Article Text

Abstract
Background Endovascular treatment of intracranial aneurysms relies on coaxial catheter support systems to provide safe and stable access. Large-bore distal intracranial catheters have become necessary for aneurysm treatment with flow diverting devices including the Pipeline embolization device (PED). These catheters must accommodate 0.027 inch microcatheters, be supple enough to track distally and be able to provide sufficient support for manipulations required for PED deployment.
Methods A single-center aneurysm database was reviewed to identify patients who underwent anterior circulation aneurysm embolization with the PED while using the Navien distal intracranial catheter. Data were collected regarding the equipment used, cervical internal carotid artery (ICA) tortuosity, intraprocedural Navien positions and periprocedural complications.
Results The Navien catheter (5 Fr, 0.070 inch outer diameter, 0.058 inch inner diameter, 115 cm) was used in 78 cases of anterior circulation PED. It was tracked into position over a Marksman microcatheter in 76 of the 78 cases (97%). The final catheter tip position was in the cervical ICA (1/78, 1%), petrous ICA (23/78, 30%), proximal cavernous ICA (48/78, 62%), distal cavernous/clinoidal ICA (3/78, 4%), supraclinoid ICA (2/78, 2%) and the M1 segment (1/78, 2%). In each case the catheter was tracked to its desired position (100% clinical success) despite significant proximal vessel tortuosity in 34 cases (44%). No clinically significant catheter-related complications occurred.
Conclusions The Navien intracranial catheter is an important component of the triaxial system for embolization of cerebral aneurysms with the PED. This catheter is highly trackable to distal positions, atraumatic and provides sufficient support for the microcatheter manipulations used during typical PED deployments.
- Aneurysm
- Catheter
- Device
- Flow Diverter
- Intervention
Statistics from Altmetric.com
Introduction
Successful endovascular treatment of intracranial aneurysms and other vascular pathologies of the brain rely on coaxial catheter support systems to provide safe stable access to the intracranial circulation. In general, increased guide catheter support is required for procedures with larger device delivery systems, tortuous anatomy and distal targets. Classic guide catheters are large in size and rigid in design, and these catheters are generally limited in position to the cervical internal carotid artery (ICA). Technological advances have led to a newer generation of distal guide and access catheters that have more supple distal ends, thereby allowing the catheter to navigate further into the intracranial circulation. Previous reports have demonstrated the effectiveness of the Neuron1–5 and the Outreach distal access catheter (DAC)6–8 for a variety of neurointerventional procedures.
The introduction and now widespread use of flow diverting devices, including the Pipeline embolization device (PED; Covidien Vascular Therapies, Mansfield, Massachusetts, USA), for the treatment of intracranial aneurysms has resulted in a need for more robust access platforms. This is secondary to the comparatively larger size of the Pipeline delivery catheter (0.027 inch inner diameter (ID)) and the significant intradeployment manipulations required for proper device implantation. As such, there has been a paradigm shift in the design and approach to catheter support systems for cases of Pipeline embolization from a classic biaxial set-up to a more robust triaxial system.9 Distal intracranial catheters now serve as the cornerstone of these triaxial set-ups.
The Navien 5 Fr, 0.058 inch ID catheter (formerly the ReFlex Intracranial Catheter; Covidien Vascular Therapies, Mansfield, Massachusetts, USA) is a newer generation distal intracranial catheter that is highly trackable and atraumatic with a large-bore lumen that can accommodate 0.027 inch ID delivery catheters with added room for flush and injections. In this report we summarize our experience using the Navien catheter in 78 cases of Pipeline embolization of anterior circulation aneurysms. To our knowledge, this is the first such report on the systematic utilization of the Navien catheter for intracranial procedures, particularly with respect to aneurysm treatment with flow diverters.
Methods
Patient selection
We retrospectively reviewed the records of a prospectively collected single-center aneurysm database to identify all cases in which the Navien catheter was used during Pipeline embolization of an anterior circulation aneurysm from August 2011 (date of first Pipeline embolization at our institution) until December 2012.
Endovascular procedure
Pipeline embolization procedures were performed as previously described.9 Triaxial systems were used through femoral access. These consisted of a Flexor Shuttle sheath 0.087 inch ID (Cook Medical, Bloomington, Indiana, USA) or a Neuron MAX 0.088 inch ID (Penumbra, Alameda, California, USA), a Navien 0.058 inch ID distal intracranial catheter (Covidien Vascular Therapies) and a microcatheter 0.027 inch ID. The microcatheters used included the Marksman (Covidien Vascular Therapies) and the XT-27 0.027 inch ID catheter (Stryker, Kalamazoo, Michigan, USA). The Navien catheter is shown in figure 1.
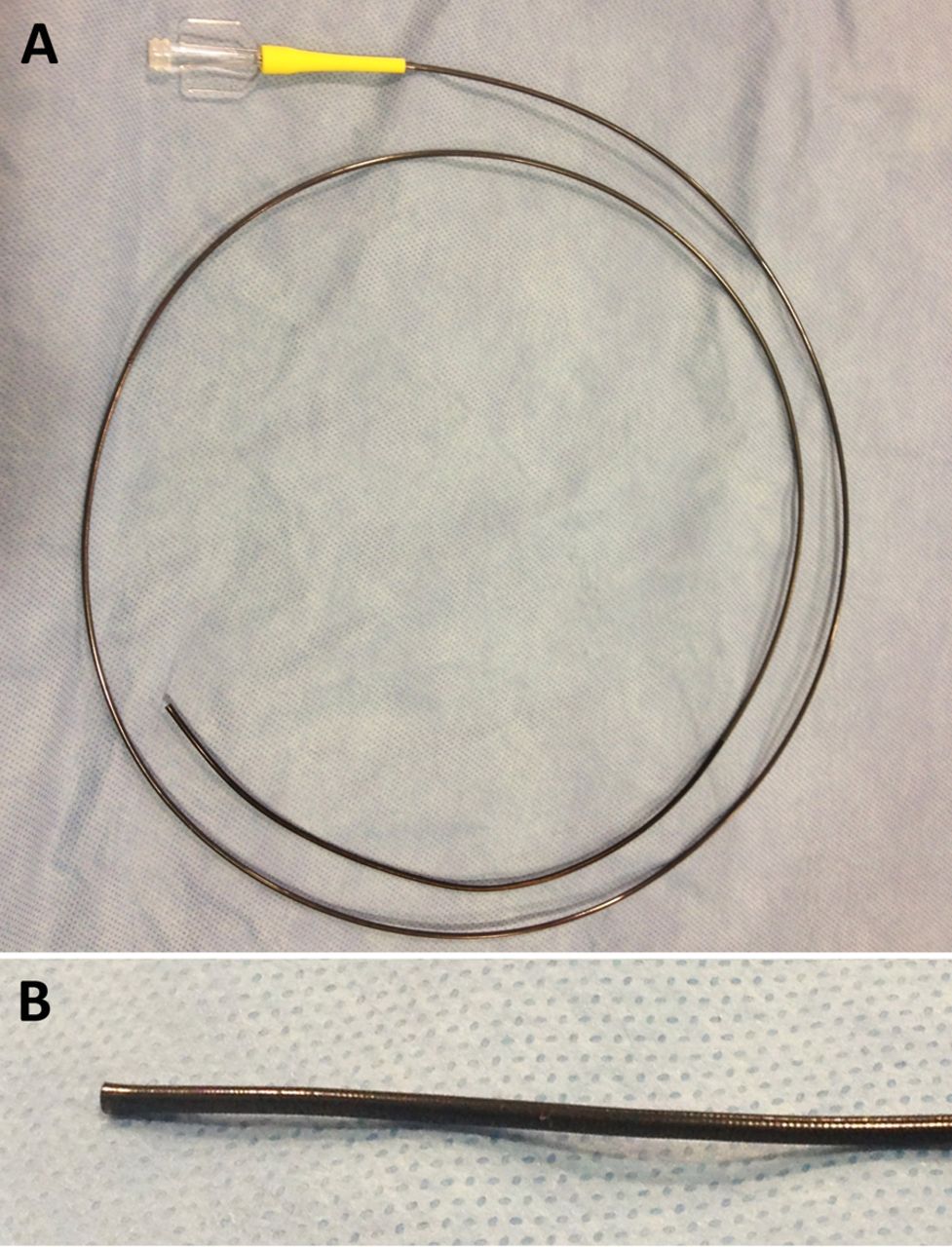
Navien distal intracranial catheter. (A) Image of the Navien 5 Fr outer diameter, 0.058 inch inner diameter, 115 cm version of the catheter. (B) Magnified view of the distal tip. The distal 8 cm is flexible.
Data collection and statistical analysis
Data were collected with respect to patient demographics, aneurysm characteristics, procedural equipment, guide catheter position, tortuosity of the parent vessel (defined as a 90° turn, hairpin turn or corkscrew loop) and guide catheter-related complications. Data were presented as counts, percentages and means. When means were presented, the SEM was used to assess sample distribution.
Results
Patient and aneurysm characteristics:
From August 2011 to December 2012 the Navien was used as a distal intracranial catheter in 71 patients (mean age 53.2±1.6 years, range 19–80) with anterior circulation aneurysms who underwent Pipeline embolization. The characteristics of these patients and the aneurysms are presented in table 1. Seventy-eight cases were performed, treating a total of 84 anterior circulation aneurysms with a mean size of 8.0±0.6 mm (range 3–26). Most of the 84 aneurysms were located in the paraophthalmic/clinoidal ICA (49/84, 59%) and cavernous ICA (21/84, 25%). Smaller numbers of aneurysms were located along the supraclinoid ICA (5/84, 6%), petrous ICA (2/84, 2%), ICA termination (1/84, 1%), anterior cerebral artery (ACA) (5/84, 6%) and middle cerebral artery (MCA) (1/84, 1%). None of the patients treated in this series presented with subarachnoid hemorrhage. None of the patients in this series had pre-existing indwelling endoluminal devices.
Patient demographic data and aneurysm characteristics
Access systems and equipment
The access systems and catheters used for the 78 cases are presented in table 2. A triaxial support system, with the Navien as the distal access catheter, was used in all 78 cases (100%). This high percentage of cases using triaxial support is consistent with our previously reported series of Pipeline embolization.9 In each case the Navien was tracked over a 0.027 inch ID microcatheter with an endoluminal 0.014 inch microwire to reach its final position. The Marksman microcatheter was used for tracking in 76 of the 78 cases (97%) and the XT-27 microcatheter was used in two (3%). In all cases, a Synchro-2 standard microwire (Stryker) was positioned at the tip of the microcatheter when the Navien was tracked.
Access systems and catheters used
Vessel tortuosity, guide catheter positions and clinical success
The tortuosity of the cervical ICA, the most distal position of the Navien tip, and the rate of clinical success are presented in table 3. Significant cervical ICA tortuosity was present in 34 of the 78 cases (44%). Tortuosity was defined as a 90° turn, hairpin turn or corkscrew loop, and a typical example of defined significant cervical ICA tortuosity is shown in figure 2. The most extreme tortuosity encountered during the study was a patient with two complete corkscrew loops in the cervical ICA (not shown).
Vessel tortuosity, guide catheter position and clinical success

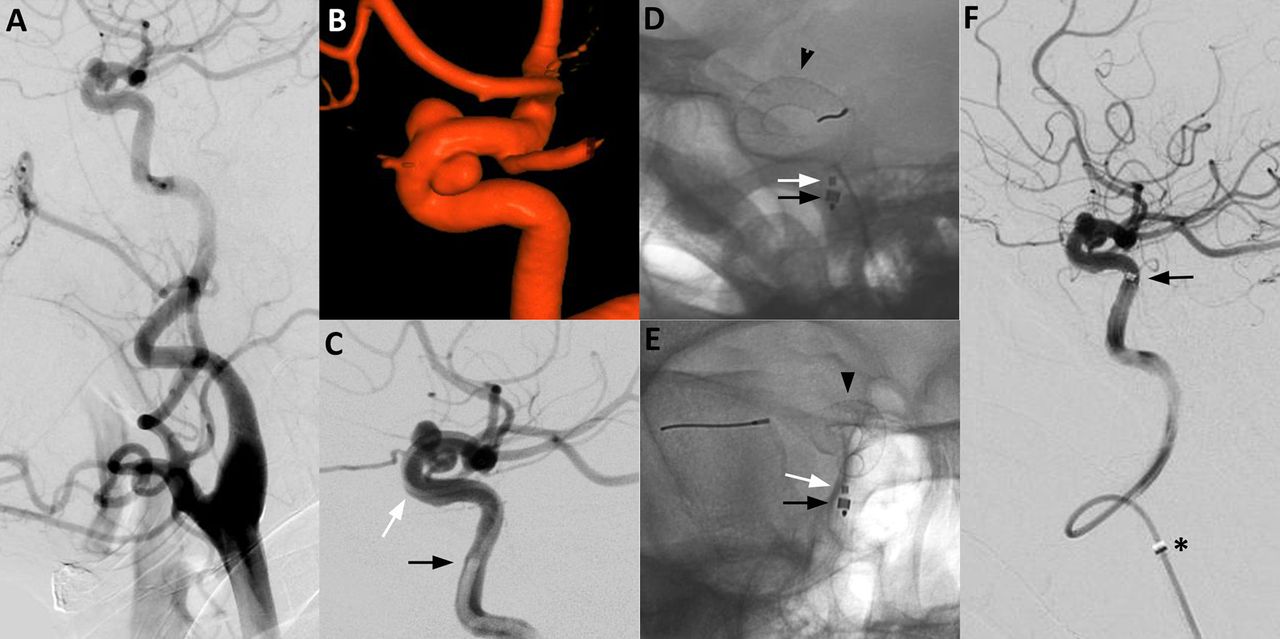
Proximal cavernous internal carotid artery (ICA) Navien support during Pipeline embolization of a 10 mm paraophthalmic aneurysm in a 61-year-old patient with significant mid-cervical ICA tortuosity. (A) Right common carotid artery pre-embolization digital subtraction angiogram (DSA) showing significant tortuosity of the mid-cervical ICA. (B) 3D-rotational reconstructed images showing the 10 mm paraophthalmic right ICA aneurysm. (C) Right ICA angiography during positioning of the Navien catheter (black arrow shows tip of Navien) in the cavernous ICA. The white arrow points to the Marksman catheter that was used for tracking the Navien and deployment of the Pipeline embolization device (PED). Post-PED deployment, single shot native fluoroscopy images in (D) lateral and (E) transorbital oblique views demonstrate the Navien positioned in the distal vertical portion of the cavernous ICA. The black arrow shows the tip of the Navien, the white arrow shows tip of the Marksman and the black arrowhead shows the deployed PED. (F) Control DSA injection of the right ICA performed from the Navien catheter after PED implantation. The Navien catheter (black arrow shows tip) is seen conforming to the anatomy of the tortuous mid-cervical ICA. The asterisk marks the tip of the Cook shuttle catheter just distal to the carotid bulb.
For the majority of cases, the Navien tip was positioned in the proximal cavernous ICA (48/78 cases, 62%), defined as the vertical cavernous segment up to and including the posterior genu. This was the Navien position of choice for treatment of most paraophthalmic aneurysms in our series. The next most common position for the Navien was in the petrous ICA (23/78, 30%), with each of these cases in the horizontal segment of the petrous segment. This was the catheter position of choice for treatment of cavernous ICA aneurysms. In addition, the Navien tip was positioned in the distal cavernous/clinoidal ICA in three cases (4%), supraclinoid ICA in two cases (2%), MCA in one case (1%) and cervical ICA in one case (1%). Representative cases of Navien positioning in the proximal cavernous, distal cavernous and supraclinoid ICA are shown in figures 2⇓–4, respectively. In all 78 cases, including the case with double corkscrew loops, the Navien was able to track smoothly over the microcatheter to its intended target position, representing a clinical success of 100%. However, PED deployment was unsuccessful in 3/78 cases (4%) secondary to inability of the device to open (device failure).

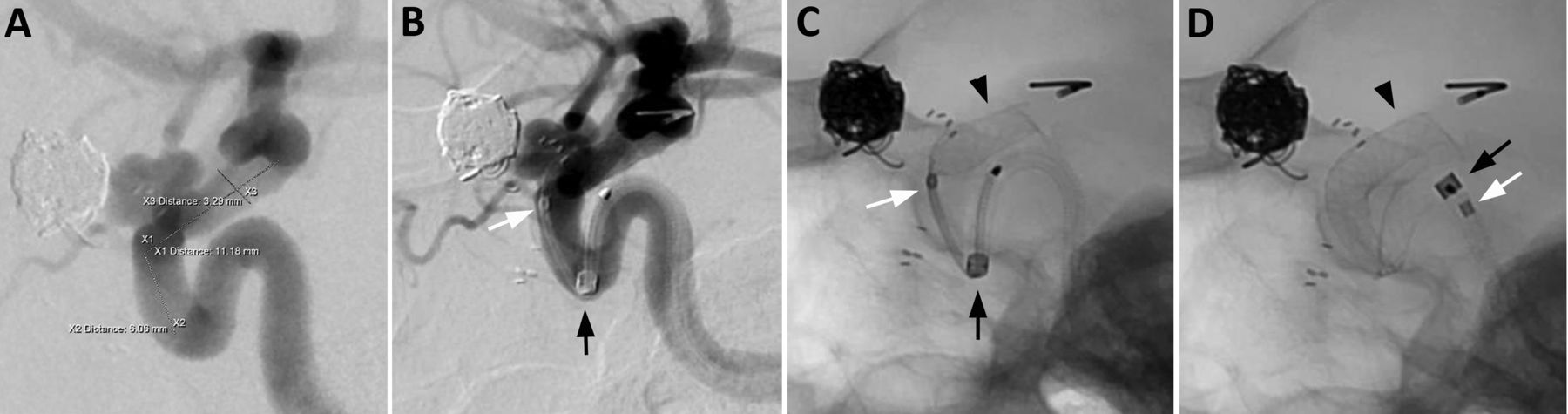
Distal cavernous internal carotid artery (ICA) Navien support during Pipeline embolization of an 8 mm paraophthalmic aneurysm in a 61-year-old patient. (A) Right ICA pre-embolization digital subtraction angiogram (DSA, lateral view) showing the 8 mm paraophthalmic aneurysm. Of note, the patient had a contralateral paraophthalmic aneurysm previously treated by stent-assisted coiling at another hospital. Intra-deployment DSA (B) and single shot fluoroscopy (C), both lateral views, demonstrating the Navien catheter in the distal cavernous ICA with its tip (black arrow) at the anterior genu. The Marksman catheter (tip shown by white arrow) and the partially deployed Pipeline embolization device (PED, black arrowhead) are also visualized. (D) Single shot fluoroscopy (lateral view) post-PED deployment. The Navien was pinch-pulled back during the PED deployment and now its tip (black arrow) is positioned at the posterior genu of the cavernous ICA. The tip of the Marksman (white arrow) is now inside the Navien. The deployed PED is indicated by a black arrowhead.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
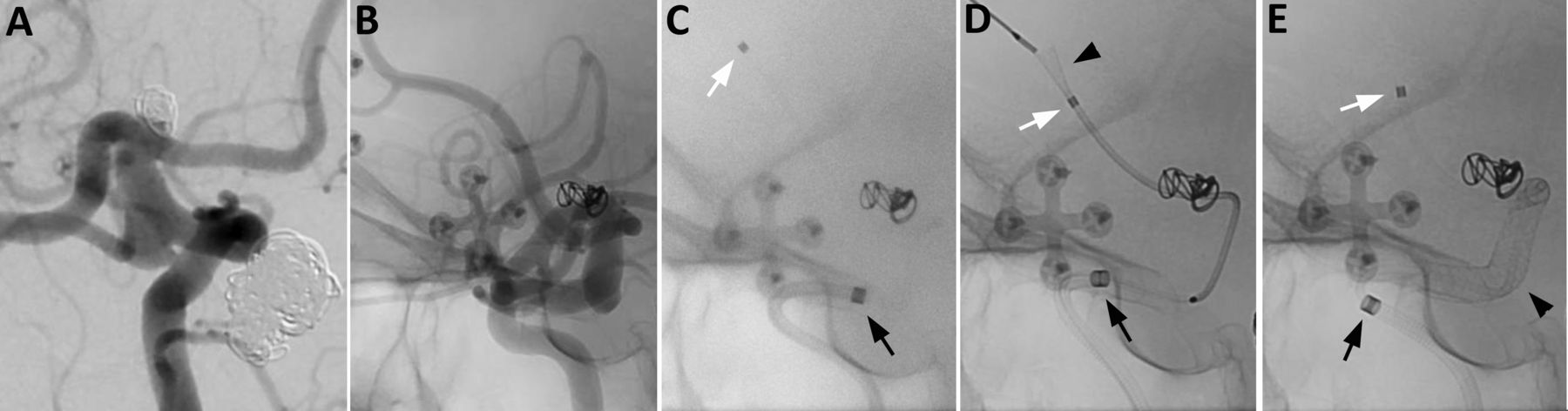
Periclinoidal internal carotid artery (ICA) Navien support during Pipeline embolization of a 2 mm ICA termination aneurysm residual and a 6 mm posterior communicating artery (Pcom) aneurysm in a 52-year-old patient with multiple intracranial aneurysms. (A) Right common carotid pre-embolization digital subtraction angiogram (DSA, oblique view) demonstrating a 6 mm Pcom aneurysm and a previously coiled ICA termination aneurysm with a 2 mm residual (initial treatment at another institution). Of note, the patient had a ruptured basilar apex aneurysm that was previously treated by coil embolization at another institution, and the coil pack is visualized in this image. (B) Pre-embolization right ICA angiography (native fluoroscopy, lateral view). This image is to be used as a reference view for images in C–E. (C–E) Unsubtracted single shots (lateral views) showing the position of the Navien catheter during deployment of the Pipeline embolization device (PED). (C) Prior to advancing the PED, the Navien tip (black arrow) is positioned in the supraclinoid ICA and the Marksman tip (white arrow) is positioned in the right A2 segment. (D) Intra-deployment, the Navien is withdrawn slightly to the clinoidal ICA while the PED (black arrowhead) is opened in the A2 segment. The distal PED was subsequently pulled back to position in the A1 segment (not shown). (E) During PED deployment the Navien (black arrow) is pinch-pulled back to its final position at the anterior genu of the cavernous ICA. The fully deployed PED is indicated by a black arrowhead.
Guide catheter complications
No clinically significant guide catheter-related complications occurred in the 78 cases. In three cases, intra-arterial nicardipine was used for vasospasm. In one case, a 31-year-old woman, vasospam developed during advancement of the Navien catheter into the petrous ICA. This spasm was primarily distal to the tip of the Navien and probably resulted from advancement of the Marksman catheter subsequently used to track the Navien into position. Nicardipine (1 mg total) was administered after the vasospasm developed and this resulted in significant improvement in vessel caliber. The case continued without further incidents. In two additional patients nicardipine was added to the flush bag as prophylaxis against hyperactive vessels. Only one of these patients developed vasospasm despite the prophylaxis. The incidence of significant vasospasm was therefore calculated as 2/78 cases (3%), although no clinical sequelae resulted in either of the two cases. No arterial dissections occurred in any of the cases performed. Furthermore, no vessel wall abnormalities were visualized in the region of the guide catheter during follow-up angiography.
Discussion
In this report we describe our experience using the Navien 5 Fr, 0.058 inch ID distal access catheter in 78 cases of anterior circulation aneurysm treatment by Pipeline embolization. The catheter tip was positioned successfully from the cervical ICA all the way to the M1 segment of the MCA. In 62% of the cases the Navien tip was positioned in the proximal cavernous ICA, and this corresponded to the favored position for treatment of paraophthalmic aneurysms (59% of the aneurysms in the series). In 30% of the cases the Navien tip was positioned in the petrous ICA, and this corresponded to the favored position for treatment of cavernous aneurysms (25% of the aneurysms in the series). Clinical success, defined as successful tracking of the Navien to the intended position, occurred in all 78 cases (100%) despite significant cervical ICA tortuosity in 34 cases (44%). No significant guide catheter complications occurred in the series, including no dissections. Intra-arterial nicardipine was used for vasospasm in three cases (4%); however, it was used as prophylaxis in the guide catheter flush bag in two cases.
Classically, neurointerventions were performed using a biaxial system consisting of a relatively rigid guide catheter (eg, Envoy) positioned in the cervical ICA and a small flexible microcatheter that was advanced intracranially to the target of interest. Often the microcatheter has to be advanced a considerable distance from the supporting guide catheter, thereby reducing the control and tactile feedback for the operator and increasing the propensity for unwanted slack in the system. These limitations are amplified in older patients with significant vessel tortuosity, and it can lead to technical failures that necessitate alternative more invasive approaches such as direct carotid puncture.10
Technological advances in catheter engineering have made significant progress in moving the support system further into the intracranial circulation. This transition has occurred concurrently with the development of novel devices such as the PED which require this robust support for deployment. The newer generation of guide catheters and distal access catheters have more flexible atraumatic distal ends for increased trackability. These catheters get support not from the rigidity of traditional guide catheters but more from the stability that results after the catheter is anchored around multiple bends.5 The Neuron and Outreach DAC are two commonly used current generation catheters, and clinical experience with the Neuron1–5 and the Outreach DAC6–8 have been described.
Park and colleagues1 used the Neuron 6 Fr delivery catheter to facilitate treatment of seven patients with cranial pathology and particularly tortuous anatomy. Six of the cases required intracranial positioning of the guide catheter, three in the vertical petrous segment and three in the vertical cavernous segment. No guide catheter-related complications were reported. Turk and colleagues5 reported a large series of 659 cases in which 529 cases of current generation guide catheters (Neuron and Chaperone) were compared with 130 cases of conventional guide catheters (Shuttle and Envoy). They demonstrated that intracranial carotid purchase was successful in 70–74% of cases with current generation catheters compared with 3.4% of cases using the conventional catheters, and that these results were achieved with similar safety profiles (1.1% guide catheter-related complication events). As with these series, we had significant success achieving intracranial purchase with the Navien catheter. We report 100% success in achieving intracranial positioning and no significant guide catheter-related complications occurred.
Chaudhary and colleagues3 reported the use of the Neuron 6 Fr, 0.053 inch ID catheter for ultradistal access to the cerebral vasculature in 12 cases. They described placement of the Neuron catheter in a variety of impressive distal locations including the M1, A1 and P1 without complications. Once in position, interventions including stenting, coiling, angioplasty and embolizations with liquid embolic agents were performed safely and effectively. In our series, the Navien catheter was also positioned safely in a variety of intracranial locations including ultradistal locations such as the M1 segment. However, in our series the Navien catheter was used for a very different type of procedure (Pipeline embolization) than the interventions reported by Chaudhary and colleagues. In our experience, Pipeline deployment requires considerably more manipulations of the system, and thereby more stresses on the distal catheter, than does coiling, stenting and other neurointerventions. These added stresses are from the multiple pushing and pulling maneuvers (termed ‘wagging the tail’) performed during Pipeline deployment. Despite these added stresses, the Navien catheter performed extremely well and provided the necessary support for the procedures.
Interventional catheters are typically compared based on objective numerical specifications such as the outer diameter (OD) and ID, and also based on more subjective specifications such as flexibility and trackability. The hard specifications of the Neuron, DAC and the newer Navien catheter are compared in table 4. The objective features of the Navien catheter which offer advantages over the other two catheters are the smaller OD and larger ID. The Navien is a true 5 Fr OD along its entire length compared with 5.2 Fr for the DAC and 5 Fr distal/6 Fr proximal for the Neuron. This smaller profile probably contributes to its trackability and allows for improved flush and injections around the catheter, particularly if it is used in a triaxial system. The Navien also has a larger 0.058 inch ID compared with the 0.057 inch ID for the DAC and the 0.053 inch ID for the Neuron. This larger ID helps to accommodate the larger 0.027 inch microcatheters used for flow diverters and also provides additional room for improved flush and contrast injections. In our experience, the smaller OD and larger ID of the Navien, combined with a supple distal end, have led to significant clinical success in a large number of cases. The small OD has facilitated distal and ultradistal atraumatic positioning of the catheter, and the larger ID has the added advantage of being able to perform intraprocedure runs and roadmaps.
5 Fr distal intracranial catheters
The stability of distal access and guide catheters has been attributed to the fact that they anchor themselves around the multiple bends of the intracranial circulation such as the petrous and cavernous segments. This is in contrast to conventional guide catheters that are positioned in the cervical ICA, which achieve stability from the rigidity of the catheter. However, the gentle curves of the cervical ICA in combination with the soft surrounding tissues of the neck are thought to have a negative impact on the stability of these conventional catheters. These catheters commonly back out when devices are being advanced distally, and the back and forth movement of the catheter during a procedure is thought to give rise to vessel trauma and dissections.5 This back and forth movement has not been described with respect to modern distal access catheters. In our experience with the Navien catheter, we commonly visualized movement of the catheter tip during PED deployment, particularly when the Marksman and PED are wagged to facilitate vessel wall apposition of the device. As the PED is deployed and slack is removed from the system, the Navien catheter will commonly migrate forward. If the Navien tip is positioned just proximal to the target aneurysm prior to initiating deployment, the Navien will have to be pinch-pulled back as the PED is deployed to prevent migration of the Navien over the outside of the partially deployed PED. Despite the significant motion of the Navien catheter during these procedures, we experienced no vessel dissections in our series. This motion has been atraumatic and further validates the trackability of the catheter. Furthermore, we attribute the success of the previously described pseudo-corking technique to the added trackability of the Navien.11
Although we have had great success with the Navien catheter for Pipeline procedures, the main limitation of this catheter is its lack of proximal support. This catheter is not well suited to be used alone as a guide catheter for anterior circulation embolizations. It is best used in combination with a triaxial system for these anterior circulation cases so that the Shuttle catheter can provide the necessary proximal support, particularly for Pipeline embolization. Triaxial systems including a distal access catheter are in general more complicated to assemble than biaxial systems, and the risks of using such access systems must be considered for each case, particularly when there is minimal vessel tortuosity. We have successfully used the Navien as a distal guide catheter in a biaxial system for posterior circulation cases. However, the majority of these cases have been performed via brachial approaches.
Conclusions
The Navien distal intracranial catheter is a newer generation distal access catheter and an important component of the support system used for embolization of cerebral aneurysms with the PED. This catheter is highly trackable, atraumatic and, when used in conjunction with a triaxial access system, it provides sufficient support for the significant microcatheter manipulations needed for PED deployments. Furthermore, the OD and ID specifications of the Navien are favorable compared with other current commercially available distal access and guide catheters, resulting in a low profile catheter with improved flushing and contrast injections.
Footnotes
-
Contributors All authors contributed to the design, implementation and writing of this manuscript.
-
Competing interests ALC is a proctor for the Pipeline Embolization Device (Covidien, Mansfield, Massachusetts, USA) and a consultant for Covidien. The other authors have no competing interests.
-
Ethics approval Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.