injuries nor technical limitations for this approach.
Financial support and sponsorship
Nil.
Conflicts of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with financial interest (such as honoraria, educational grants, participation in speakers bureaus, membership, employment, consultancies, stock ownership, or other equity interest, or expert testimony or patent-licensing arrangements), and no financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in subject matter or materials discussed in this manuscript.
References
1. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, Turri M, Anselmi M. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; Systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol. 2004. 44: 349-56
2. Bakhshi F, Namjou Z, Andishmand A, Panabadi A, Bagherinasab M, Sarebanhassanabadi M. Effect of positioning on patient outcomes after coronary angiography: A single-blind randomized controlled trial. Nurs Res. 2014. 22: 45-50
3. Benit E, Vranckx P, Jaspers L, Jackmaert R, Poelmans C, Coninx R. Frequency of a positive modified Allen's test in 1,000 consecutive patients undergoing cardiac catheterization. Cathet Cardiovasc Diagn. 1996. 38: 352-4
4. Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn. 1989. 16: 3-7
5. Connolly ES, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage. A Guideline for Healthcare Professionals From the American Heart. Association/American Stroke Association. Stroke. 2012. 43: 1711-37
6. Cooper CJ, El-Shiekh RA, Cohen DJ, Blaesing L, Burket MW, Basu A. Effect of transradial access on quality of life and cost of cardiac catheterization: A randomized comparison. Am Heart J. 1999. 138: 430-6
7. Cox N. Managing the femoral artery in coronary angiography. Heart Lung Circ. 2008. 17: S65-9
8. Eichhofer J, Horlick E, Ivanov J, Seidelin PH, Ross JR, Ing D. Decreased complication rates using the transradial compared to the transfemoral approach in percutaneous coronary intervention in the era of routine stenting and glycoprotein platelet IIb/IIIa inhibitor use: A large single-center experience. Am Heart J. 2008. 156: 864-70
9. Esente P, Giambartolomei A, Simons AJ, Levy C, Caputo RP. Overcoming vascular anatomic challenges to cardiac catheterization by the radial artery approach: Specific techniques to improve success. Catheter Cardiovasc Interv. 2002. 56: 207-11
10. Hildick-Smith DJ, Lowe MD, Walsh JT, Ludman PF, Stephens NG, Schofield PM. Coronary angiography from the radial artery--experience, complications and limitations. Int J Cardiol. 1998. 64: 231-9
11. Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P. Radial Versus Femoral Access for Coronary Angiography and Intervention in Patients with Acute Coronary Syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet. 2011. 377: 1409-20
12. Kiemeneij F, Laarman GJ, de Melker E. Transradial artery coronary angioplasty. Am Heart J. 1995. 129: 1-7
13. Kim JH, Park YS, Chung CG, Park KS, Chung DJ, Kim HJ. Feasibility and utility of transradial cerebral angiography: Experience during the learning period. Korean J Radiol. 2006. 7: 7-13
14. Jo KW1, Park SM, Kim SD, Kim SR, Baik MW, Kim YW. Is Transradial Cerebral Angiography Feasible and Safe? A Single Center's Experience. J Korean Neurosurg Soc. 2010. 47: 332-7
15. Lee DH, Ahn JH, Jeong SS, Eo KS, Park MS. Routine transradial access for conventional cerebral angiography: A single operator's experience of its feasibility and safety. Br J Radiol. 2004. 77: 831-8
16. Lee M, Applegate B, Rao S, Kirtane A, Seto A, Stone G. Minimizing femoral artery access complications during percutaneous coronary intervention: A comprehensive review. Catheter Cardiovasc Interv. 2014. 84: 62-9
17. Levy EI, Boulos AS, Fessler RD, Bendok BR, Ringer AJ, Kim SH. Transradial cerebral angiography: An alternative route. Neurosurgery. 2002. 51: 335-40
18. Lotan C, Hasin Y, Mosseri M, Rozenman Y, Admon D, Nassar H. Transradial approach for coronary angiography and angioplasty. Am J Cardiol. 1995. 76: 164-7
19. Louvard Y, Krol M, Pezzano M, Sheers L, Piechaud JF, Marien C. Feasibility of routine transradial coronary angiography: A single operator's experience. J Invasive Cardiol. 1999. 11: 543-8
20. Ludman PF, Stephens NG, Harcombe A, Lowe MD, Shapiro LM, Schofield PM. Radial versus femoral approach for diagnostic coronary angiography instable angina pectoris. Am J Cardiol. 1997. 79: 1239-41
21. Maniotis C, Koutouzis M, Andreou C, Lazaris E, Tsiafoutis I, Zografos T. Transradial Approach for Cardiac Catheterization in Patients with Negative Allen's Test. J Invasive Cardiol. 2015. 27: 416-20
22. Matsumoto Y, Hongo K, Toriyama T, Nagashima H, Kobayashi S. Transradial approach for diagnostic selective cerebral angiography: Results of a consecutive series of 166 cases. AJNR Am J Neuroradiol. 2001. 22: 704-8
23. Nohara AM, Kallmes DF. Transradial cerebral angiography: Technique and outcomes. AJNR Am J Neuroradiol. 2003. 24: 1247-50
24. Ricci MA, Trevisani GT, Pilcher DB. Vascular complications of cardiac catheterization. Am J Surg. 1994. 167: 375-8
25. Saito S, Ikei H, Hosokawa G, Tanaka S. Influence of the ratio between radial artery inner diameter and sheath outer diameter on radial artery flow after transradial coronary intervention. Catheter Cardiovasc Interv. 1999. 46: 173-8
26. Schonholz C, Nanada A, Rodriguez J, Shaya M, Dágostino H. Transradial approach to coils embolization of an intracranial aneurysm. J Endovasc Ther. 2004. 11: 411-3
27. Thompson BG, Brown RD, Amin-Hanjani S, Broderick JP, Cockroft KM, Connolly ES. Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015. 46: 2368-400
28. Wu CJ, Hung WC, Chen SM, Yang CH, Chen CJ, Cheng CI. Feasibility and safety of transradial artery approach for selective cerebral angiography. Catheter Cardiovasc Interv. 2005. 66: 21-6

