Article Text

Abstract
Introduction Neurothrombectomy frequency is increasing, and a better understanding of the neurothrombectomy call burden is needed.
Methods Neurointerventional physicians at nine participating stroke centers prospectively recorded time requirements for all neurothrombectomy (NT) consultations over 30 consecutive 24 hour call periods.
Results Data were collected from a total of 270 days of call. 214 NT consultations were reported (mean 0.79 per day), including 130 ‘false positive’ consultations that ultimately did not lead to thrombectomy (mean 0.48 per day). 84 NT procedures were performed at the nine centers (0.32 per day, or 1 every 3 days). Most (59.8%) consultations occurred between 5pm and 7am. 30% of thrombectomy procedures resulted in delays in scheduled cases; treating physicians had to emergently travel to the hospital for 51.2% of these cases. A median of 27 min was spent on each false positive consultation and 171 min on each thrombectomy. Overall, the median physician time spent on NT responsibilities per 24 hour call period was 69 min (mean 85 min; IQR 16–135 min).
Conclusions NT consultations are frequent and often disrupt physician schedules, requiring physicians to commute in from home after hours in the majority of cases. As procedural and consultation volumes increase, it is crucial to understand the significant burden of call on neurointerventional physicians and develop strategies that reduce the potential for burnout. Importantly, this study was performed prior to the completion of the DAWN and DEFUSE3 trials; NT consultations are expected to continue to increase in the future.
- thrombectomy
- stroke
- angiography
- intervention
- statistics
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy for anterior circulation emergent large vessel occlusions (ELVO) has been well established in the literature,1–10 and is now the standard of care for ELVO patients, with position statements in support of more widespread use from both the American Heart Association/American Stroke Association and the Society for Neurointerventional Surgery.11 12 Since 2015, institutions have seen an increase in neurothrombectomy (NT) cases, and practitioners have reported increased aggressiveness in pursuing thrombectomy in ELVO patients.13 14 Recently, the DAWN (Diffusion Weighted Imaging or Computerized Tomography Perfusion Assessment with Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) and DEFUSE 3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trials were published showing functional benefit in patients receiving endovascular revascularization as many as 24 hours after symptom onset if salvageable penumbra is present.15–17 It is likely that these findings will result in an even larger increase in case volume as surgeons adjust their practices to include patients presenting in a delayed manner or with wake up strokes.
A recent retrospective study performed at 10 geographically diverse stroke centers in the USA demonstrated that NT cases often occur outside of regular work hours, most commonly at 8–9pm, with each procedure requiring approximately 2–3 hours of time commitment from contact to procedural finish.14 The nature of neurointerventional (NI) care for ELVO patients is that teams that are appropriately activated will often subsequently decide to not proceed with NT. For the purposes of this study, such activations are termed false positive consultations. False positive consultations and time requirements following the NT procedure were not included in the prior study due to its retrospective design. Therefore, the prior study may have significantly underestimated the total workload of endovascular call for NI physicians. Understanding this workload is important because the burden of NT call may have significant ramifications on physician elective schedules and quality of life.
The aim of the present study was to capture a comprehensive picture of the total time burden of stroke NT call by including false positive consultations and measuring total time required for patient care as a means of more accurately quantifying physician workload.
Methods
Institutional review board approval was obtained at nine participating stroke centers (table 1). NI physicians prospectively recorded time requirements for all thrombectomy consultations over 30 consecutive 24 hour call periods, including both false positive consultations and mechanical thrombectomy procedures. Non-thrombectomy consultations for cerebrovascular conditions other than large vessel occlusion were excluded from the study.
Participating centers
In accordance with HIPAA, de-identified data on each consultation were collected and transmitted to the primary center for analysis. Data collected included: day of the week, start and end times for each consultation, and time of groin puncture and groin closure for thrombectomy consultations. Start time was defined as time of initial contact of the attending NI physician. End time was defined as the time when all NI team patient care requirements were completed. For false positive consultations, end time was defined as the time at which the patient was determined to not be a thrombectomy candidate. For thrombectomy procedures occurring during peak hours, end time was defined as the time when ordersand all family and service provider discussions had been completed. For thrombectomy procedures occurring outside of regular work hours, end time was defined as the time when ordersand all family and service provider discussions had been completed, and the physician arrived back at home. Time for completion of procedural dictations was not included. Additionally, on-call physicians recorded whether the thrombectomy procedure resulted in a delay of 30 min or more to scheduled cases or clinic duties, whether or not an alternate physician was required to cover a given case due to conflicts, and whether or not the physician was required to commute from home. For the purposes of analysis, ‘day time’ was defined as 6am to 9.59pm and ‘night time’ as 10pm to 05.59am, based on typical sleep and wake cycles. ‘Work hours’ were defined as 7am to 4.59pm, Monday through Friday, while ‘non-work hours’ were defined as 5pm to 06.59am, Monday through Friday and all day Saturday and Sunday. Time stratifications were defined based on groin puncture time for thrombectomy cases and based on contact times for false positive consultations. A post hoc analysis was additionally carried out using pooled thrombectomy data from the previously published retrospective data14 to demonstrate the peak times of day that thrombectomies occurred.
Statistical analysis
Statistical analysis was performed using SPSS, V.24.0 for Mac (Armonk, New York, New York, USA: IBM Corp). The Kolomogorov–Smirnov test was used to evaluate for normality of distribution of data; therefore, non-parametric tests were used for analysis when appropriate. The χ2 test of independence, the Mann–Whitney U test, and the Kruskal–Wallis test were used when appropriate. R Studio (Vienna, Austria: R Foundation for Statistical Computing, 2016) was used to generate graphical representation of the data.
Results
Data were prospectively collected from a total of 270 days of call (30 consecutive days at nine institutions) between the months of May to September 2017, based on differing approval times of each unique institutional review board. A total of 214 NT consultations (mean 0.79 per day), including 130 false positive consultations (mean 0.48 per day) and 84 thrombectomy procedures (mean 0.31 per day), were prospectively recorded at the nine centers.
Time requirement
The median total time for initial thrombectomy consultations, from time of contact until completion of all related responsibilities, was 171 min (mean 191 min; IQR 120–221 min). This does not include subsequent care required over the remaining course of the patient’s hospital course, or even follow-up call during that same 24 hour period. The median time from contact to groin puncture was 68 min (mean 92 min; IQR 45–104 min), median procedure length was 46 min (mean 57 min; IQR 29–76 min), and median amount of time from groin closure to end time (completion of all initial responsibilities) was 35 min (mean 43 min; IQR 19–60). These times did not vary significantly by day versus night, work versus non-work hours, or weekdays versus weekends, except for time from groin closure to end of consult, which was significantly shorter during day time (32 mins vs 51 mins; P=0.029). The median amount of time for consultations that did not proceed to thrombectomy was 27 min (mean 56 min; IQR 13–78 min). The median overall time burden per 24 hour call period was 69 min (mean 85 min; IQR 16–135 min).
Procedure frequency
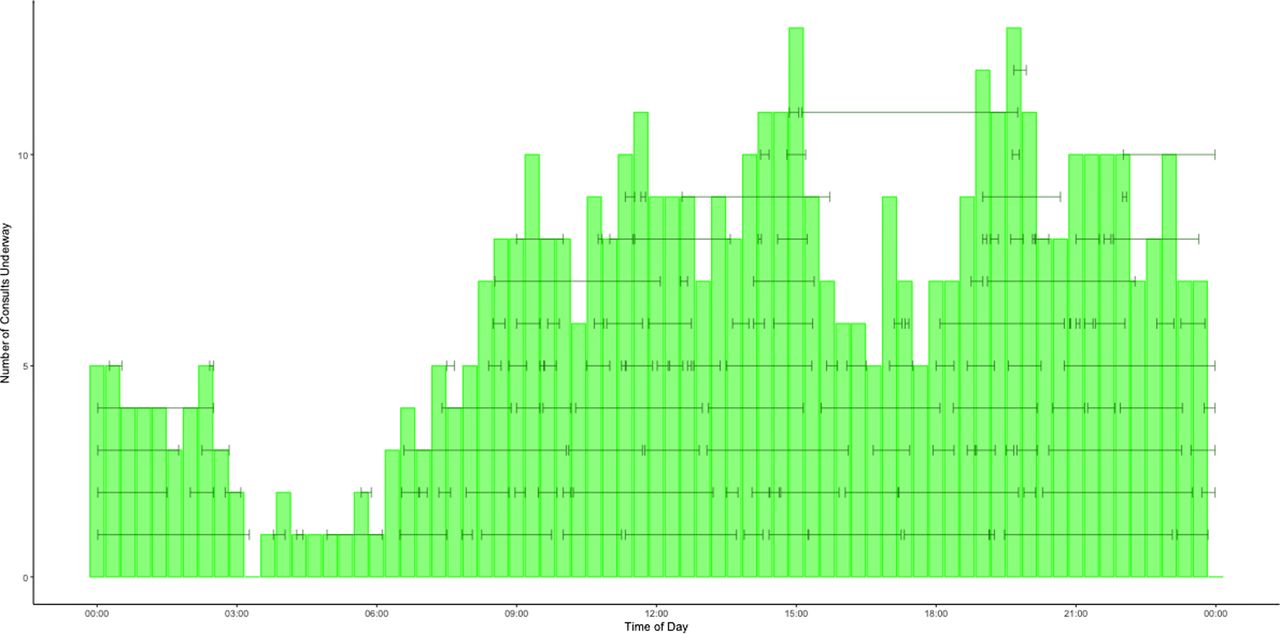
Table 2 reports the number of consultations occurring based on day of the week and time of day. Thrombectomy frequency was bimodal, occurring most commonly between 3–5pm and 9–10pm (figure 1). The most common times for false positive consultations was also bimodal, at 3pm and 7.30pm (figure 2). Including all NT related responsibilities, the most common time was 2pm, with the majority of time burden occurring between the hours of 9am and 10pm (figure 3).
Consultations based on time of day and day of the week

Thrombectomy procedure times organized by time of day. Horizontal bars represent time from contact until all responsibilities have been completed.

False positive consultation times organized by time of day. Horizontal bars represent length of time of consult.

Total neurothrombectomy time expenditure organized by time of day. Horizontal bars represent length of time per consult and/or procedural consult.
Delays and commute
For consultations requiring thrombectomy, a delay in scheduled cases or clinic schedules was reported in 25 cases (29.8%); this represented 71.4% of cases performed during work hours. An alternative operator was required to cover eight cases (9.5%). The physician was required to commute from outside of the hospital during non-peak hours for 43 of the 84 procedures (51.2%).
Thrombectomy incidence: retrospective versus prospective
Eight centers participated in both a previously published manuscript14 (retrospective data from a 92 day period, including June 1–August 31, 2016) and in this prospectively collected study (30 days of data from May–September 2017). A comparison of thrombectomy incidence between studies is shown at each of these eight centers in table 3. The rate of thrombectomy was approximately 1 every 3 days in the present study compared with approximately 1 every 5 days in the prior study from 2016. Seven of the eight centers (88%) had a higher rate of thrombectomy in the present study compared with the study performed in 2016.
Thrombectomy incidence from the retrospective study14 (2016) compared with the present study (2017) for all eight centers that participated in both studies
Thrombectomy timing: retrospective and prospective pooled data
Time of groin puncture and groin closure from 189 thrombectomy procedures from the previously published retrospective data was pooled with time of groin puncture to closure for the 84 thrombectomy procedures from this prospective study. Overall, 273 procedural times were combined. The distribution of procedural times based on time of day for these 273 procedures is shown in figure 4. Most common procedural times were from 11am to 9pm, with the highest incidence at 3–4pm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled time of day for 273 thrombectomy procedures from the retrospective study (189 procedures) and the present prospective study (84 procedures). Horizontal bars represent length of time for thrombectomy (puncture to closure).
Discussion
This prospective study of NT call among NI physicians at nine geographically diverse stroke centers indicates that, on average, NI physicians are spending approximately 69 min per 24 hour call on thrombectomy related responsibilities. Consultations and thrombectomy procedures are frequent and more commonly occur during non-work hours. In over half of the cases, physicians must emergently commute from outside of the hospital to perform the procedure. While most procedures occur after hours, those that do occur during work hours usually result in delays in elective clinic or procedural schedules of at least 30 min (71% of procedures).
Importantly, a comparison of NT procedural incidence from 2016 versus 2017 across the eight centers that participated in both studies shows a marked increase in procedural volume across that time. Studies of the potential number of total NT patients would suggest that this trend will continue well beyond this study.18 19 In the previously published retrospective study which evaluated procedures performed between June and August 2016, thrombectomy procedures occurred, on average, every fifth day. These prospective data now indicate that thrombectomy procedures are occurring, on average, every third day. The recently published DAWN trial results, showing the overwhelming benefit of thrombectomy in appropriately selected patients presenting with strokes between 6 and 24 hours from onset (including wake up strokes), are likely to lead to further procedural volume growth.16
At most stroke centers, including those in this study, thrombectomy call is continuously covered by a small number of physicians (table 1). Most of these physicians have elective clinical and procedural schedules outside of thrombectomy call, including busy neurosurgical, neurology, or radiology practices. This study suggests that the physician time commitment for thrombectomy call, both in terms of total quantity but also the non-work hour responsibilities, is burdensome and disruptive. For instance, 60% of all consultations and 60% of thrombectomies occurred during non-work hours, with 15% and 18% (respectively) occurring during night time (sleeping) hours. Beyond the medical and health system considerations, this has implications for providers’ personal and family lives. Additionally, almost a third of thrombectomy cases caused a delay in scheduled cases, which further dramatically impacts time at work, often with compounding delays occurring as resource limitations (eg, anesthesia availability for the delayed elective case) result in further delays beyond the added minutes from the stroke cases itself. These downstream added delays can be quite substantial. Furthermore, data suggest procedural volumes have increased over the past few years and may continue to increase as the thrombectomy eligible patient population expands. In concert with the emergent, high risk nature of thrombectomy procedures and the clinical severity of ELVO, the effect of progressively increasing consultation and procedural volumes on NI physician well being is considerable. There have yet to be any rigorous studies reporting on either NI physician compensation for NT call or physician burnout associated with NT call, but clearly these topics are of increasing importance as NT volumes increase across the world.
A study in 2013 investigated the consequences of increasing percutaneous coronary intervention (PCI) rates in patients with myocardial infarctions, in the setting of decreasing reimbursement rates for interventional cardiologists based on Medicare Severity Diagnosis Related Groups billing practices.20 Despite the fact that PCI was determined to be more cost effective with similar costs to Medicare, the average decrease in reimbursement for the entire family of PCI codes was about 18%, largely due to a diminution in procedure time from 2008 to 2012. The paper concluded that this lack of appropriate reimbursement was ‘catastrophic’ to medical professionals and their staff: 31% of interventional cardiologists surveyed planned to reduce or stop taking PCI call, and 65% reported reductions in staffing or services in their own or colleagues' practices. It is crucial that we avoid a similar scenario in NI practice; compensation for NI call should appropriately reflect the time burden.
There are important limitations to this study. Call responsibilities that were not related to ELVO patients were not included in this study. We sought to capture the total time that physicians are engaged in NT patient care, which included data from time of contact regarding ELVO patients at alternate sites that were being transferred for NT. While transfer times may overestimate the physician call time responsibility, these patients do require manipulation of upcoming schedules and place limits on what physicians may do while on call. This is a study of physician time, but clearly NI care occurs as part of a team, and the call burden for operating room staff, fellows, technologists, and others directly involved in ELVO treatment is not captured directly by these data. Along similar lines, subsequent resource associated delays that occur in the 30% of cases when elective patients are delayed were not captured, further underestimating the total burden. Additionally, while the participating centers are geographically diverse, there are other models of NI care that might not be captured in this sample and the volumes of consults and cases at the participating centers may not be representative of the volumes at the majority of interventional stroke centers. Importantly, this study took place prior to the results of the DAWN and DEFUSE3 trials, which are expected to further increase the number of NT consultations.16 17
Conclusions
The burden of NT call on NI physicians is significant and disruptive. The median amount of time required for NT responsibilities per 24 hour neurovascular call is 69 min with most consultations occurring outside regular work hours. This study suggests that NT procedural incidence has increased from 1 procedure every 5 days in 2016 to 1 every 3 days in 2017. As procedural and consultation volumes increase, it is important that we understand the burden of call on NI physicians and develop strategies to reduce the risk of physician burnout, compensate providers appropriately, and optimize our triage and selection paradigms.
References
Footnotes
Contributors Conception and design: KMF. Data collection and interpretation: all authors. Statistical analysis: TAW. Drafting the article: MMW, TAW, and KMF. Critical revision of the article: all authors. Final approval of the article: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Ethics approval Institutional review board approval wasobtained at the nine participating stroke centers.
Provenance and peer review Not commissioned; externally peer reviewed.