Article Text

Abstract
Background and Purpose Liquid embolic agents (LEAs) are the determinant tool for successful embolization of cranial arteriovenous shunts. There are few currently available LEAs. The aim of the study was to summarize our initial experience with a recently introduced non-adhesive ethylene vinyl alcohol (EVOH) copolymer based LEA (Menox 18) in the endovascular treatment of cerebral arteriovenous malformations.
Methods From April 2018 to November 2018, 24 patients harboring cerebral arteriovenous malformations underwent endovascular embolization with Menox 18. Clinical features, angiographic results, procedural details, complications, and follow-up details were prospectively collected and retrospectively analyzed.
Results Curative embolization in one endovascular session was achieved in 14/24 (58.3%) of the treated patients. Partial embolization was achieved in 10 patients (42.6%) in whom staged treatment with radiosurgery or microsurgical resection was planned. No mortality was recorded in our series. Clinical complications after embolization occurred in 1/24 (4.66%) patients. No technical complications were noted
Conclusions Our pilot study suggests that the Menox embolization system offers similar technical and clinical results in comparison with the other currently available LEAs. Further studies with larger cohorts and long term follow-up data are needed to fully evaluate its efficacy
- liquid embolic material
- arteriovenous malformation
- device
Statistics from Altmetric.com
Introduction
Endovascular embolization has emerged as one of the primary treatment modalities of intracranial arteriovenous malformations (AVMs). Historically, this method has been applied mostly as an adjuvant therapy for perioperative devascularization and/or volume reduction prior to open microsurgical or radiosurgical procedures.1–3 In addition, definitive endovascular treatment resulting in curative embolization in selected patients has also been increasingly reported in recent years.4–6 The success of endovascular embolization is highly dependent on technological advances, such as dual lumen balloon and detachable tip microcatheters, as well as the development of the non-adhesive liquid embolic agents (LEAs). The most widely used and highly effective agents are the two currently available ethylene vinyl alcohol (EVOH) based copolymers (Onyx (eV3-Covedien, Irvine, California, USA) and Squid (Balt Extrusion, Mont-morency, France)), and the precipitating hydrophobic injectable liquid (PHIL; Microvention Inc, California, USA).7 8 The Menox liquid embolic system (Meril Life Sciences, India Pvt Ltd) is another recently introduced EVOH based biocompatible copolymer with micronized tantalum powder added to the mixture for radiopacity. It is available in a lower viscosity of 18 centistokes containing 6% EVOH and 94% dimethylsulfoxide (DMSO). In the present report, we describe the first clinical experience with this new non-adhesive LEA in 24 patients.
Materials and methods
We performed a retrospective analysis of prospectively collected data. Between April 2018 and November 2018, 24 cerebral AVMs were treated with Menox LEA in our center. The initial four patients included in this study were selected based on the ease of catheterization and higher likelihood of successful embolization. The remaining 20 patients were treated consecutively, irrespective of their clinical condition or anatomical features. The following baseline characteristics were recorded: clinical presentation, AVM angioarchitecture (Spetzler–Martin (S-M) grade), dominant arterial supply, type of microcatheter used, approximate nidal reduction rate (%), and pre- and post-procedure modified Ranking Scale scores (table 1). Technical details and embolization characteristics in terms of procedure duration, number and total time of injections, volume of LEA applied, and time need to form a stable proximal plug were also assessed. Dimensional calculations and post-embolization estimated nidal size reduction were based on angiographic biplane images pre- and post-final endovascular treatment. Curative endovascular embolization was aimed for all patients harboring smaller AVMs, or S-M grade I or II.9 Staged endovascular embolization was performed in larger AVMs.
Demographic and clinical characteristics of the 24 treated patients
Procedural and technical details
Written informed consent was obtained from each patient and their relatives prior to each endovascular session according to local institutional policy. The decision to perform each endovascular embolization was based on consensus by the institutional multidisciplinary team of interventional neuroradiologists, neurologists, and neurosurgeons.
All procedures were performed under general anesthesia on a biplane angiographic unit (Innova GE Healthcare 31 31 IQ biplane). The patient’s blood pressure during and after the procedure was controlled and maintained between 90 and 110 mm Hg in order to prevent perfusion pressure breakthrough. Approximately one-third (9/24, 37.5%) of the lesions were accessed through distal radial access, and right femoral access was used in 15/24 (62.5%). After completion of diagnostic angiography, the diagnostic catheter was exchanged over an exchange length wire for a 6 F Softip XF guide catheter (Boston Scientific). In general, the guide catheter was positioned in the pre-petrous portion of the internal carotid artery or V3 vertebral artery segment and connected to a pressurized infusion bag of normal saline containing 10 mL of nimodipine solution.
Once the angioarchitecture of the AVM was defined and the appropriate pedicle for embolization was selected, a DMSO compatible Apollo (Medtronic, USA) microcatheter was navigated to the nidal part of the malformation over a 0.008 inch or 0.010 inch guidewire. A microcatheter angiography was performed to confirm optimal and safe positioning. Next, the deadspace of the microcatheter was injected with DMSO. The vials of Menox were placed into a shaker machine for at least 20 min prior to usage in order to ensure homogenous dispersion of the tantalum particles. Using well established EVOH injection techniques, the material was slowly injected via 1 mL syringe.10 A small amount of reflux over the detachable portion of the microcatheter and multiple shot cycled injections (push–pause technique) were used to create a stable proximal ’plug’. Control angiographies were obtained in between the injections to assess the nidal occlusion progression and the venous outflow pattern of the AVM. If untoward Menox penetration, such as microcatheter reflux, or extra-nidal or venous system extension was noted, the injection was temporarily stopped and resumed after a 1–2 min pause. In cases of persistent untoward Menox penetration, embolization was stopped completely. In cases of satisfactory nidal filling, embolization was carried out until complete obliteration or until the prespecified target volume reduction was achieved.
No antireflux modifications, techniques, or adjuvant devices were used in this cohort.11–14 All patients were monitored in the intensive care unit for 48 hours after the procedure
Results
Twenty-four patients with cerebral AVMs underwent endovascular embolization. Mean patient age was 40 years (range 5–71 years), and 15 (62.5%) were women. Among all treated AVMs, none had a previous endovascular treatment. Menox 18 was used in a total of 24 procedures. The average volume of Menox 18 injected was 4.5 mL (range 2.2–8 mL). A total of 32 pedicles were injected, ranging from 1 to 3 per case, resulting in 83% average estimated size reduction of the AVM (30–100%). Adequate nidal penetration was achieved in all cases. The mean procedure time was 60 min, with an average fluoroscopy time of 25 min. The mean injection time needed for stable proximal formation was 170 s. The mean duration of injections was 11.2 min (7.3–30 min) with an average number of 30 injections per procedure.
Curative embolization with complete nidal obliteration and no residual AVM visualization at the end of the procedure was achieved in 14/24 cases (58.3%) (figure 1).

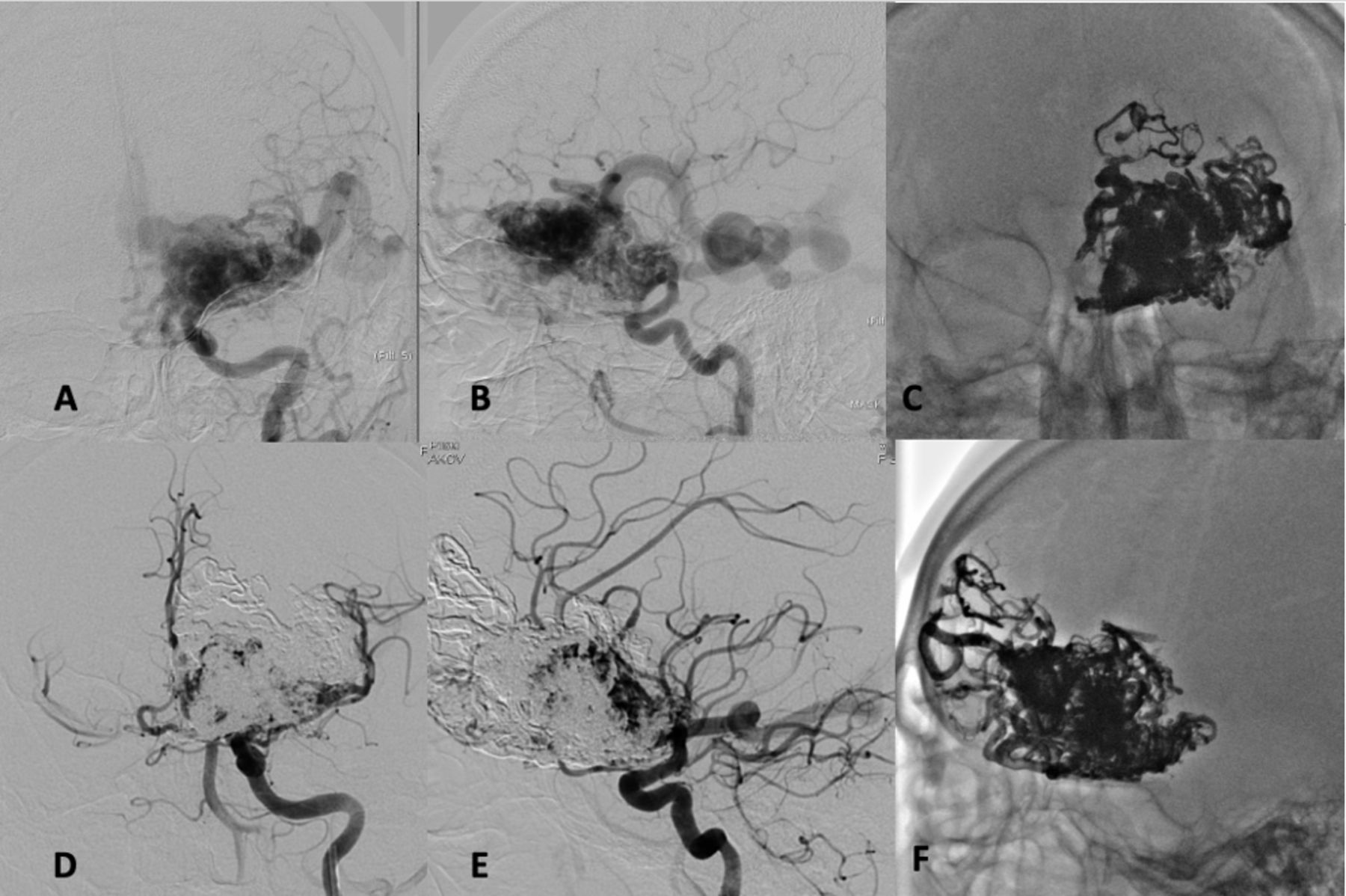
Patient with a ruptured, Spetzler–Martin grade II, left frontal arteriovenous malformation (AVM). (A, B) Anteroposterior and lateral DSA shows the AVM, fed by the left anterior cerebral artery. Injection through the Apollo microcatheter of the left anterior cerebral artery feeder demonstrating intra-nidal penetration of Menox. Curative embolization was confirmed on final angiography (D, E). Native image (F) of the Menox cast demonstrating adequate opacity of the embolic material.
Ten out of 24 (41%) lesions were partially obliterated (volume reduction rate 30–80%). Four of those patients had sufficient AVM nidal reduction suitable for stereotactic radiotherapy of the residual components. None of the patients included in this dataset had surgical resection. Additional staged embolization has been scheduled for the remaining six patients with a plan to achieve further nidal reduction as a complement to final definitive treatment (either surgical resection or radiosurgery) (figure 2).

Patient harboring a ruptured, Spetzler–Martin grade IV, arteriovenous malformation. Internal carotid artery DSA (A, B) demonstrating multiple arterial feeders from the left middle cerebral and left anterior cerebral arteries. Substantial nidal embolization (approximately 80%) was achieved, as evidenced by the final angiograms (D, E). Native anteroposterior (C) and lateral (E) images demonstrating the Menox cast.
Complications
There were no major technical complications during or after the embolization. However, one patient harboring an AVM S-M IV (1/24, 4.16%), which was partially obliterated, experienced a clinical complication. The patient reported a severe headache after the procedure. CT scan revealed a small subarachnoid hemorrhage. The patient was discharged home without permanent clinical sequelae. There was no mortality in our case series. No technical complications, such as microcatheter entrapment or rapid tantalum sedimentation, were observed in this cohort of treated patients. No adverse physiological effects, such as hemodynamic changes or signs and symptoms of allergic reaction, were noted.
Follow-up
Six month angiographic and clinical follow-up was available for 17/24 patients. Good clinical outcome (modified Ranking Scale score <2) was confirmed for all 17 patients. The remaining seven patients are still within <6 months since the last procedure. No angiographic or cross sectional MR angiography data of AVM recurrence was noted in the patients in whom complete embolization was achieved.
Discussion
Rapid technological advancements in the neuroendovascular field as well as increased utilization of LEAs and materials have made a significant impact on the treatment of cerebral AVMs and shunts. Currently, Onyx remains the most commonly used non-adhesive LEA for intracranial endovascular embolization. This EVOH based agent allows slow polymerization and less adhesiveness and thus it provides excellent control and ability to start or interrupt injections during the embolization process.15 16
In this study, we described our initial clinical and technical experience with the use of the recently introduced EVOH based LEA, Menox 18, for embolization of cerebral AVMs. Introduced in 2018, Menox is a non-adhesive EVOH copolymer that allows multiple cycles of short lived and continuous injections. Similar to the other available EVOH based agents, Menox advances into the vasculature with a lava-like flow pattern without any fragmentation during injections (figure 3).17

{kind=link}
{kind=link}
{kind=link}
Photograph showing the lava-like formation of Menox cast being injected through a microcatheter in 0.9% NaCl suspension. The polymer solidifies centripetally in one solid mass.
The key components of the Menox embolization system are: (1) 1.5 mL phial of the liquid embolic agent; and (2) 1.5 mL phial of DMSO. The agent contains suspended tantalum and requires at least 20 min of shaking prior to the procedure. In terms of particle size of the tantalum powder according to the manufacturer, Menox has nearly 52% of particle size in the range 1.9–5.5 μm. In our limited experience with Menox, there were no occasions where the embolic agent precipitated within the vials prior to or after shaking. We did not observe any technical complications, such as microcatheter occlusion, due to rapid tantalum sedimentation. The embolization system contains three DMSO compatible syringes—two white pistons and one blue piston syringe. Based on our experience with other LEAs (Onyx, Squid, and PHIL), the syringes of Menox are slightly loose and clumsier. One practical disadvantage of the Menox syringes is the lack of catheter interface–adapter, which comes included in the Onyx, PHIL, and Squid embolization systems.18 19 As such, the operator has to use caution during the first injection, while adapting thumb pressure.
Overall, the treated lesions were visualized with the same radiodensity as those embolized with Onyx. The average estimated post-embolization volume reduction of the nidus in our study was 80%. Total occlusion in one endovascular session was achieved in more than a half of all treated patients. Similar results in terms of complete occlusion and the rate of adverse events were observed in studies conducted in patients treated with Onyx.5 20 21
From our perspective and previous clinical and technical experience with PHIL, there is no major difference between PHIL and Menox in terms of obliteration rates.22 It is important to emphasize that these observations are based only on personal opinion and do not represent statistically validated conclusions. In our experience, the risk of inadvertent embolization of potentially dangerous feeders or untoward extra-nidal or venous penetration between both LEAs is also equivalent. However, it is important to highlight that due to the tantalum nature of Menox, the beam hardening artifacts on post-procedure imaging were more pronounced compared with PHIL, limiting the adjacent brain parenchymal visualization of larger volume AVMs. Another drawback of Menox compared with PHIL is that PHIL is available in three different formulations and viscosities (25%, 30%, and 35%), while Menox is available only in a viscosity of 18 centistokes.23 Similar differences were noted in comparison with the other available EVOH based liquid embolic agent Squid. The 18 LD and 12 centistoke formulations and the 30% less tantalum in the Squid solution may increase and improve the visualization structures behind the dense embolic cast inside the treated AVM.
We gained our very first experience with Menox in the embolization of renal tumors, which were subsequently resected. As such, we also had the opportunity to observe the behavior of Menox during surgical manipulation. Similar to Onyx, Menox gives the sensation of spongy and pliable material. A sparkling effect of the embolic material in large vessels manipulated with the electrocautery device was observed. These properties of the embolic agent did not interfere with the surgical procedure.
In summary, in our experience, Menox behaves in a similar fashion to Onyx in terms of delivery during embolization. We found the required proximal plug formation and penetration comparable with the well known Onyx techniques. Menox can be delivered in a controlled fashion over a prolonged period of time with frequent pauses and with similar solidification time in between the injections, ultimately resulting in predicable, targeted, and satisfactory nidal obliteration. We did not observe an increased risk of inadvertent embolization, or untoward extra-nidal or venous penetration in comparison with other EVOH based LEAs. In our series, there were no major technical complications related to Menox injections.
Limitations
Despite being the largest clinical study of treatment of cerebral AVMs with Menox reported to date, our data have several important limitations. First, this was a single center study and the technical results are limited by authors’ individual techniques and experiences. Second, the sample was relatively small. Third, the presented data are permeated by selection bias, as the first four patients included in this cohort were selected on the basis of anatomical features and ease of catheterization. In addition, the authors gained their initial experience with Menox in peripheral embolization (renal tumors) and selected external carotid artery branches (dural AV fistulas) prior to using it for embolization of cerebral AVMs. As such, our study should be interpreted with caution as the results may not be widely applicable to general practice.
Conclusions
In our initial experience with endovascular embolization of cerebral AVMs, Menox had a similar technical profile and comparable clinical outcome with other well known EVOH based LEAs. Moreover, Menox appears to be a safe and promising option for endovascular treatment for cerebral AVMs and intracranial arteriovenous shunts. However, larger multicenter series are needed to confirm the clinical benefits of this new embolic system.
References
Footnotes
Contributors The main author interpreted the data, drafted the original manuscript version, reviewed all suggestions provided by all co-authors, approved the final version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The senior author provided major edits and assumed responsibility for final review and submission as a corresponding author. All co-authors provided substantial contribution to the interpretation of the provided data. All co-authors also contributed with revisions to the original draft, approved the final version of the manuscript, and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data related to this manuscript are available upon request.
Patient consent for publication Not required.