Article Text

Abstract
Purpose To report percutaneous transcranial puncture, embolization and occlusion of a very symptomatic hypoglossal canal/anterior condylar vein dural arteriovenous fistula (DAVF) using syngo iGuide navigational software in a patient in whom transarterial and transvenous embolization and surgery had failed.
Methods After unsuccessful arterial and venous embolization and surgical treatment of a symptomatic hypoglossal canal DAVF, a 47-year-old man was transferred for further management. With exquisite anatomic detail provided by C-arm cone-beam computed tomography (CBCT) equipment (Artis zee Biplane, Dyna CT VC21H, Siemens Healthcare GmbH, Germany) and syngo iGuide needle guidance navigational software (Siemens Healthcare GmbHy) for planning a safe direct approach, the hypoglossal/anterior condylar vein, the dominant outflow vein of the fistula, was needle punctured percutaneously at the hypoglossal foramen and occluded with ethylene vinyl alcohol copolymer liquid embolic agent (Onyx, Medtronic, Minneapolis, Minnesota, USA) after placing two anchoring platinum coils (Target detachable coils, Stryker Neurovascular, Fremont, California, USA).
Results After a year of progressively severe left eye proptosis, chemosis and increased intraocular pressure, the symptoms quickly subsided after this embolization and the patient was symptom free at his 3-month and later checkups.
Conclusion With guidance and imaging provided by CBCT and syngo iGuide navigational software, an otherwise untreatable DAVF was successfully embolized and obliterated by an aggressive unique percutaneous trans-cranial needle puncture of the dominant outflow vein in the hypoglossal canal.
- arteriovenous malformation
- posterior fossa
- CT angiography
- angiography
- fistula
Statistics from Altmetric.com
Background
The abnormal arteriovenous connections within the dura mater of dural arteriovenous fistulas (DAVFs) usually drain into a specific dural sinus or an adjacent cortical vein. The clinical presentation, management strategy and clinical outcome depend on the location and accessibility of the DAVF. The standard approach for management of DAVFs is transvenous and/or transarterial embolization. Surgery is usually reserved for residual fistulous communications.1 The posterior fossa DAVF in our case falls into the subset of DAVFs with involvement of the anterior condylar/hypoglossal vein (ACV).2–13 Because embolization and surgery in this patient had failed, a combination of 3D digital subtraction arteriography (DSA), C-arm cone-beam computed tomography (CBCT) and syngo iGuide navigational software was used to formulate a unique treatment plan and approach for direct percutaneous needle puncture via the hypoglossal foramen of an otherwise untreatable DAVF.
Case presentation
A 47-year-old man presented at an outside hospital with left eye chemosis and minimal proptosis that had gradually worsened over a year. Physical and neurological exam were normal except for chemosis and orbital and periorbital edema. Elevation of the intraocular pressure was documented on the ophthalmological exam and MRI revealed a dilated left cavernous sinus and multiple serpentine vessels in the left temporal fossa with large flow voids in the left prepontine region. Cerebral arteriography demonstrated a type IV Cognard classification14 15 base of the skull DAVF with posterior fossa cortical venous drainage into the basal vein of Rosenthal (figure 1). The left internal jugular vein was accessed for possible embolization of the DAVF via venous connections with the jugular vein and bulb. There were no connecting veins. Then arterial embolization with liquid embolic agent was attempted via the transmastoid branch of the left occipital artery. This produced no benefit. Three days later, still in the outside hospital, the patient underwent a craniotomy to close the fistula. A postoperative angiogram showed that the DAVF was patent with early venous drainage to the condylar venous pouch and retrograde filling of the inferior petrosal and cavernous sinuses and deep temporal veins.
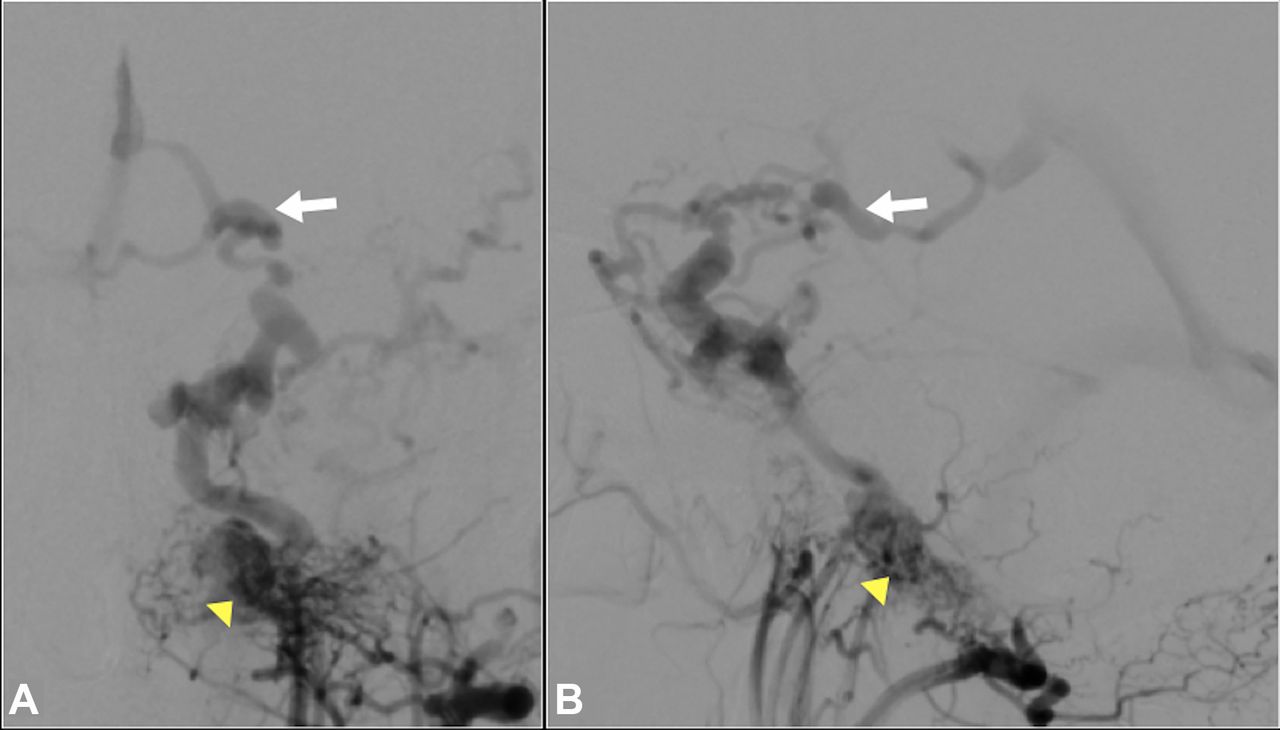
Left external carotid cerebral arteriogram: AP (A) and lateral(B): DAVF of the hypoglossal canal (arrowhead) draining into the inferior petrosal sinus with cortical venous drainage into the posterior aspect of the left basal vein of Rosenthal. (arrow).
After three failed treatment attempts and several days following craniotomy, the patient was transferred to our tertiary care neuro-interventional hospital for management of the DAVF of the left ACV. On arrival at the hospital, it was evident that the patient was confused and disoriented as to place and time. An emergency CT scan of the head showed a left temporal intraparenchymal hematoma. He underwent surgery for left fronto-parietal craniectomy and drainage of the hematoma.
Pre-procedural imaging and diagnostic neuroangiography
The following day, after obtaining informed consent from the patient’s next of kin, subselective cerebral arteriography was carried out in the Neuro-interventional suite (Artis zee Biplane, VC21H, Siemens Healthcare GmbH, Germany). Selective and sub-selective arteriography was performed with biplane 2D DSA. 3D DSA and intra-procedural CBCT imaging were also performed (20 s DR-Head protocol, syngo DynaCT, Siemens).
The exact position of the arteriovenous shunting was pinpointed in the left hypoglossal canal (ACV) with drainage into the left inferior petrosal sinus (IPS) and retrograde cortical venous drainage into the posterior fossa venous system. The DAVF was supplied mainly by the hypoglossal artery from the the neuromeningeal trunk of the ascending pharyngeal artery bilaterally, the meningohypophyseal branch of the internal carotid artery bilaterally, and both vertebral arteries via theC3 anastomotic branch with opacification of the left transverse and sigmoid sinuses and the left jugular vein from the right vertebral artery injection. The major venous drainage was via the left ACV into the IPS, the cavernous sinus, and the posterior portion of the basal vein of Rosenthal, with retrograde flow into the posterior fossa venous system. There was evidence of surgery at the skull base in the region of the left hypoglossal foramen. The left temporal and posterior fossa vessels showed severe venous hypertension with irregularity of the veins and multiple venous aneurysms, findings that were best visualized on three-dimensional rotational views and CBCT images. The exact location of the fistula in the left hypoglossal canal with the ACV draining into the left IPS was clearly seen with the left external carotid injections (figure 1). Compared with the original arteriograms, it was evident that there had been interval thrombosis of the basal vein of Rosenthal, likely the cause of the hemorrhagic venous infarct and hematoma in the left temporal lobe. Opaque embolic material was identifiable in several arterial branches but none in the veins. The relationship of the bony structures and the fistula was best seen on 3D rotational angiography views and CBCT images (figure 2). Based on the 2D and 3D imaging findings and prior unsuccessful endovascular and surgical treatment, it was decided that the best chance for cure of the DAVF was to occlude the ACV by percutaneous direct access at the left hypoglossal foramen.

Cone-Beam CT axial and coronal images with diluted contrast at the level of the left hypoglossal foramen (HF). (A), (B): Exact location of the fistula at the level of the left HF (arrow). Previous Onyx embolization material visible in vessels near the fistula.
3D planning and direct access under intraprocedural CBCT guidance
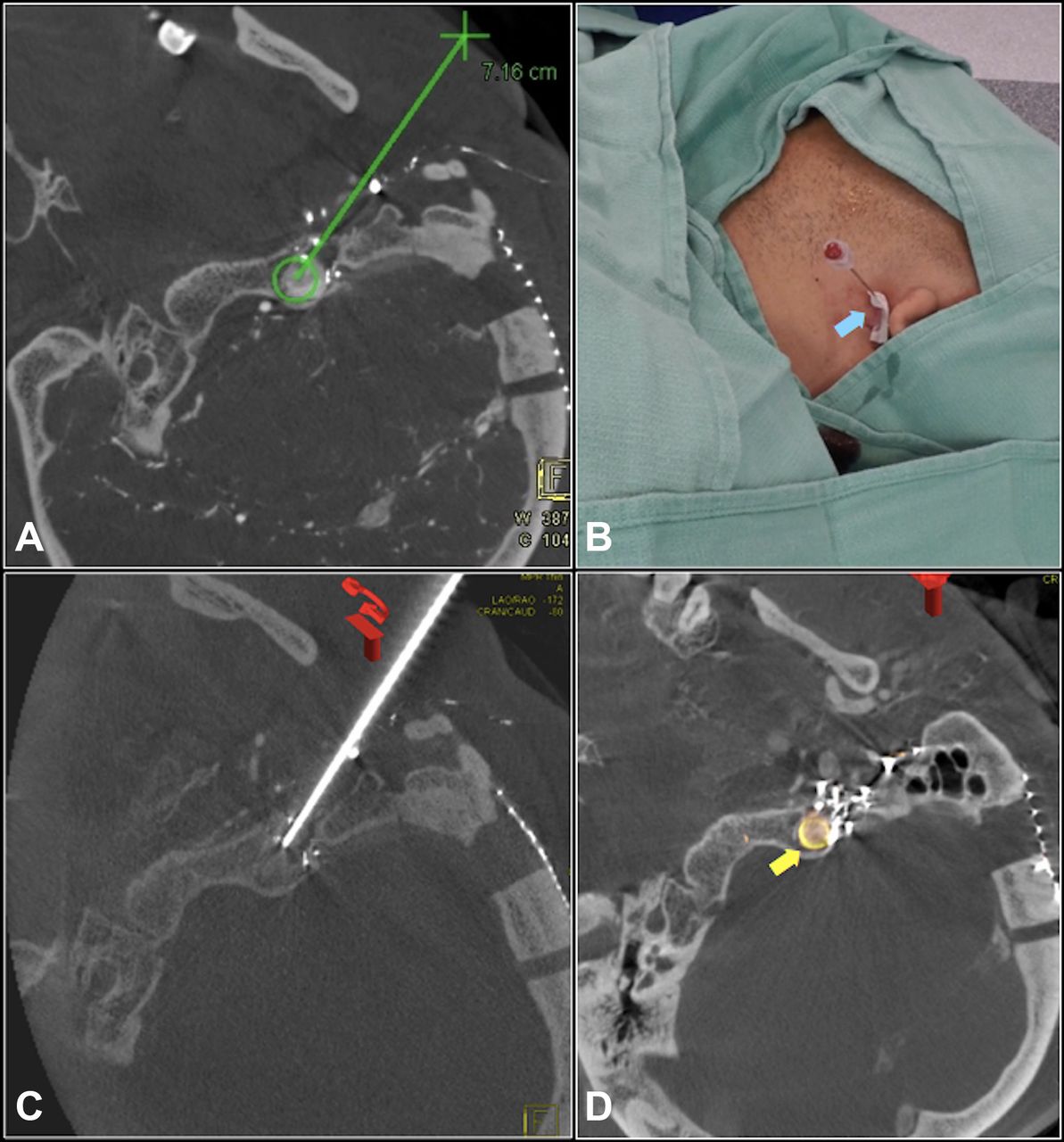
After careful review of the CBCT images in multiplanar and volume rendered reconstruction formats, an ‘ideal’ virtual needle path was planned using commercially available software (syngo iGuide needle guidance, Siemens) in the 3D workstation (syngo X-workplace, VB21, Siemens). Based on the 3D DSA imaging, the patient’s head was rotated to the right and taped in the position that allowed the safest path for direct needle access. CBCT images with carotid and vertebral artery injections were obtained. The CBCT images in multi-planar and volume rendered reconstruction formats were reviewed and the virtual needle path and trajectory were optimized to avoid ascending pharyngeal artery branches of the left external carotid, the left internal carotid and left vertebral arteries, and to pass anterior and to the left of the stylo-mastoid process, thereby avoiding Onyx casts from prior embolization. The length of the virtually planned needle path was measured at 7.16 cm. To precisely control the depth of needle advancement, a 7 cm stop was placed on the 15 cm 20 ga. needle. C-arm views that corresponded to en face ‘bull’s-eye’ and needle progression views were selected using the 3D syngo iGuide planning software (figure 3a). The C-arm was automatically driven to the optimal angle for the en face ‘bull’s-eye’ view of the needle path. The virtual needle path was overlaid on 2D fluoroscopy in the frontal plane and was automatically tracked with changes in C-arm angulation, table position and image zoom. The needle was advanced in en face ‘bull’s eye’ view projection through the planned virtual path with fluoroscopy, 3D image overlay and CBCT images to confirm the exact positioning of the needle tip at the anterior margin of the hypoglossal foramen at 7 cm. Additional advancement of the needle (figure 3c) about 3 mm produced active back bleeding (figure 3b) through the needle. Safe position of the needle tip inside the DAVF was confirmed with contrast injection and biplane imaging.

Axial reconstructions of intraprocedural CBCT images with 3D planning of virtual needle path. (A): syngo iGuide Needle Guidance planning image: the virtual trajectory of the needle. (B). Needle in the left side of the neck advanced under fluoroscopy using Needle Guidance software. Blood (Arrow) dripping from needle. Tip is in hypoglossal foramen. {See (C).} (C): Confirmation of needle position in left HF using CBCT. (D): Post embolization coil and liquid embolic (Onyx) cast in the hypoglossal canal (arrow).
Embolization of hypoglossal AVF after direct access
After stabilizing the needle, a Headway Duo Microcatheter (Microvention, Tustin, California, USA) was advanced into the ACV. Embolization with two platinum coils (Target) to act as an endo-skeleton to stabilize and anchor the non-adherent liquid embolic agent EVOH (Onyx) was performed under 2D biplane roadmapping. Under fluoroscopic control, Onyx 34 was injected and produced complete occlusion of the DAVF (figure 3D). Post-embolization CBCT imaging demonstrated the coils and the liquid embolic cast confined to the left hypoglossal canal. These images were co-registered with the planning CBCT images to correlate and confirm the location of the coils and the Onyx cast relative to the DAVF (figure 4A,B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
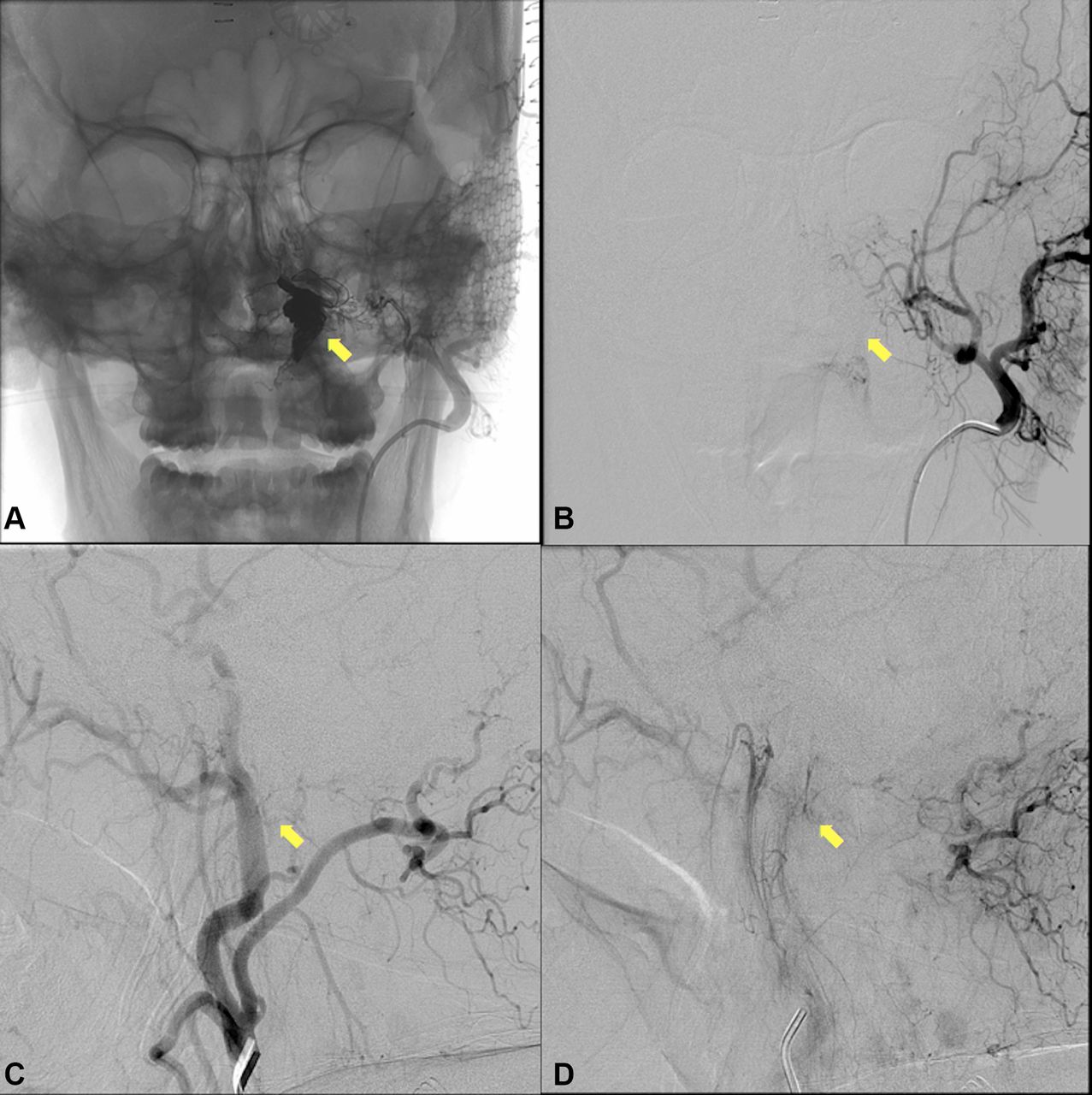
Left external carotid artery (LECA) injection. Post coil and Onyx embolization. (A): AP projection: the Onyx cast in the hypoglossal canal.(Arrow). (B). DSA image of (a). (C),(D): Early and late arterial phase of LECA arteriogram: Complete occlusion of the fistula.
Post-embolization arteriograms (left internal and external carotid arteries, right external carotid and both vertebral arteries) showed complete occlusion of the DAVF with no evidence of distal branch occlusions (figure 4C,D). There were no complications.
Outcome and follow-up
The patient was neurologically intact postoperatively and at 3-month and later follow-ups. The left eye symptoms resolved completely.
Discussion
Most dural arteriovenous fistulas are considered acquired lesions, although the exact aetiology in most is indeterminate. DAVFs account for 10–15% of intracranial vascular malformations and 35% of those occur in the posterior fossa.1 They are seen most commonly in men in their 50s. The clinical manifestations are variable and depend on the site and the drainage pattern. Ernst in 1999 reported three cases of DAVFs that involved the ACV.5 There have been reports of DAVFs involving the marginal sinus, the IPS and the hypoglossal canal, called by some the anterior condylar canal. This complex confluence of veins around the foramen magnum and skull base was called the petrosal confluence by Katsuta et al 7 in 1997 and then the term anterior condylar confluence (ACC) was introduced by San Millan Ruiz et al 8 in 2002. The treatment considered most favorable is embolization with liquid media, with or without coils, and with Onyx (EVOH copolymer) as the preferred embolic agent.16–20 N-butyl cyanoacrylate (n-BCA ‘glue’) is the liquid agent less favoured.19 20 The route most commonly used is transvenous via the internal jugular vein. Transarterial embolization is the second choice with surgery as the third choice and is usually reserved for lesions not amenable to or incompletely treated by embolization. The DAVFs in this area share a blood supply with cranial nerves. (Cranial nerves 9, 10, 11 and 12 receive a blood supply from the neuromeningeal trunk of the ascending pharyngeal artery; the seventh nerve receives a supply from the petrosal branch of the middle meningeal artery and the stylomastoid branch of the occipital artery.) Overly aggressive embolization therapy can result in cranial nerve damage. Surgical morbidity has been reported to be as high as 13.3–16.7%.3 The angioarchitecture of any lesion may dictate the use of any combination of the three forms of therapy.
Our male patient was 46 years of age at the onset of symptoms, primarily ocular and periorbital with proptosis, chemosis and increased intraocular pressure, features most commonly seen with cavernous sinus DAVFs. Originally seen and treated at an outside institution with attempted transvenous and transarterial embolization and craniotomy (although the exact site of the fistula had not been identified), the patient’s symptoms were unimproved. On arrival at our institution, the patient was confused and disoriented.
An emergency CT scan showed an intraparenchymal hematoma in the left temporal region (probably related to spontaneous thrombosis of the vein of Rosenthal) necessitating emergency surgery. On the day following surgical evacuation of the hematoma, he was transferred to the Neuroradiology suite for endovascular treatment. Reports from the outside hospital indicated that there was no communication between the jugular vein and the DAVF. Selective and subselective arteriography with CBCT imaging precisely identified the fistula in the hypoglossal canal with drainage by the ACV into the IPS and retrograde cortical venous flow into the posterior fossa venous system.
Because both transarterial embolization with Onyx and craniotomy had been fruitless, a unique form of treatment was conceived: using syngo iGuide navigational software to perform a percutaneous transcranial needle puncture and catheterization of the ACV within the hypoglossal canal. Occlusion was achieved with Onyx after placement of two coils to anchor the non-adhesive liquid embolic Onyx. This proved to be completely successful and the patient was symptom free in a few days and at his 3-month and later checkups.
To our knowledge, this is the first report of a DAVF treated by a percutaneous trans-cranial approach. This would not have been possible without extensive 3D planning using CBCT imaging and the syngo iGuide needle guidance software. Complete fistula closure and total relief of symptoms were achieved. Teng21 and White22 reported similar success using a percutaneous transorbital needle puncture of the cavernous sinus via the superior orbital fissure for embolization of cavernous sinus fistulas. Houdart23 reported performing surgical craniectomies in 10 patients before transferring the patients to the angiography room for direct sinus puncture and embolization with coils, glue or both. The sinuses punctured and embolized were the transverse sinus in five patients, the superior sagittal in four patients and the superior petrosal in one patient.
As shown in our case, the advances in intraprocedural 3D imaging, 3D planning, sophisticated fluoroscopic needle guidance software and the ancillary tools (catheters, guidewires, embolic agents etc.) have enabled a new approach for the management of DAVFs. CBCT is used during all our neurointerventional procedures and has proved to be a critically important component in maximizing quality results. The syngo iGuide navigational software is invaluable but has been needed in only a few patients. Historically, emphasis has been on the ACC, a major extracranial venous crossroads medial to the jugular vein and adjacent to the hypoglossal canal. Management reports are usually labelled as DAVF of the major draining sinus such as DAVF of the inferior petrosal sinus, the marginal sinus, the hypoglossal canal, the ACV, the jugular foramen, etc. Katsuta7 used the term petrosal ‘confluence’ in 1997. San Millan Ruiz8 introduced the term anterior condylar confluence in 2002. Miyachi9 and Abiko10 in 2008 and Hsu11 in 2014 emphasized the sensible use of the term ‘anterior condylar confluence’ (ACC) fistulas in describing this group of posterior fossa fistulas. Takemoto16 in 2013 suggested that ‘terminology has been almost harmonized’. In so many of those cases, the exact site of the fistula could not be identified. In our case, after exact localization of the fistula, an otherwise untreatable DAVF was occluded by embolization with access provided by direct percutaneous needle puncture of the dominant outflow vein in the hypoglossal canal, a technique never used before. Emphasizing the ACC as a group title may be an oversimplification in light of the technical advances in CBCT imaging equipment and software that now permit precise localization of the fistula site for precise management.
As was true in our case, Miller1 points out that ‘in contradistinction to cerebral arteriovenous malformations, obliteration of DAVFs may be accomplished by occlusion of the fistula’s draining vein(s)'. In patients with DAVFs with multiple arterial feeders and multiple draining veins, CBCT provides an excellent tool for identifying the exact site of the fistula as well as an access route to a dominant outflow vein for embolization. Arteriography with CBCT and navigation guidance software may simplify the treatment procedure and offer improved outcomes.23–27
The critical importance of the superior imaging provided by integrated 3D CBCT with fluoroscopic guidance and the guidance software cannot be overstated. 3D imaging and navigational tools will evolve and improve, and it is vital that the interventional team remain up to date and familiar with the improvements in order to safely perform such complex interventions.
Conclusion
In a patient with suitable anatomy, an otherwise untreatable intracranial DAVF was safely embolized and obliterated. The patient was cured by an aggressive unique percutaneous trans-cranial needle puncture approach of the dominant outflow vein in the hypoglossal canal. Extensive 3D planning using imaging provided by CBCT and sophisticated needle guidance software was crucial to the safety and success of this unique approach for successful occlusion of a complex dural AV fistula.
References
Footnotes
Contributors All authors have made a substantial direct and intellectual contribution to the work. OD was involved in procedural planning and performance, contributed to manuscript conception, design, creation, editing, and revision. MT was involved in the neurointerventional procedure and contributed to manuscript conception and design. JR was involved in manuscript creation, design, editing, and revision. GB and RK were involved in the neurointerventional procedure, study design and manuscript preparation. GL was involved in manuscript preparation and revision. PC was involved in pre-procedural 3D planning and intra-procedural guidance with cone beam CT imaging and software.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PC: full-time paid research scientist, Siemens Medical Solutions USA Inc., Hoffman Estates, Illinois, USA. All other authors: none declared.
Patient consent Obtained.
Ethics approval The study was approved by the Institutional Review Board of the Houston Methodist Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.