Article Text

Abstract
Objective To assess the clinical safety and efficacy of the Atlas microstent in stent-assisted coil embolization of wide-necked intracranial aneurysms.
Methods Single-center observational study in 36 patients (24 female, 12 male, mean age 56 years) with 37 aneurysms for the endovascular treatment of wide-necked aneurysms. After giving informed consent, patients were included according to the following criteria: aneurysm dome-to-neck ratio <2 or neck diameter >4 mm, and a parent vessel diameter of ≤4.5 mm. Primary endpoint for clinical safety was absence of death, absence of major or minor stroke, and absence of transient ischemic attack. Primary endpoint for treatment efficacy was complete angiographic occlusion according to the Raymond-Roy occlusion classification (RROC) immediately after the procedure.
Results In 36/37 (97%) cases, the primary endpoint of safety was reached, one patient had a transitory ischemic attack which completely resolved until discharge. In 31/37 (84%) cases, complete occlusion (RROC 1) was reached, and in 6/36 (17%), a residual neck remained (RROC 2). A sequential approach (first stent, then coiling through the same catheter) was used in 21 cases; the other 16 were treated with the jailing technique. Deployment was technically successful in all cases. Follow-up at a median of 6.1 months was available for 29/37 (78%) aneurysms and showed complete occlusion in 27/29 aneurysms (93%) and a neck remnant in 2 cases (7%).
Conclusion Deployment of the Neuroform Atlas microstent is a safe and effective method for the treatment of intracranial wide-necked aneurysms.
- aneurysm
- angiography
- stent
- coil
Statistics from Altmetric.com
Introduction
Endovascular treatment has become the preferred treatment in most ruptured, but also unruptured, cerebral aneurysms.1–3 Nowadays, a variety of interventional techniques, such as basic coiling, stent- or balloon-assisted coiling, intrasaccular flow disruption, or flow diversion of the parent vessel, are available. The treatment of more complex aneurysms, however, has remained a challenge for neurointerventionalists. This is especially true for wide-necked aneurysms, in which coil prolapse into the parent vessel is a concern to be met by supportive interventional techniques. The first technique introduced to facilitate treatment of these aneurysms was balloon-assisted coiling as it keeps the coils inside the aneurysm sac until the coil basket is stable.4 However, frequently the dome-to-neck ratio is too low to retain the coils. In these cases, the preferred technique is stent-assisted coiling, which has been shown to be as safe as balloon-assisted coiling with a higher long-term occlusion rate.5 In the past 10 years, several new laser-cut or braided stents have been introduced such as the Solitaire, Neuroform, Enterprise, Leo and Leo baby, Low Profile Visualized Intraluminal Support (LVIS) and LVIS Jr, or the Acclino stent.
The Neuroform Atlas (Stryker Neurovascular, Fremont, USA) stent is a successor to the Neuroform stent as the first approved stent for aneurysm treatment. It is intended for the treatment of aneurysms on small parent vessels ranging from 2 to 4.5 mm. It gained its CE mark in May 2015. Similar to other microstents (Leo Baby, LVIS Jr, and Acclino flex), it can be delivered through standard coiling catheters down to an inner diameter of 0.0165 inches
We report our initial experiences with the Atlas stent and evaluate safety, technical feasibility, and effectiveness in this multicenter registry of consecutive patients.
Materials and methods
Patient population
Between April 2016 and April 2017, the Neuroform Atlas device was used to treat 37 aneurysms in 36 patients at the three participating institutions. The treating neurointerventionalist decided to use the Neuroform Atlas device based on clinical and angiographic presentation of the aneurysm. Patient data were analysed retrospectively with approval of our local ethics committee. An independent review of all interventions was performed by three experienced interventional neuroradiologists.
The Neuroform Atlas stent system
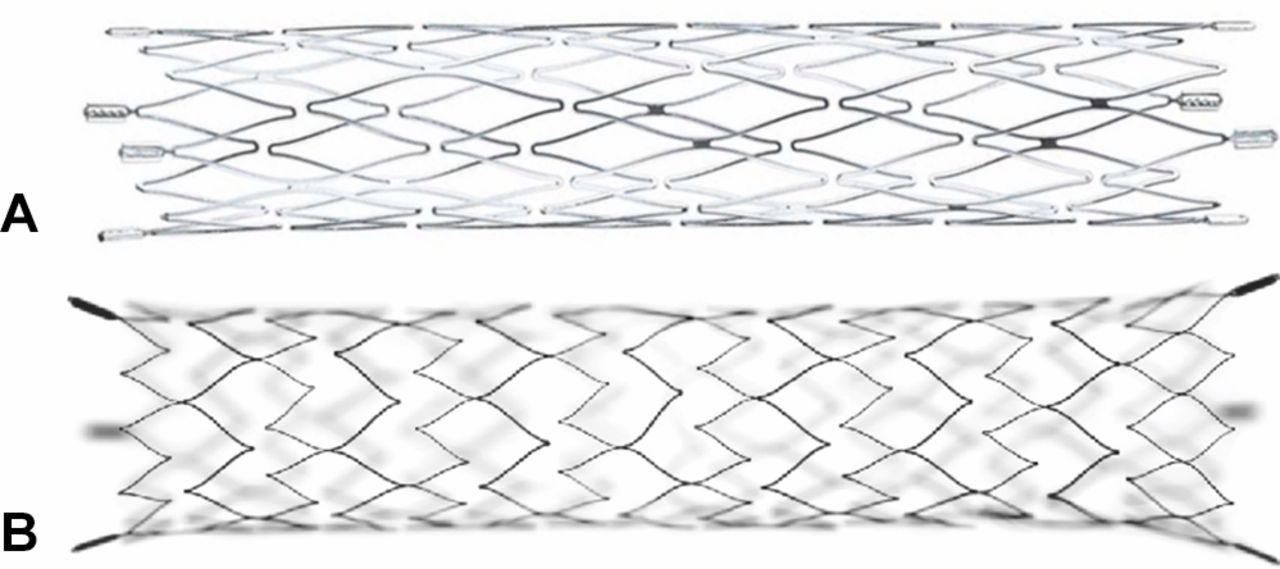
The Neuroform Atlas is a self-expanding nitinol stent with a mixed open-cell/closed-cell design. The stent can be delivered via a 0.0165 in or a 0.017 in microcatheter. The cell size of the Neuroform Atlas stent has been reduced in comparison with that of its predecessor, the neuroform stent, to achieve better coil retention in the aneurysms. Images of both stents are provided in figure 1. The Neuroform Atlas stent has three radiopaque markers at each end. It can be used either with the jailing technique or be reprobed after placement. Available diameters range from 3 mm to 4.5 mm and can be placed in vessels ranging from 2 to 4.5 mm. Available stent lengths are 15, 21, 24, and 30 mm. With stent release only little or no foreshortening occurs improving the accuracy of stent placement. The mix of open and closed cell in the stent design is supposed to improve stability within the vessel via the closed cells at the proximal end while providing high flexibility, even in tortuous vessels through the open cells in the middle. Owing to the mostly open-cell design, resheathing of the stent is not possible.

(A) The Neuroform EZ stent with its uniform diamond-shaped cells. (B) The Neuroform Atlas stent with its W-shaped cells and alternating cell counts per row. The pictures were provided courtesy of Stryker.
Antiplatelet therapy
At two sites, the antiplatelet therapy consisted of a dual antiplatelet medication (daily dose: 100–300 mg of aspirin and 75 mg of clopidogrel (loading dose: 300 mg)). The recommended duration of use was at least 5 days before the procedure followed by maintenance of the antiplatelet medication for at least 3–6 months after the procedure.6 Afterwards, patients were switched to aspirin only for a minimum of 6 months or for life. At the remaining centre, the daily dual antiplatelet therapy was initiated with 100 mg aspirin and 180 mg ticagrelor for a duration of 3 months followed by aspirin-only. In the case of clopidogrel non-response, this same regimen was employed at the first two centres. Platelet inhibition was tested by different methods, such as VerifyNow (Accumetrics, San Diego, California, USA) or light transmission aggregometry either 1 day before or immediately before endovascular treatment. A bolus of standard heparin (70–100 IU/kg) initiated anticoagulation, which was maintained through intravenous administration to sustain an activated clotting time of 250–300 s or 2–2.5 times that of baseline during the endovascular procedure.
Endovascular technique
Endovascular treatment was performed in a biplane angio-suite under general anaesthesia (Axiom Artis or Zee, Siemens Healtheneers, Erlangen, Germany). At the discretion of the treating physicians either coaxial or triaxial access was chosen, depending on vessel tortuosity. The optimal working projection was identified based on standard projections as well as 3D-rotational angiography. Using a standard 0.014 inch microwire, the microcatheter (SL-10 or a XT-17, Stryker) was placed in the parent vessel. Selection of the stent diameter was based on the manufacturer’s recommendation— that is, a 4 mm stent for ≥3.0 to <4.0 mm vessel diameter. Its length was chosen at the treating physician’s discretion, aiming to exceed the distal and proximal limits of the neck by at least 3 mm.
Representative cases illustrating the procedure and effectiveness assessment are shown in figures 2–4.
- Download figure
- Open in new tab
- Download powerpoint
Case 1 is a patient with incidental bilateral middle cerebral artery bifurcation aneurysms. Both aneurysms were coiled with additional placement of an Atlas stent. The one on the left was treated in a sequential fashion, the results are seen here.
- Download figure
- Open in new tab
- Download powerpoint
The one on the right was treated with the jailing technique, which also leads to complete aneurysm occlusion.

{kind=link}
{kind=link}
Case 2 has a very wide-necked aneurysm on the V4 segment of the left vertebral artery. The second image shows good coil retention of the Neuroform Atlas, leading to an adequate coiling result.
Endpoints
The effectiveness of the interventional procedure was assessed at the end of the treatment session by consensus of two interventional neuroradiologists according to the revised Raymond-Roy occlusion classification (RROC).7 Follow-up examinations five (±1) months after treatment consisting of high-resolution time-of-flight magnetic resonance angiography (MRA) (angiography before and after application of intravenous gadolinium-based contrast agent).8 9 An example of the images obtained can be seen in figure 5. If reperfusion was suspected based on the MRA images, digital subtraction angiography (DSA) was performed to determine if re-treatment would be necessary.
- Download figure
- Open in new tab
- Download powerpoint
Enlarged time-of-flight magnetic resonance angiography of an anterior communicating artery aneurysm treated with the Neuroform Atlas and coils. Evaluation of vessel patency is possible even in small vessels like the A1 or A2.
A detailed neurologic examination (ie, absence of transient ischemic attack, minor or major stroke) was performed immediately after the procedure, at 2 hours after the procedure, during the clinical visit on the following day, and at discharge. Follow-up to assess functional outcome base on the modified Rankin Scale (mRS) was performed by a board-certified neuroradiologist, neurosurgeon, or neurologist.10 Morbidity was defined as a mRS score ≥2 at any point. The attending neurointerventionalist rated technical safety, including navigation, visibility, deployment, opening, and vessel wall apposition of the stent.
Statistics
Differences in variable distribution between groups were compared using Kruskal-Wallis tests for continuous variables and χ²-tests for categorical variables. All statistical analysis was undertaken with SPSS, version 22.0 (IBM, Armonk, New York, USA).
Results
Patient and aneurysm characteristics
Thirty-six patients (24 female; median age 56; age range 19–75) with 37 aneurysms treated with the Atlas stent were included. Thirty-four patients had unruptured aneurysms, two had had a subarachnoid hemorrhage. Aneurysm location was the anterior communicating artery in 18 cases (49%), middle cerebral artery in 10 (27%), internal carotid artery in four (11%), basilar artery in four (11%), and posterior communicating artery in one case (3%). The median aneurysm diameter was 4.5 mm (range 1.3–25.2 mm) with a median neck size of 3.3 mm (range 1.8–9 mm). Median vessel diameter was 2.6 mm (range 1.5–4.3 mm) proximal to the aneurysm and 2.2 (range 1.5–4.0 mm) distal to the aneurysm. Two aneurysms had been previously treated, one with coils and the other with a Medina device (Medtronic, Irvine, USA). A comprehensive overview of patient demographics and baseline clinical features is shown in table 1.
Patient demographics and clinical symptoms
Effectiveness and technical results
In all patients and for all aneurysms, the Neuroform Atlas stent could be navigated to the target vessel and was deployed successfully across the aneurysm neck. After placement, the aneurysm was coiled either through the jailed microcatheter (16 cases, 43%) or the microcatheter that was used to place the stent was advanced through the stent into the aneurysm and used for coiling (21 cases, 57%). Likewise, the subsequent coiling was successful in all cases regardless of the chosen technique (jailing/sequential). Advancing the coiling catheter through the stent struts was unproblematic in all cases. The stent always kept the coil basket inside of the aneurysm and coil protrusion through the stent cells or stent dislocation during the coiling was not observed. Immediate angiographic outcome was assessed as either RROC 1 (31/37 aneurysms, 84%) or RROC 2 (16%). Details of the angiographic procedure and occlusion grades at follow-up are listed in table 2.
Aneurysm features and details of the angiographic procedure
Safety and outcome
One patient experienced a transitory ischaemic attack and presented with a minor hemiparesis after extubation. An MRI was immediately performed and showed multiple fresh lesions in the diffusion-weighted MRI sequence, which were most likely due to peri-interventional emboli. To exclude in-stent thrombosis, DSA was performed and showed no signs of thrombus or vessel occlusion. At the time the DSA was performed (approximately 2 hours after symptom onset) the clinical deficit had completely resolved. Follow-up data (4–6 months after the procedure, median 6.1 months) were available for 29 patients. Twenty-seven (93%) aneurysms remained completely occluded (RROC 1) and two aneurysms (7%) showed residual perfusion at the neck (RROC 2). More severe reperfusion was not seen in any case and no re-treatment was required. All patients received high-resolution time-of-flight MRA. In nine of the 29 cases (31%) additional DSA was performed to confirm the MRA findings. Longer follow-up data (12.3 months) were available for only five patients, who were all RROC 1 (100%).
None of the patients developed new symptoms and no permanent deterioration in mRS score was observed. Overall mortality and morbidity at follow-up was 0%.
Discussion
In this multicenter post-marketing registry, the Neuroform Atlas stent was evaluated for stent-assisted coiling of broad-based intracranial aneurysms. This new intracranial stent dedicated for vessels between 2 and 4 mm appears to be a promising, safe, and effective alternative for stent-assisted coiling. In this series, all stents were deployed successfully and the aneurysms could be coiled without technical problems.
Technical success was achieved in 100% of cases. This is similar to, or better than, previously published results using other stents. For the LVIS Jr, Behme et al reported a success rate of 100%,11 Fiorella et al experienced a 93.5% success rate for the LVIS,12 while Aydin et al reported a 97.5% success rate using the Leo baby13 and Mocco et al saw a 95% success rate using the Enterprise stent.14
Stent placement was possible in all cases and—due to the relatively small foreshortening—could be performed accurately. No apparent expansion failures were observed. When in doubt we acquired a flat-panel detector CT image; an example is shown in figure 6. In all cases the stent struts were sufficiently adapted to the vessel wall. Whenever a sequential technique was chosen for coiling, probing of the aneurysm through the stent cells was unproblematic. Visibility of the device was sufficient, although the stent struts are not radiopaque, as shown in our illustrations.
- Download figure
- Open in new tab
- Download powerpoint
In a patient with a middle cerebral artery aneurysm and an additional, previously treated internal carotid artery aneurysm the Neuroform Atlas is visible outside the artefacts.
In tortuous vessels, in particular, there was no relevant anatomical displacement of the vessel, but nonetheless, the stent expanded without problems. In the early years of stent-assisted coiling, immediate aneurysm occlusion rates were relatively low. Piotin et al, for example, reported a complete occlusion rate of 46.3% for stent-assisted coiling compared with 63.5% complete occlusion for bare coiling.15 A meta-analysis of stent-assisted coiling done by Shapiro et al 16 reported 45% complete occlusion in stent-assisted coiling. However, in recent years, the new microstents have considerably improved these numbers. In 2014, Möhlenbruch et al reported an immediate complete occlusion rate of 75% with the LVIS Jr stent.17 Aydin et al 13 reported a 75% complete occlusion rate when using the Leo baby stent. These occlusion rates are comparable to the 84% complete occlusion rate determined in our study. The vast improvement in immediate angiographic outcome might be a result of advancements in stent design, resulting in better wall adherence and superior coil scaffolding allowing for a higher packing density. Another factor influencing occlusion rates might be that the older stents were used in larger aneurysms compared with the smaller aneurysms located along small vessels, treated with the newer microstents. The mean aneurysms size of the aforementioned study by Piotin, for example, was 9.7 mm in the stented group compared with 4.5 mm in our series.15
With no permanent morbidity and mortality and a peri-interventional complication rate of 1/37 (2.7%), our results are comparable to recent studies using the LVIS Jr stent, with 3% morbidity and 1% mortality.18 Similarly, for the Leo baby stent, the reported morbidity and mortality rates were 3.8% and 0%, respectively.13 The incidence of morbidity and mortality were 2.8% and 2% for the Enterprise stent14 and 1.4% and 0% for the LVIS stent, respectively.19
We noticed several technical improvements using the Neuroform Atlas stent; the most obvious being that all stent sizes can be deployed through a 0.0165 inch microcatheter, allowing a sequential technique where the same catheter that is used to place the stent is then used to coil the aneurysm, in addition to the usual jailing technique. The Neuroform Atlas stent design, a combination of open- and closed-cell design, is supposed to combine the advantages of both cell types. The closed cell at the proximal end facilitates recrossing the stent for coiling and provides stable adherence to the vessel wall. Furthermore, since it is a laser-cut stent, the foreshortening is negligible, which allows for accurate placement. The cell size has been decreased compared with its predecessor (ie, the Neuroform stent) to reduce coil protrusion and to allow the use of smaller coils. Another observed advantage of the Neuroform Atlas stent is the absence of a leading tip of the stent wire, possibly reducing the risk of distal vessel perforation. Additionally, this might facilitate deployment of the Atlas in very tortuous vessels or before a sharp bend in which a leading tip could injure the vessel wall. However, the stent is less visible than the LVIS Jr or the Leo baby stent since only the stent markers at each end of the stent are radiopaque but the struts themselves are not visible. Nevertheless, the visibility of the Atlas stent was sufficient to allow accurate placement and deployment of the device in this study. Owing to its partially open-cell design, resheathing of the device is not possible. Therefore, accurate and reliable measurements should be taken before choosing the stent size. If there is doubt about complete opening of the stent (which we did not experience in our series), the struts can be visualized by unenhanced flat-panel detector CT.
We acknowledge that there are several limitations associated with this study. First, this was a small non-randomized case series of 36 consecutive patients. Therefore, there might have been selection bias, and no control group undergoing alternative neurointerventional treatments was used. However, inclusion followed clearly defined criteria and our cohort is the first multicenter registry of this new device. Second, follow-up imaging could be performed in only 78% of the casesand long-term follow-up of ~12 months was available in only 5 cases (13%) at the time of publication.
In conclusion, in this case series the Neuroform Atlas stent provided satisfactory technical safety and a high rate of immediate complete occlusion. However, long-term angiographic follow-up is still needed to observe long-term durability, recurrence rates, and the need for re-treatment.
References
Footnotes
Contributors Conception and design, CU and MAM. Data acquisition, all authors. Drafting the article, CU and MAM. Critically revising the article, all authors. Final approval of the version to be published, all authors. Agreement of accountability for all aspects of the work, all authors.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MB has received honoraria or is consultant for Guerbet, Novartis, Codman, and Roche. MM has received honoraria or is consultant for Acandis, Codman, Microvention, and Phenox.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at Parts of the results have been presented at WFITN 2017 and Neurad 2017.