Article Text

Abstract
Background Mechanical thrombectomy (MT) is a safe and effective therapy for ischemic stroke. Nevertheless, very elderly patients aged ≥90 years were either excluded or under-represented in previous trials. It remains uncertain whether MT is warranted for this population or whether there should be an upper age limit.
Methods We retrospectively reviewed 79 patients with stroke aged ≥90 years from three neurointerventional centers who underwent MT between 2013 and 2017. Good functional outcome was defined as modified Rankin scale (mRS) ≤2 and assessed at 90-day follow-up. Successful recanalization was graded by Thrombolysis in Cerebral Infarction Scale (TICI) ≥2 b. Feasibility and safety assessments included unsuccessful recanalization attempts (TICI 0), time from groin puncture to recanalization, symptomatic intracranial hemorrhage (sICH), mortality, and intervention-related serious adverse events.
Results Only occlusions within the anterior circulation were included. Median time from groin puncture to recanalization was 39 min (IQR 25–57 min). The rate of successful recanalization (TICI ≥2 b) was 69.6% (55/79). Good functional outcome (mRS ≤2) at 90 days was observed in 16% (12/75) of patients. In-hospital mortality was 29.1% (23/79) and increased significantly at 90 days (46.7%, 35/75; p<0.001). sICH occurred in 5.1% (4/79) of patients. No independent predictor for good functional outcome (mRS ≤2) at 90 days was identified through logistic regression analysis.
Conclusion MT in nonagenarians leads to high mortality rates and less frequently good functional outcome compared with younger patient cohorts in previous large randomized trials. However, MT appears to be safe and beneficial for a certain number of very elderly patients and therefore should generally not be withheld from nonagenarians.
- intervention
- thrombectomy
- stroke
- thrombolysis
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy (MT) has become the standard of care for treatment of acute ischemic stroke (AIS) due to large vessel occlusions (LVO).1 2 However, most large randomized controlled stroke studies excluded patients older than 80 or 85 years of age. Those studies without an upper age limit enrolled only a small number of octogenarians, and even fewer nonagenarians (table 1). Although advanced age is not considered a contraindication for MT, no substantial therapy recommendations for patients aged 90+ have been derived from the latest thrombectomy landmark trials.3 4 Data on patients aged 90+ undergoing MT for AIS are limited and inconsistent, and the outcomes and safety of MT in the very elderly have not been investigated rigorously. As demographics are changing and the number of very elderly subjects is expected to increase, the incidence of stroke will likely increase too.5 Therefore, we require selection criteria, therapeutic options, and treatment strategies for this particular subgroup of patients to manage this anticipated challenge in stroke care effectively.
Age as inclusion criterion in past mechanical thrombectomy landmark studies1
The objective of this study is to report on the feasibility, effectiveness, and safety of MT in very elderly patients aged 90+ treated at three high-volume stroke centers.
Methods
Patient selection
We prospectively analyzed patient data collected between 2013 and 2017 from three large German neurointerventional centers: Hospital Bremen-Mitte, University Medical-Center Hamburg-Eppendorf, and University Hospital of Cologne. The study was approved by the local ethics committees (Chamber of Physicians, Hamburg/Bremen, Germany) and no informed consent was required. Patient inclusion criteria were defined as: (1) endovascular treatment for AIS due to LVO, with or without additional intravenous thrombolysis (IVT); (2) LVO within the anterior circulation; and (3) patient age ≥90 years on the date of intervention. Patients with a baseline pre-stroke modified Rankin Scale (mRS) score ≥3 were excluded from the analysis.
Diagnostic and interventional procedure
Imaging studies (CT, CT angiography or, in some cases, CT perfusion) were performed on admission to exclude patients with intracranial hemorrhage (ICH) and to detect arterial occlusions. Experienced neurologists performed all neurological evaluations. The National Institutes of Health Stroke Scale (NIHSS) was applied on admission and the mRS at discharge and at 90-day follow-up. All patients were treated with modern thrombectomy devices. Depending on commercial availability and institutional preference, different stent retriever and aspiration catheter models were used. There was no limitation for devices, thus stent retriever and aspiration catheters were used either in combination or alone.
Study endpoints
The main neurological endpoint was the rate of functional independence (defined as mRS ≤2) at 90-day follow-up. The mRS score at 90 days was not available in four patients due to drop-out from the follow-up program at that time; these cases were excluded from the functional outcome analysis. The angiographic endpoint was successful recanalization (TICI ≥2b) of the occluded target vessel as determined by post-interventional digital subtraction angiography. Other endpoints for procedural feasibility and safety included rate of unsuccessful recanalization with failed arterial groin access or unsuccessful catheter navigation to the occlusion site (both classified as TICI 0), time from groin puncture to recanalization (indicating complexity of the intervention), and rate of intervention-related serious adverse events (SAEs) such as iatrogenic dissection, new distal embolization, or occurrence of post-interventional symptomatic intracranial hemorrhage (sICH). sICH was defined according to ECASS II as evidence of intracranial hemorrhage and a minimum increase of 4 NIHSS points within 24 hours after treatment in relation to the initial NIHSS score on hospital admission.6 All-cause mortality rates were assessed and compared during hospital stay and at 90-day follow-up.
Statistical analysis
Standard descriptive statistics were employed for all study endpoints. For comparison of categorical variables, Fisher’s exact test was used. The Mann–Whitney U test (non-normally distributed data) and the unpaired Student’s t-test (normally distributed data) were used to compare continuous variables. The McNemar test was used for comparing categorical outcome follow-up data. Univariable regression was followed by stepwise forward multivariable regression analysis to determine independent predictors for good clinical outcomes at 90 days follow-up. Results are presented as odds ratios (ORs) with 95% CI. The significance level was set at α=0.05. All statistical analyses were carried out using SPSS Version 22 (SPSS, Chicago, Illinois, USA).
Results
Study population
Seventy-nine patients met the inclusion criteria and were treated between 2013 and 2017. The median age was 92 years (IQR 90–93) and 79.7% (63/79) were women. Patients were admitted to hospital with a median NIHSS score of 17 (IQR 13–21) and the median baseline ASPECTS was 9 (IQR 8–10). A CT scan was used to select patients for MT in 93.7% of cases (74/79). The most common cardiovascular risk factors were arterial hypertension (83.5%, 66/79) and atrial fibrillation (63.3%, 50/79). Most occlusions (69.6%, 55/79) involved the M1 segment of the middle cerebral artery (MCA); other locations within the anterior circulation included the terminal carotid artery (21.5%, 17/79), the MCA M2 segment (7.6%, 6/79), and the MCA M3 segment (1.3%, 1/79). Almost 60% (47/79) of patients received IVT prior to MT. The most frequently used thrombectomy device was a stent retriever (74.7%, 59/79). Comparison of baseline characteristics on admission showed no significant differences between favorable (mRS ≤2) and unfavorable (mRS >2) outcomes at 90 days (table 2).
Overview of patients’ baseline characteristics and procedural outcomes
Functional and procedural outcomes
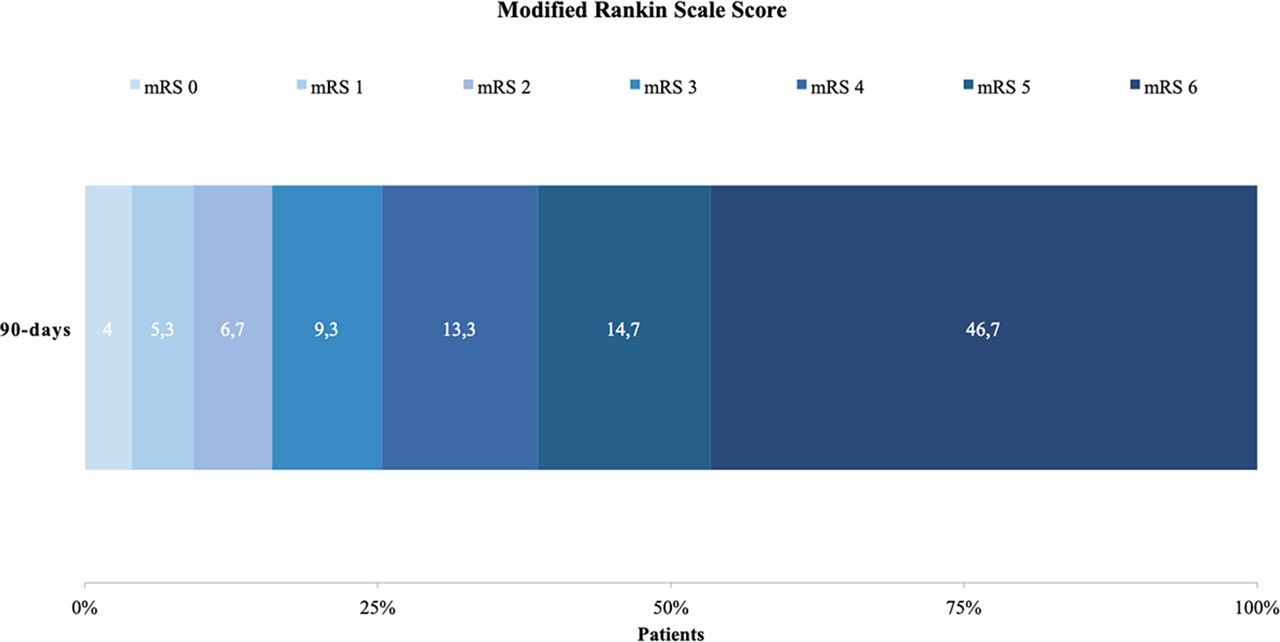
Favorable clinical outcomes (mRS ≤2) were observed in 16% (12/75) of patients at 90-day follow-up. Figure 1 provides an overview of mRS distribution at 90-day follow-up. In univariable as well as multivariable logistic regression analysis, no independent predictors of good functional outcome (mRS ≤2) at 90 days were identified (Table 3 and Table 4). Post-interventional in-hospital mortality was 30.7% (23/75), which increased to 46.7% (35/75; p<0.001) at 90 days. The overall rate of sICH was 5.1% (4/79).
Univariable analysis for good functional outcome (mRS <2) at 90 days
Multivariable analysis for good functional outcome (mRS <2) at 90 days
{kind=link}
Distribution of modified Rankin Scale at 90-day follow-up.
Unsuccessful recanalization attempts (TICI 0) were reported in 21.5% (17/79) of cases, including two failures of femoral groin access. No case underwent radial or carotid puncture as a rescue approach. Most interventionalists reported these cases as challenging because of complicated arterial access or elongated vessels rendering catheter navigation or retrieval maneuvers impossible. In 44.3% (35/79) of the cases MT was performed under general anesthesia. Successful angiographic recanalization (TICI ≥2 b) was achieved in 69.6% (55/79) of patients. The median time from groin puncture to recanalization was 39 min (IQR 25–57 min), and a median of 1 (IQR 1–2) passes was needed for the final MT result. There were two reports on periprocedural SAEs, both documented as iatrogenic dissections resulting in small subarachnoid hemorrhages that did not cause clinical symptoms. Comparison of main procedural outcome results between favorable (mRS ≤2) and unfavorable (mRS >2) outcomes at 90 days did not reveal any significant differences.
Discussion
MT is considered superior to IVT alone in octogenarians. Most studies showed that older stroke patients are more likely to experience a poor clinical outcome than younger patients.7–10 Only a few reports of MT in nonagenarians are available, most of which are small single-center case series with inconsistent conclusions.9 Although data from the HERMES meta-analysis suggested a significant beneficial effect of MT in patients aged ≥80, the number of enrolled patients aged ≥90 years was very limited.11
Three-quarters (79.7%, 63/79) of all patients in this study were women. This coincides with the fact that women generally have a higher life expectancy than men and thus a higher chance of suffering from stroke in old age.12 Previous studies on endovascular stroke therapy emphasized advanced age as a strong predictor of unfavorable outcome after MT.13 14 Hence, lower rates of good functional outcomes are expected in very elderly populations.
In this study a good functional outcome (mRS ≤2) was achieved in 16% (12/75) of patients at 90-day follow-up. Similar to our results, Möhlenbruch et al reported good functional outcomes (mRS ≤2) in 5 of 29 (17.2%) patients aged 90+ at 90 days.15 Rates of good favorable outcome in previous representative thrombectomy trials ranged from approximately 30% to 70%.11 Good functional outcomes in octogenarians were reported in 20–35% of patients.16–18 According to the published data, the rate of good functional outcome after thrombectomy appears to decline with advancing age.
Common independent predictors for good functional outcome, such as low NIHSS scores on admission, have been described in MT studies.19 We did not identify any predictors for good functional outcome at 90 days, which suggests that these predictors may not be applicable for very elderly patients. Another important predictor for good functional outcome after MT is successful recanalization (TICI ≥2 b).20 To date, reports on recanalization rates have been inconsistent, ranging from no association with age to lower rates of recanalization in the elderly.13 21 22 Recanalization was successful (TICI ≥2 b) in 55 of 79 cases (69.6%) in this study compared with rates of up to 90% reported in large randomized trials.23 The lower rate our cohort is most likely due to the relatively high number (17/79, 21.5%) of unsuccessful recanalization attempts (TICI 0) because of increased vessel tortuosity which complicated arterial access and intracranial navigation. Data regarding unsuccessful recanalization were not systematically collected in this study; therefore, this finding should be interpreted with some caution. Vessel tortuosity, however, is a well-described technical problem in endovascular therapy with an increased prevalence in elderly patients.7 9 24
Similar to other studies focusing on older patients, we observed a high rate of in-hospital mortality (30.7%, 23/75); overall mortality significantly increased at 90-day follow-up (46.7%, 35/75; p<0.001). Tonetti et al and Khan et al reported even higher mortality rates of 70% (21/30) and 60% (11/18) at 90 days in their case series.9 25 These findings emphasize the fact that very elderly patients have a higher incidence of comorbidities and a higher risk for developing complications such as pneumonia during and after hospitalization, presumably leading to increased mortality and disability rate after thrombectomy.26 27 Comparison with the results of the HERMES meta-analysis (n=633) with an overall mortality rate of 15.3% at 90 days, the development of mortality rates in very elderly patients seems to be unique and in some way independent of the stroke event and MT result.11 Consequently, the time from discharge to 90-day follow-up, including neurorehabilitation, seems to be a critical time period for this subgroup compared with younger patients. Very elderly patients appear to be at continued risk of death, disability, and functional dependency regardless of early clinical outcomes after MT.
Previous studies have reported higher rates of sICH in elderly patients while others failed to detect an age-related risk.10 13 17 Our results were comparably low (incidence of 5.1%, 4/79) compared with recent thrombectomy trials. Rates of other intervention-related SAEs including iatrogenic dissection were comparable to previous randomized studies.23
Our study has certain limitations inherent to retrospective study designs. Nevertheless, the strength of this study is its relatively large sample size for this specific clinical subgroup and the multicenter approach, representing the first study of its kind.
Conclusion
MT in nonagenarians is a technically challenging procedure but can be considered as feasible and comparatively safe. Pre-existing comorbidities, as well as hospitalization and rehabilitation, represent risk factors potentially leading to poor clinical outcomes and death regardless of the initial MT result. Thus, high mortality rates should be expected at 90-day follow-up. However, non-interventional therapies, including IVT, are no effective alternatives for LVOs. This study demonstrates that nonagenarians can benefit from MT. Therefore, excluding this age group from MT per se seems unjustified. Instead, patients should be evaluated on a case-by-case basis, with specific consideration of the patient’s baseline medical condition and the severity of the stroke.
References
Footnotes
Contributors LM, MA, and PP made substantial contributions to the conception and design of the work. Data acquisition was performed by LM, AM, HL, FF, VM, NA, and MD-C. LM and PP performed the data analysis. Interpretation of the data was done by LM, JF, GT, AM, CR, AK, MP and PP. LM and PP drafted the manuscript and all of the other authors revised it critically for important intellectual content. All authors approved the final version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PP: Consultant for Penumbra. JF: Consultant for Acandis, Boehringer Ingelheim, Codman, Microvention, Sequent, Stryker. Speaker for Bayer Healthcare, Bracco, Covidien/ev3, Penumbra, Philips, Siemens. Grants from Bundesministeriums für Wirtschaft und Energie (BMWi), Bundesministerium für. Bildung und Forschung (BMBF), Deutsche Forschungsgemeinschaft (DFG), European Union (EU), Covidien, Stryker (THRILL study), Microvention (ERASER study), Philips. GT: Received personal fees as consultant/lecturer from Acandis, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Daichi Sankyo, Stryker, and research grants from Bayer, Federal Ministry for Economic Affairs and Energy (BMWi), Corona-Foundation, German Research Foundation (DFG), Else Kröner-Fresenius Foundation, European Union (Horizon 2020), German Innovation Fund. AM: Consultant for Stryker, Penumbra, Perflow, Phenix. All other authors declared no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.