Article Text

Abstract
Introduction Completed randomized trials on endovascular thrombectomy (ET) did not independently assess the efficacy of ET in the elderly (≥80 years old) who were often excluded or under-represented in trials. There were also inconsistent criteria for patient selection in this population across the different trials. This work evaluates outcomes after ET for acute ischemic stroke (AIS) in the elderly at a high volume stroke center.
Methods We reviewed all cases of AIS that underwent a direct aspiration first pass technique (ADAPT) thrombectomy for large vessel occlusions between March 2013 and October 2017 while comparing outcomes in the elderly with younger counterparts. We also reviewed AIS cases in elderly patients undergoing medical management who were matched to the ET counterparts by demographics, comorbidities, baseline deficits, and stroke severity.
Results Of 560 patients undergoing ET for AIS, 108 patients were in the elderly group (≥80 years of age), and had a significantly lower likelihood of functional independence (defined as a modified Rankin Scale score of 0–2) at 90 days compared with younger patients (20.5% vs 44.4%, P<0.001), and higher mortality rates (34.3% vs 20%, P<0.001). When compared with patients undergoing medical management, elderly patients did not have a significant improvement in rates of good outcomes (20.5% vs 19.5%, P>0.05), and had significantly higher rates of hemorrhage (40.7% vs 9.3%, P<0.001). We also identified baseline stroke severity and the incidence of hemorrhage as two independent predictors of outcome in the elderly patients.
Conclusions ET in the elderly did not show a similar benefit to younger patients when compared with medical management. These findings emphasize the need for more optimal selection criteria for the elderly population to improve the risk to benefit ratio of ET.
- stroke
- thrombectomy
- elderly population
- age
Statistics from Altmetric.com
Introduction
Following the success of several trials on endovascular thrombectomy (ET) for acute ischemic stroke (AIS) in 2015, ET has become a standard of care for the management of stroke patients.1–4 Although the trials predominantly investigated outcomes in anterior circulation large vessel occlusion (LVO) and often selected adults <80 years old, real world practices have expanded the use of ET to posterior circulation stroke,5 elderly patients,6 more distal vessel occlusions, patients with a low National Institute of Health Stroke Scale (NIHSS) score,7 and other subpopulations of AIS patients.
Evaluating the efficacy of ET in elderly patients has become of specific interest recently, especially given that advanced age is generally an independent predictor of poor outcomes after ET.5 8 9 Elderly patients (≥80 years old) have been either excluded or under-represented in clinical trials of ET which reported conflicting evidence regarding the benefit of ET in this population.2 3 10–15 Although recent data from HERMES suggested a significant effect of ET in the elderly,14 this age group was still under-represented,16 included patients with variable selection criteria, and included data from trials preferentially favoring younger age groups in the elderly (80–85 years).1 3 Prospective trials designed specifically to evaluate the safety and efficacy of ET in this elderly sub-population, and determine the optimal candidates for intervention, are still pending.
Therefore, the aim of this study was to retrospectively assess the safety and outcomes of ET in elderly patients in a ‘real world’ practice at a high volume stroke center. We compared the outcomes between elderly patients (≥80 years old) and younger adults (<80 years old) following ET for AIS. To assess whether ET provides an additional benefit compared with medical management with the standard of care in the elderly patients, we compared outcomes after AIS in the elderly for patients undergoing ET to matched controls receiving medical management. We also compared the difference in characteristics of patients among the elderly (≥80 years old) who achieved good functional recovery compared with those with poor outcomes after ET to determine predictors of good outcome after ET in this population.
Methods
Patient selection
We retrospectively studied a prospectively maintained database of AIS cases that underwent a direct aspiration first pass technique (ADAPT) thrombectomy at a tertiary care center between January 2013 and November 2017, including all age groups (see online supplementary figure 1). In addition, we reviewed the stroke registry at the Medical University of South Carolina for patients who underwent medical management for AIS with LVO without ET. Patients selected from the medical arm were not offered ET due to only advanced age in some cases (19%), delayed presentation (>12 hour) in 42%, or due to lack of defined penumbra and completed infarct after transfer from the outside hospital and that was deemed unlikely to recover neurological function. The study was approved by the institutional review board at the Medical University of South Carolina.
Supplemental material
Patients underwent ADAPT thrombectomy if CT perfusion imaging demonstrated a mismatch between cerebral blood volume and blood flow corresponding to regions of penumbra that could significantly contribute to their presenting NIHSS score, irrespective of time of onset.17 For posterior circulation LVO, ADAPT was performed unless a patient presented after 10 hours of symptom onset and diffusion weighted imaging showed extensive infarct (more than half of the brainstem on any axial MRI slice) for which benefit from the procedure is not expected. Patients who met criteria for intravenous tissue plasminogen activator (IV tPA) received thrombolytic therapy. Whether a patient received IV tPA did not affect the decision to perform ET or the timing of the procedure.
Mechanical thrombectomy
All patients undergoing ET for AIS underwent ADAPT thrombectomy with the exception of 15 patients who were enrolled in an independent study evaluating stent retriever thrombectomy. ADAPT thrombectomy was performed as described previously.17 18 Direct aspiration was performed using the largest caliber aspiration catheter the target vessel could safely accommodate; larger caliber catheters, including 5 MAX, 5 MAX ACE, ACE 64, and ACE 68, were mainly used (Penumbra, Alameda, California, USA) and smaller caliber catheters, including 4 MAX and 3 MAX, were used when needed (Penumbra). Patients predominantly underwent conscious sedation for the procedure, and general anesthesia was rarely used (9% of cases). Following the ADAPT protocol, direct aspiration is attempted 3–4 times before an additional device, such as a stent retriever, is used at the discretion of the operating physician.
To assess for postprocedural hemorrhage, a CT scan was obtained within 12–24 hours of ET and scored by a neuroradiologist blinded to the study.
Patients undergoing ET were divided into two groups (60 to <80 years of age) and (≥80 years of age). The age of 80 years as the cut-off was based on the age limits of prior trials as well as on preliminary data showing that the likelihood of good outcome versus age curve starts to drop at the age of 80 years (see online supplementary figure 2). The choice of 60 to <80 years as a comparison group was chosen to compare the elderly population with older adults with similar comorbidities rather than with younger adults that are expected to have significantly better rates of good outcomes and different baseline characteristics.
Patients selected for the non-ET group included patients who presented to the Medical University of South Carolina during the same study period with AIS and LVO who underwent medical management per standard stroke protocols.
Data collection
Patient charts were reviewed for demographics, comorbidities, pre-stroke deficits, admission deficit, and treatment, including whether IV tPA was administered. ET procedure notes were reviewed for procedural variables, including the number of reperfusion attempts, the final Thrombolysis in Cerebral Ischemia (TICI) score, and complications. Postprocedural CT scans were reviewed by a blinded neuroradiologist to assess and score postprocedural hemorrhage using the ECASS system.19
Outcomes
The 90 day modified Rankin Scale (mRS) was used as the primary outcome. Additionally, 90 day NIHSS, mortality, and length of stay were also used as secondary outcome measures. An mRS score of 0–2 at 90 days was considered a ‘good’ outcome whereas an mRS score of ≥3 was considered a ‘poor’ outcome. Both the 90 day mRS and the 90 day NIHSS were collected during a routine follow-up visit with a stroke neurologist at 90 days (±14 days) after stroke onset in the majority (92%) of patients. Patients who did not present for the 90 day visit were contacted along with their caregivers by telephone at 90 days after the stroke. In a small percentage of patients (3.6%), 90 day outcomes were not available and 30 day outcomes were alternatively used if available.
Statistical analysis
Statistical analyses were performed using SPSS V.24 (IBM Corporation, New York, USA), and Graphpad Prism 6 (Graphpad, La Jolla, California, USA). Descriptive statistics and univariate analysis were used as follows: Student’s t test for continuous measures, Mann–Whitney test for non-continuous variables or with failed normality, and the χ2 test for categorical measures. Two sided comparisons were used and α<0.05 was considered statistically significant.
Multivariate regression analysis was used to assess whether age (dichotomized to <80 years and ≥80 years) is an independent predictor of functional independence or mortality after ET. Two logistic regression models were performed with 90 day mRS (dichotomized into good (mRS 0–2) and poor (mRS 3–6)) or mortality as outcome measures. Model performance was assessed using the Hosmer–Lemeshow test and c statistic. Variables included in the models were: gender (women vs men), race (white vs not white), time from onset to groin (min), admission NIHSS score, pre-stroke mRS, Alberta Stroke Program Early CT (ASPECT) score, number of vessels involved, IV tPA (yes vs no), intra-arterial (IA) tPA (yes vs no), number of attempts, procedure time (min), final TICI flow (dichotomized into recanalized (TICI 2b–3) or non-recanalized (TICI 1–2a), comorbidities (hypertension, hyperlipidemia, atrial fibrillation, and diabetes each as yes vs no), prior stroke (yes vs no), procedural complications, and age (<80 vs ≥80 years).
For comparison of ET to medically managed patients, those with ET (n=121) were matched to medically managed patients (total pool=1213) by the following variables: age, gender, race, baseline NIHSS, pre-stroke mRS, comorbidities, history of prior stroke, and use of IV tPA. A fuzzy matching algorithm was used in SPSS to ensure there were no significant differences between the two groups. A total of 108 patients per group were matched by these variables, and then compared for outcome measures. Comparisons between outcomes of the two groups were performed using descriptive statistics and univariate and multivariate analyses, as described above.
Results
Patient population
A total of 560 patients underwent ET for AIS during the study period, of whom 15 patients did not undergo ADAPT thrombectomy and were excluded from the analysis. As our study focused on the elderly population compared with patients aged 60 to <80 years, 124 patients <60 years of age were excluded from the statistical analyses. Of the remaining patients, 85 were lost to follow-up after discharge. Therefore, 336 patients (108 patient s≥80 years old) were included in the analyses (see online supplementary figure 1). Of the included patients, six patients did not have detailed procedural information and were excluded from table 1. As detailed in the methods, a matched subset of medically managed patients of at least 80 years old was also identified, and 108 patients from this group were included.
Comparison of baseline characteristics, and procedural and outcome measures in patients aged 60–<80 years and those aged ≥80 years
Outcomes after ET in elderly patients compared with older adults
We first examined how 90 day outcomes post-ET measured by the mRS scores changed across different age groups. Age was associated with a left shift in the mRS distribution curve and with a decreased likelihood of a good outcome with increasing age (figure 1). The curve representing the distribution of 90 day outcomes in older adults (60–<80 years) and elderly patients (≥80 years) by subsets of age groups demonstrates an inflection point in the ‘good’ outcome and ‘poor’ outcome curves around 80 years of age (see online supplementary figure 2). Therefore, to evaluate outcomes of elderly patients (≥80 years) following ET while controlling for preprocedural and procedural comorbidities, this group was compared with older adults (60–<80 years old). As shown in table 1, preprocedural variables, including race, pre-stroke functional independence (mRS 0–2), baseline NIHSS, time from onset to the groin, use of IV tPA, proportion of posterior circulation strokes, and the number of vessels involved were not significantly different between the two groups. Patients in the elderly group had a higher proportion of women (68.5% vs 45.8%, P<0.01), and a significantly higher ASPECT score (8.5 vs 7.8, P<0.001). There were no significant differences in comorbidities between the two groups, and there were no significant differences in all procedural variables investigated in this study (table 1).

(A) Shift in 90 day modified Rankin Scale (mRS) score after endovascular thrombectomy (ET) in acute ischemic stroke patients stratified by age group. (B) Likelihood of good outcome (mRS 0–2) 90 days after ET across different age groups.
With respect to functional outcome, patients in the elderly group had a significantly higher median mRS score at 90 days (p<0.001), and significantly lower rates of good outcome compared with the 60–<80 year age group (P<0.001) (table 1). Mortality at 90 days post-ET was also significantly higher in the elderly group compared with the 60–<80 year group (34.3% vs 20%, P<0.001) (table 1). There was no significant difference in length of stay between the two groups.
To assess whether age ≥80 years old was an independent predictor of functional outcome and mortality at 90 days, two independent multivariate regression models were performed (table 2). Age ≥80 years was independently and inversely correlated with good outcome (OR=0.42, P=0.015), as well as an independent predictor of mortality (OR=3.56, P<0.001) on multivariate logistic regression. In addition to age, predictors of good outcome on multivariate analysis included low baseline NIHSS, lower pre-stroke mRS, and lower number of attempts to reperfusion (table 2). Independent predictors of mortality were race (not white), pre-stroke mRS, and baseline NIHSS (table 2).
Multivariate analysis for predictors of good outcome and mortality at 90 days after endovascular thrombectomy
Outcomes after ET versus medical therapy in elderly patients
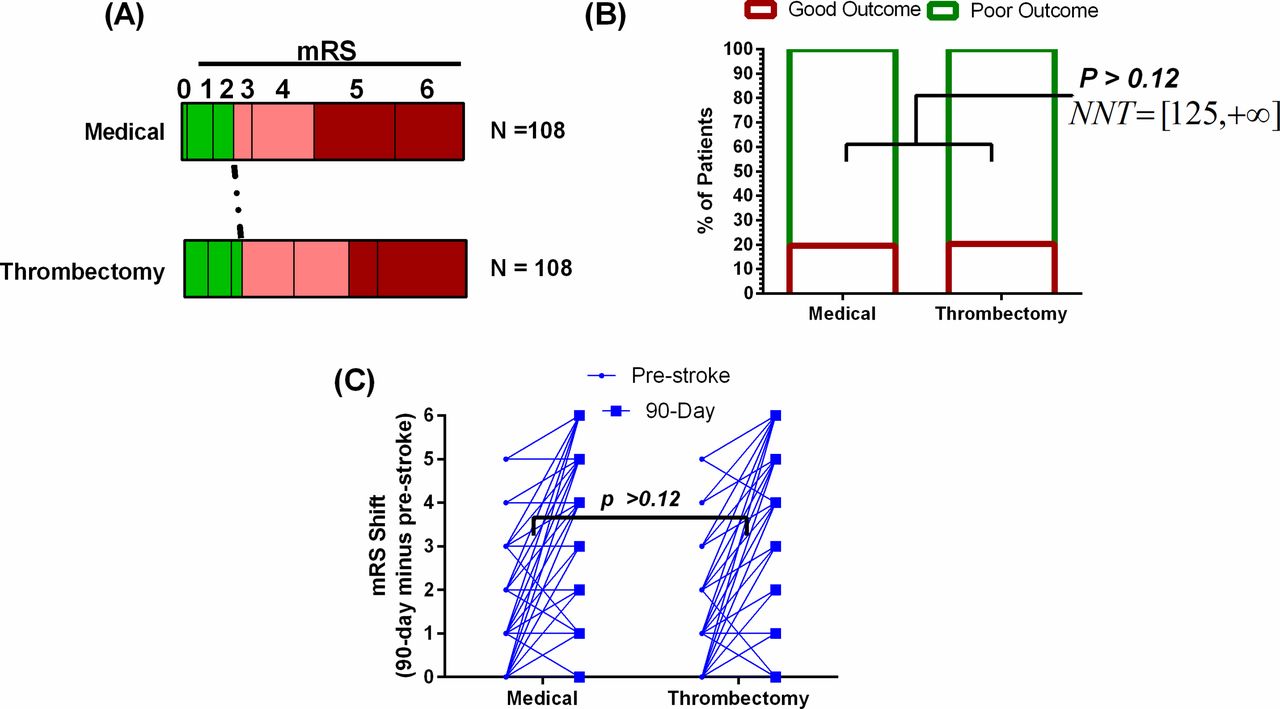
We then compared outcomes in patients who underwent ET for LVO with those who were managed medically. Baseline characteristics comparing both groups showed no significant difference in preprocedural variables, including age, gender, race, pre-stroke level of functioning (mRS), baseline NIHSS on admission, comorbidities (diabetes, hypertension, hyperlipidemia, atrial fibrillation), history of prior stroke, proportion of posterior circulation stroke, or use of IV tPA (table 3). We then assessed outcomes measured as 90 day mRS scores, mortality, length of stay, and post-procedural hemorrhage. There were no significant differences in median mRS scores between the ET and medical groups (4 (IQR 3) vs 5 (IQR 2), P>0.05), likelihood of good outcome (20.5% vs 19.5%, P>0.05), or length of stay (9.4 vs 10.5, P>0.05). However, patients undergoing ET had a significant increase in rates of postprocedural hemorrhage compared with medical therapy (40.7% vs 9.3%, P<0.001), with a similar trend observed with parenchymal hematoma 2 (PH2) type hemorrhage alone (0.9% vs 5.6%, P=0.05). There was no significant difference in mortality between the two groups (table 3). The distribution of individual mRS scores at 90 days for the two groups is provided in figure 2. Since no significant difference was observed with ET in the elderly, the computed number needed to treat ranged from 125 to +∞ (figure 2B). We also computed whether ET had a positive effect on reducing the increase in mRS between pre-stroke mRS and 90 day mRS compared with medical therapy, but no significant difference was observed (P>0.05) (figure 1C).

{kind=link}
{kind=link}
(A) Distribution of functional outcome (modified Rankin Scale (mRS)) at 90 days, showing the effect of endovascular thrombectomy (ET) on functional outcome compared with medical therapy. (B) Comparison of rates of good outcome with medical therapy compared with ET. No significant difference was observed on categorical testing. Number need to treat (NNT) calculated shows a lower limit of 125 with an upper limit of positive infinity given the lack of statistical significance. (C) Change in mRS between pre-stroke and 90 days post stroke showing that ET does not significantly affect the change compared with medical therapy. Mann–Whitney test was used. n=108/group.
Characteristics of elderly (≥80 years of age) patients in thrombectomy compared with medical management, matched by baseline variables
Predictors of good outcome in the elderly population
Patients in the elderly group undergoing ET were then subgrouped into those with good and poor outcomes for subsequent analysis of factors associated with a good outcome (table 4). On univariate analysis, elderly patients with good outcomes had a significantly lower baseline NIHSS, lower pre-stroke mRS, longer time from onset to the groin, lower number of branches involved, required less number of reperfusion attempts, and had a lower incidence of postprocedural hemorrhage (table 4). Patients with a poor outcome were found to have a longer length of stay compared with patients with good outcomes. On multivariate analysis, initial deficit (baseline NIHSS) in addition to postprocedural hemorrhage were the only independent and significant predictors of functional outcome at 90 days (table 4).
Comparison of patients at least 80 years old who had good versus poor outcome after thrombectomy
Discussion
This study has found that in a ‘real world’ high volume stroke center, rates of ‘good’ (mRS 0–2) outcomes for elderly patients (≥80 years old) undergoing ET for AIS from LVO are inferior to those in younger patients. The number needed to treat therefore increases from approximately 2.5 patients in those <80 years of age, to at least 125 and possibly as high as infinity (mathematical equivalent of ‘no benefit’) in the elderly. Acute stroke care providers should assess their own experience and outcomes in treating octogenarians at their centers so that they may provide families with an accurate expectation when offering thrombectomy. This stark difference in the number needed to treat based on age may also have cost, systems of care, and resource utilization implications that may warrant further analysis at centers providing this level of expertise.
In addition, while rates of good outcome in the elderly following ET are no better than standard medical management in their age matched controls, there was an associated increased (fourfold) risk of postprocedural hemorrhage. These findings suggest that, utilizing the same selection criteria for ET as those employed in the younger patient population, ET may be harmful and does not provide a benefit compared with medical management alone. It also underscores the importance of developing better and more stringent selection criteria to octogenarians with LVO and AIS.
Confirming prior findings, advanced age was associated with a lower likelihood of a good outcome after ET, and elderly patients had higher mortality and higher mRS scores at 90 days, despite comparable baseline features, comorbidities, and procedural variables. Our findings showing poor outcomes after ET are consistent with prior single arm studies, as previously reviewed by Jayaraman et al 20 and as reported in an earlier meta-analysis.21 Some studies attributed worse outcomes in the elderly to potential higher comorbidities, procedural variables, and impaired collaterals.20–22 In our work, being an octogenarian was an independent predictor of poor outcome even when comorbidities and procedural variables were accounted for. Although a previous report mentioned lower success rates of ADAPT23 or stent retriever thrombectomy24 in the elderly, there were no differences in the rates of successful ADAPT between elderly and younger patients in our cohort.
We also found that NIHSS on admission in addition to the presence of postprocedural hemorrhage were independent predictors of good outcomes in the elderly population. Although randomized controlled trials on ET for AIS with LVO were not specifically designed to investigate the safety and efficacy of ET in the elderly, subgroup analysis for the elderly age group (≥80 years old) were performed on a post hoc analysis, but have demonstrated conflicting results.2 3 10–15 The recently completed Diffusion Weighted Imaging or Computerized Tomography Perfusion Assessment with Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) trial reported that ET was effective in patients >80 years old who had an NIHSS score of 10 or higher and <21 mL of infarct volume on imaging.15 Despite this selection, the effect size in the elderly population was relatively small, and only 25 patients were included from this age group. However, the results of DAWN have further emphasized the need for optimal selection criteria for elderly patients different from those used in younger patients. Table 5 summarizes the difference in selection criteria for elderly patients in major ET trials and the resulting outcomes for this population. In addition to the fact that the majority of studies excluded patients >80 years old or did not analyze this group separately, different parameters were chosen for patient selection for ET among the elderly, and reported outcomes were conflicting. Although Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands (MR CLEAN) and DAWN trials showed a significant benefit with ET in the elderly with anterior circulation LVO, Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE), Randomized Trial of Revascularization with Solitaire FR Device vs Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting within Eight Hours of Symptom Onset (REVASCAT), and Trial and Cost Effectiveness Evaluation of Intra-arterial Thrombectomy in Acute Ischemic Stroke (THRACE) did not show a similar effect. This variability in outcome with relatively low effect sizes presents an obstacle to the application of trial findings to ‘real world’ practice, especially in an acute setting when careful selection of patients may not be feasible given the time sensitivity and if there is an insufficient family presence to provide adequate collateral history.2 3 10–15
Selection criteria and efficacy of endovascular thrombectomy in the elderly in recent trials
In our cohort, elderly patients had a statistically significant higher ASPECT scores compared with younger patients undergoing ET; however, the overall difference of 0.7 between the two groups falls below the common variability in ASPECT scores (± units) which limits the clinical significance of this difference. Yet, a potential bias in selecting those patients with smaller core infarcts when >80 years of age cannot be ruled out.
In our experience, we have not observed a benefit for ET in the elderly population who were selected for intervention utilizing the same CT perfusion based triage system that is applied to younger patients. Notably, both our medical arm elderly patients and younger patients treated with ET showed a comparable likelihood of achieving good outcomes, as reported in major trials (see online supplementary figures 3 and 4).14 25 This further supports the fact that the lack of benefit in the elderly population is not likely technique or management related as the difference in outcomes between our studies and successful ET trials is not observed in medically treated patients (medical arm) or younger patients with ET. It is also important to emphasise that our data refer to ADAPT thrombectomy compared with stent retriever thrombectomy used in major trials; however, the recently completed Contact Aspiration versus Stent Retriever for Successful Revascularization (ASTER) and Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trials demonstrated comparable technical and clinical outcomes in patients undergoing either procedure.26 27
Additional predictors of outcome
Our study also shows that in addition to postprocedural hemorrhage, pre-stroke baseline function and NIHSS on admission were two predictors of outcome after ET in our cohort. This explains why randomized controlled trials employing ET which excluded patients with mRS >1 at baseline found a significant benefit following intervention and higher rates of good outcomes than in our ‘real world’ experience, although this was not always consistent across studies.11 13 15 28 Our findings support the use of pre-stroke level of functioning as well as baseline NIHSS in patient selection given that patients with higher mRS and higher admission NIHSS have increased odds of mortality and poor outcomes. Our study showed a fourfold increase in the occurrence of postprocedural hemorrhage in patients with ET compared with their medical counterparts, around 14% of which was graded as PH2 type hemorrhage. This is specifically important as it indicates that although outcomes are comparable between the two groups, the likelihood of hemorrhagic complications is significantly increased in patients undergoing ET compared with medical management. Although not significant on multivariate analysis, onset to groin time was significantly longer in patients with good outcomes compared with poor outcomes. This can be explained by the fact that patients with better collaterals who tend to do better after stroke, will also still be eligible for ET on CT perfusion despite longer onset to groin time.
Limitations
The retrospective nature of this study is one major limitation of this work, and the comparison between medical therapy and ET in the elderly was not based on prospective randomization. However, cases from either intervention were matched based on the most significant covariate related to outcomes to ensure comparable patients at baseline were assigned to either group; however, this may not have completely eliminated potential selection bias. It is also important to note that a large cohort of patients was included in this study (330 patients, 108 of whom were at least 80 years old). Angiographic and neurological outcomes were blindly collected by stroke neurologists not involved in data collection. Another limitation is that this study is from a single institution, and multicenter studies are still needed to explore similar findings. Yet, the fact that all cases were from a single institution with standard management and procedural protocols help to minimize procedural variability and disparities in perioperative patient care. Finally, this work did not investigate why patients ≥80 years old fare differently after ET compared with younger adults even in the absence of difference in comorbidities or baseline characteristics other than age. This question remains to be investigated and age related factors contributing to increased susceptibility to ischemic damage as well as reduced post-stroke neuronal plasticity with age are two important factors that may account for this difference, as predicted from preclinical studies.29 30 In addition, psychosocial factors may have a higher impact on stroke recovery in the elderly population compared with the young, and this remains to be investigated in the context of its implications on outcomes post-ET for AIS.
Conclusion
An analysis of our ‘real world’ experience in treating octogenarians with thrombectomy for LVO has demonstrated a rate of good outcomes that is (A) greatly inferior compared with younger patients, (B) equivalent to elderly patients undergoing medical management, and (C) associated with a higher rate of hemorrhagic complications. These findings highlight the importance of refining selection criteria in this elderly population, so that we may maximize the benefit to patients while minimizing the harm. Based on our experience, elderly patients with good baseline functioning (mRS 0–1) with uncomplicated anatomy predicting shorter procedure times and lower number of passes are more likely to benefit from ET using ADAPT. In addition, the number of attempts was significantly associated with poor outcome in the elderly. Ultimately, a modified selection protocol will be proven efficacious in a prospective fashion when it yields outcomes that more closely parallel those of younger patients.
References
Footnotes
Contributors Each author listed receives authorship credit based on material contribution to this article, their revision of this article, and their final approval of this article for submission to this journal.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AMS: Penumbra–consulting, honorarium, speaker bureau; Pulsar Vascular–consulting, honorarium, speaker bureau; Microvention–consulting, honorarium, speaker bureau, research; Stryker–consulting, honorarium, speaker bureau. AST, RDT, and MIC: Codman–consulting, honorarium, speaker bureau, research funding; Covidien–consulting, honorarium, speaker bureau; Penumbra–consulting, honorarium, speaker bureau, research grants; Microvention–consulting, honorarium, speaker bureau, research grants; Blockade–stock, consulting, honorarium, speaker bureau; Pulsar Vascular–stock, consulting, honorarium, speaker bureau, research; Medtronic–consulting, honorarium, speaker bureau.
Patient consent Not required.
Ethics approval The study was approved by the institutional review board at the Medical University of South Carolina.
Provenance and peer review Not commissioned; externally peer reviewed.