Article Text

Abstract
Background Direct carotid–cavernous sinus fistulas (dCCFs) are high flow arteriovenous shunts between the internal carotid artery and the cavernous sinus. Recently, we have used the pipeline embolization device (PED) to treat dCCFs.
Methods We describe our experience treating patients with dCCFs in whom the PED was placed as the primary treatment modality.
Results Five patients with dCCFs were treated with PEDs deployed in the ipsilateral internal carotid artery spanning the fistula. All patients also underwent either adjunctive transvenous or transarterial embolization. The PED served both as the primary treatment modality and as a scaffold that facilitated safe and efficacious transvenous embolysate administration by altering the flow dynamics through the fistula and providing a physical barrier that protected the internal carotid artery. No intraoperative or perioperative complications occurred. One of the five patients exhibited complete angiographic resolution of the fistula immediately after the procedure. The remaining four patients experienced complete obliteration of the fistula without additional treatment, which suggests that the PED induced alteration promoted thrombosis of the fistula. Therefore, 100% of patients in this series exhibited complete and durable obliteration of the fistula and complete resolution of symptoms following treatment.
Conclusions We believe that use of the PED to treat dCCFs may be a safe and efficacious strategy that facilitates parent vessel protection during transvenous embolization. Furthermore, the flow alterations induced by the PED may promote thrombosis of incompletely occluded fistulas. This is the largest reported series of non-iatrogenic dCCFs treated with use of the PED as the primary initial treatment strategy.
- arteriovenous fistula
- direct carotid-cavernous fistulas (dCCFs)
- flow diversion
- flow-diverting devices
- flow-diverting stent
- Onyx
- pipeline embolization device (PED)
- scaffold
- transvenous embolization
Statistics from Altmetric.com
- arteriovenous fistula
- direct carotid-cavernous fistulas (dCCFs)
- flow diversion
- flow-diverting devices
- flow-diverting stent
- Onyx
- pipeline embolization device (PED)
- scaffold
- transvenous embolization
Introduction
Direct carotid–cavernous sinus fistulas (dCCFs) are high flow arteriovenous shunts secondary to a direct connection between the internal carotid artery (ICA) and the cavernous sinus. These lesions most frequently develop following trauma but can also arise spontaneously or secondary to a ruptured cavernous carotid artery aneurysm. Ideal treatment of a dCCF is complete occlusion of the arteriovenous shunt while maintaining patency of the ICA. Traditionally, endovascular treatment options for dCCFs involve detachable balloons1 2 or coils3 4 through a transarterial, transvenous, or combined approach. The use of liquid embolic agents, including n-butyl-2-cyanoacrylate (nBCA) and Onyx, has also been reported,5–7 and a recent study has demonstrated improved radiographic outcomes when a liquid embolysate is used in conjunction with detachable coils compared with coils alone.8
Here we describe our recent experience using the pipeline embolization flow diverting device (PED) as the upfront treatment modality to achieve safe and effective occlusion of dCCFs. This is the largest reported consecutive series of non-iatrogenic dCCFs treated with the PED as a primary initial treatment strategy.
Methods
We retrospectively reviewed the prospectively maintained clinical database at our institution to identify a consecutive series of patients who presented with a diagnosis of dCCF to our institution between July 1, 2012, and September 30, 2016. We excluded all patients who presented with an indirect CCF; there were no cases of iatrogenic dCCF or retreatment for a previously incompletely obliterated dCCF during this period. Clinical, radiological, procedural, and follow-up data for patients with dCCFs were extracted after a review of outpatient clinic and inpatient hospital medical records, operative notes, radiologic reports, and cerebral angiograms.
Embolization procedure
All patients who received a diagnosis of dCCF during the inclusion period were evaluated for curative endovascular treatment. The treatment strategy for all of these patients involved endovascular intervention with use of the PED with adjunctive transvenous or transarterial embolization. All treatment procedures were performed under general anesthesia with intraoperative electrophysiological neuromonitoring. All patients were heparinized during the procedure and received aspirin and clopidogrel bisulfate before treatment. In all cases, one or more PEDs were deployed in the ipsilateral ICA spanning the fistulous site. Adjunctive transvenous or transarterial treatments were then performed on the basis of the clinical judgment of the surgeon.
Results
Patient presentation
Five consecutive patients met the inclusion criteria and were analyzed. The series included three men and two women; median age was 47 years (range 14–75 years). Three patients presented following an identifiable head trauma; two patients presented with spontaneous symptom onset, one of whom had a known cavernous carotid aneurysm. One teenage patient presented acutely following a severe trauma with a score of 8 on the Glasgow Coma Scale, which significantly limited preoperative clinical evaluation. Of the remaining four patients, all presented with ipsilateral chemosis and proptosis; three presented with vision impairment including an ipsilateral abducens palsy; and one presented with ipsilateral V1 bdistribution numbness.
Endovascular embolization
All five patients underwent endovascular intervention that involved deployment of either a single PED or two overlapping PEDs (mean PEDs used per case=1.4) in the ipsilateral ICA spanning the fistula. Additional transvenous embolization was performed in four patients. Of these four patients, one patient was treated using transvenous coil embolization during the same endovascular procedure as the PED deployment. Two patients underwent transvenous embolization during the same endovascular procedure as the PED deployment as well as an additional transvenous Onyx embolization in a delayed fashion (1–3 days later). One patient underwent two subsequent transvenous embolization procedures using detachable coils and nBCA at 3 and 5 days after PED deployment. Adjunctive transarterial coil embolization was performed in one patient during the same procedure as PED deployment after jailing a coiling catheter.
For the four patients who underwent adjunctive transvenous treatment, the PED functioned as both a primary treatment device and a scaffold that facilitated safe and efficacious use of transvenous coiling and Onyx or nBCA administration by both altering the flow dynamics through the fistula and protecting the parent ICA. Indeed, a transarterial balloon was used for additional parent vessel protection during transvenous treatment in only two of these patients, and no arterial balloon protection was used for the nBCA treatment. No intraoperative or perioperative complications occurred.
Clinical and radiographic outcomes and follow-up
One of the five patients exhibited complete angiographic resolution of the fistula immediately following treatment. Interestingly, the four patients with incomplete obliteration of the fistula at the time of treatment were found to have complete resolution of the fistula on follow-up angiograms without additional treatment, which suggests that the PED induced alteration in flow may have contributed to thrombosis of the fistula. Therefore, 100% of patients in this series had complete obliteration of the fistula following treatment. Longitudinal follow-up data are available for four of these patients. On the last angiographic follow-up (median 24 months; range 2–55 months), 4/4 patients (100%) had continued complete obliteration of the fistula. All patients experienced complete resolution of symptoms following treatment.
Clinical vignettes
Patient clinical, treatment, and outcome data are summarized in table 1. Two illustrative cases are presented in detail below.
Summary of patient clinical, treatment, and outcome data
Patient No 1
A middle aged patient presented with right eye proptosis and chemosis. Six months before this presentation, the patient had been hospitalized with a temporal bone fracture and traumatic subarachnoid hemorrhage following an assault. MRI of the brain had findings concerning for a right dCCF with right superior ophthalmic vein and cavernous sinus varices. Cerebral angiography demonstrated a right dCCF with drainage via the right superior ophthalmic vein and right inferior petrosal sinus (figure 1). Decreased flow in the ipsilateral middle cerebral artery and anterior cerebral artery was also noted. We deployed a PED across the fistulous site in the right ICA. A second PED was also deployed in a telescoping fashion across the proximal end of the fistulous site to provide double coverage. After deployment of the PEDs, there was marked improvement in ipsilateral middle cerebral artery and anterior cerebral artery flow as well as significant flow stagnation within the cavernous sinus and decreased shunting. We then performed transvenous coiling of the inferior ophthalmic vein and cavernous sinus. Angiography demonstrated complete obliteration of the fistula with no residual shunting. At discharge from the hospital, the patient reported resolution of their symptoms. The patient was lost to angiographic follow-up but reported durable resolution of their symptoms at 1 year after the procedure. The patient received dual antiplatelet therapy (DAPT) for 6 months after treatment.
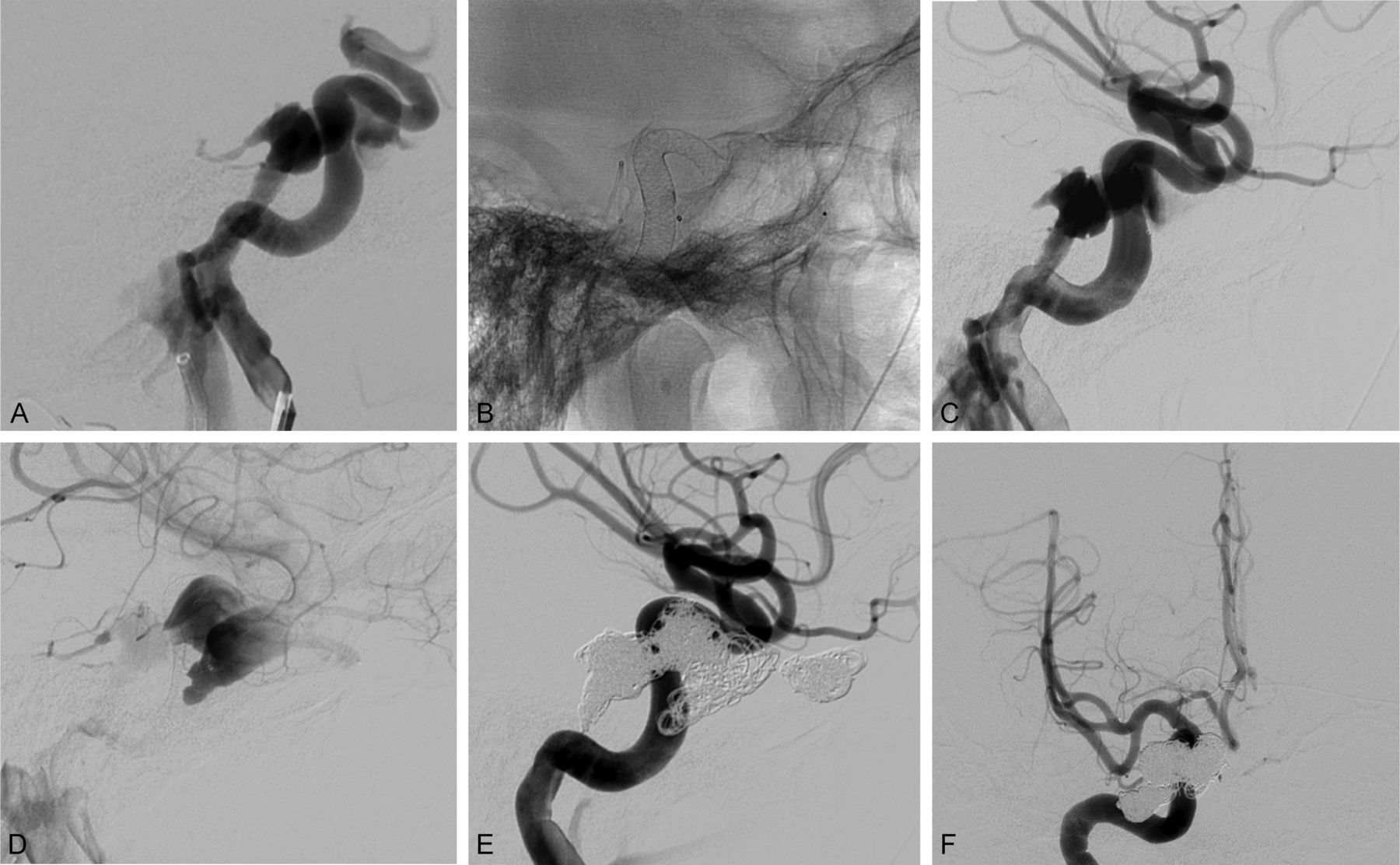
Angiograms showing (A) right direct carotid–cavernous sinus fistula (dCCF), (B) placement of the pipeline embolization device (PED) across the fistulous site, (C) decreased shunting across the fistula and increased ipsilateral middle cerebral artery and anterior cerebral artery flow after PED deployment, (D) stagnation of flow within the cavernous sinus after PED deployment, and (E, F) complete obliteration of the dCCF with restoration of normal intracranial circulation following PED deployment and transvenous coiling. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Patient No 2
A middle aged patient with a known left cavernous ICA aneurysm diagnosed 8 years earlier presented with a 2 week history of headaches, nausea with vomiting, impaired vision, and left-sided facial numbness. Physical examination demonstrated a left sixth nerve palsy and V1 distribution numbness. Non-invasive imaging suggested a dCCF. Cerebral angiography demonstrated a large left cavernous ICA aneurysm causing a dCCF with drainage via the left superior ophthalmic vein, left inferior ophthalmic vein, left superior petrosal sinus, and bilateral inferior petrosal sinus (figure 2). After positioning a coiling catheter within the aneurysm, we deployed a PED across the fistulous site in the left ICA, jailing the coiling catheter. After deployment of the PED, there was marked improvement in ipsilateral middle cerebral artery and anterior cerebral artery flow as well as decreased but persistent shunting across the dCCF. We then coiled the aneurysm via the jailed catheter. Post-treatment angiography demonstrated further decreased shunting with marked stagnation of flow within the cavernous sinus. Because of the significant decrease in flow across the fistula, the decision was made to not pursue further treatment during this procedure, and the patient was extubated and transferred to the intensive care unit.

{kind=link}
{kind=link}
Angiograms showing (A) left direct carotid–cavernous sinus fistula (dCCF), (B) placement of the pipeline embolization device (PED) across the fistulous site, (C) decreased shunting across the fistula after PED deployment, (D, E) subtotal obliteration of the dCCF on postoperative day 1 following PED deployment and transvenous coiling, and (F) complete obliteration of the dCCF and restoration of normal intracranial circulation at the 6 month follow-up after PED deployment and transvenous coiling. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
The following day, the patient reported improvement of their symptoms. Angiography revealed additional thrombosis of the fistula with only trace arteriovenous shunting. The patient was discharged from the hospital on DAPT and returned for a follow-up angiogram 6 months after treatment. At the 6 month follow-up appointment, the patient reported complete resolution of their symptoms. Angiography revealed complete obliteration of the aneurysm and fistula with no residual shunting. Treatment with clopidogrel bisulfate was discontinued, and therapy with aspirin was maintained.
Discussion
Advances in endovascular technology and techniques in recent decades have led to a significant evolution in the treatment algorithm for dCCFs.9 10 The development of flow diverting devices, including the PED, has provided another option for treating these challenging lesions. The flow diverting properties of the PED and other flow diverter stents make these devices potentially attractive for the treatment of patients with high flow shunts. The well established goals of treatment of a dCCF are to occlude the arteriovenous shunt while preserving ICA patency. The PED, by promoting laminar flow through the parent artery, can simultaneously divert blood away from the shunt and serve as a scaffold that provides a physical and hemodynamic barrier that prevents herniation or migration of transvenously or transarterially deployed embolic material. Indeed, in our series, the PED independently decreased the shunting across the fistula in all five patients, which resulted in stasis within the cavernous sinus and promoted normalization of distal arterial flow. Furthermore, in two of the four patients who underwent adjunctive transvenous treatment, the PED was the only arterial protection device used, and an arterial balloon was not required, even in a case in which a liquid embolic agent was injected on the venous side of the shunt. We encountered no thromboembolic complications or off target embolization in our series.
This article describes our recent experience using the PED as an upfront, primary treatment modality to achieve safe and effective occlusion of dCCFs. This is the largest reported consecutive series of non-iatrogenic dCCFs treated with the PED as the primary initial treatment strategy. There have been other reports in the literature describing the use of flow diverting devices for the treatment of dCCFs; however, these have largely been case reports in which the PED was used as a salvage technique for intraprocedural iatrogenic injury or as an adjunctive treatment strategy for residual or recurrent fistulas after unsuccessful primary treatment of the dCCF.11–17 These studies are summarized in table 2.11–17
Summary of previously reported cases with use of flow diverting devices for the treatment of a direct carotid–cavernous sinus fistula
Our results suggest that using flow diverting stents as a treatment for dCCF is likely to be safe and effective. All patients in our series achieved complete obliteration of the fistula, had no thrombotic or periprocedural complications, and experienced complete, durable resolution of their symptoms. We believe that the strategy of upfront flow diverting device placement is appealing for multiple reasons.
First, the reconstructive nature of PED treatment, as opposed to destructive strategies, may reduce the need for extensive coil or embolysate mass packing within the aneurysm sac or cavernous sinus, and thus minimize the mass effect that may contribute to secondary cranial nerve compression. Indeed, Bink et al 3 found that 44% of patients treated with coil embolization alone had persistent cranial nerve symptoms despite complete eradication of the fistula and that the persistence of symptoms correlated with coil mass volume. All patients in our series achieved complete and durable resolution of their presenting cranial neuropathy.
Second, the PED serves as a scaffold that protects the ICA by providing a physical and hemodynamic barrier that decreases the risk of coil or liquid embolysate protrusion into the arterial system. This may promote a more effective and focused venous embolization directly at the fistulous site that could increase treatment efficacy while limiting the risk of off target treatment or excessive coil mass placement (as discussed above). None of our patients experienced migration of embolysate into the ICA, off target deposition of liquid embolysate, or thrombotic complications. Therefore, the use of flow diverting devices may enhance the safety of transvenous delivery of liquid embolic agents, which has been reported to independently increase the rate of dCCF cure.8 Furthermore, temporary inflation of an arterial balloon was used for additional ICA protection during transvenous treatments in only two patients. Therefore, using only the protection provided by the PED scaffold, we eliminated the risk of ischemia attributable to temporary balloon occlusion while still protecting against impairment of ICA patency by the transvenous embolysates. In fact, for patients with impaired ipsilateral middle cerebral artery and ICA flow associated with dCCF shunting, the use of the PED resulted in immediate flow restoration, further protecting against intraoperative ischemia.
Third, the flow diverting properties of the PED likely promote thrombosis over time. While all of our patients demonstrated marked improvement in shunting following PED treatment, only one of the five patients exhibited complete angiographic cure of the fistula immediately following initial treatment. Interestingly, the four patients with incomplete obliteration of the fistula immediately following treatment were found to have complete resolution of the fistula on follow-up angiograms without any additional treatment, which suggests that the PED induced alteration in flow contributed to thrombosis of the fistula. We believe that the PED construct provides an excellent scaffold for robust endothelialization, resulting in a complete and durable obliteration. As we found in our series, as this thrombosis occurs, the flow through the fistula decreases, which leads to decreased cavernous sinus pressures and resolution of compressive symptoms.
One significant limitation of the use of PEDs to treat dCCFs in patients with acute presentation following a trauma is the requirement for DAPT. In our practice, we typically discontinue clopidogrel bisulfate therapy at 6 months and maintain an aspirin only regimen if there is no evidence of in-stent stenosis or thrombotic complications on follow-up imaging. However, during the acute period following a significant trauma, DAPT can pose considerable difficulty if the patient has other injuries or needs to undergo other surgical procedures. This is analogous to the situation encountered when considering PED placement or stent coiling of a ruptured intracranial aneurysm. The precise management of DAPT in the acute trauma setting is challenging, and decisions should be made on a case by case basis. As with any decision, the risk and benefits of any treatment strategy must be evaluated for each individual patient. In general, we would advocate for either delayed PED treatment or a staged treatment strategy during which the initial procedure would involve targeted transvenous and/or transarterial embolization of any potential high risk features (eg, a pseudoaneurysm or cortical venous reflux) using coils with or without balloon protection. This would be followed by a definitive treatment procedure utilizing the PED once it was deemed appropriate for the patient to begin DAPT. In practice, as in our series, patients with post-traumatic dCCF often present in a delayed fashion, therefore reducing the risk associated with initiation of DAPT.
While we believe that flow diversion is useful in the treatment of dCCFs, we do not advocate for its use as the sole, standalone treatment for high flow dCCFs. Just as the PED appears to preserve the patency of arterial branches of the ICA, the pressure gradient created by a high flow dCCF likely will continue to siphon arterial flow and maintain shunt patency, resulting in inadequate treatment. This was demonstrated in our series in which PED placement decreased but did not eliminate flow through the shunt. Furthermore, even if the PED did subsequently decrease flow through the shunt and ultimately achieve a cure, the significant delay between the initial treatment and eventual neointima formation would subject the patient to potential risk during this latency period. Therefore, we advocate a combined treatment strategy that involves upfront placement of a PED to promote normalization of arterial flow while providing a scaffold that serves as a protective physical and hemodynamic barrier for the ICA followed by transvenous and/or transarterial treatment with coils and/or liquid embolysates in the same session to achieve a cure.
Conclusions
We believe that the upfront use of the PED for the treatment of dCCFs may represent a safe and efficacious strategy for treatment of these lesions that facilitates parent vessel protection during transvenous coiling and/or liquid embolysate infusion. Furthermore, the flow alterations induced by the PED may promote thrombosis of incompletely occluded fistulas. Caution must be exercised in the setting of multisystem traumatic injuries because of the need for a DAPT.
Acknowledgments
The authors thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
References
Footnotes
Contributors Primary writing of the text, manuscript preparation, data collection, and interpretation and approval of the text: JFB, AD, and FCA. Assistance with manuscript preparation and critical revision, data collection and interpretation, and approval of the text: CJP, ROA, DD, JSC, SB, VLF, and DDC. Project design: JFB, AD, and FCA. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: JFB, AD, CJP, ROA, DD, JSC, SB, VLF, DDC, and FCA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests AD: Consulting agreement with Medtronic (pipeline embolization device certification proctor).
Ethics approval Institutional review board approval was obtained for this project (PHX-18-500-335-73-12).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data to share.
Correction notice Since this article was first published online, the initial F has been added to Dr Ducruet’s name.
Patient consent for publication Not required.