Article Text

Abstract
Objectives To characterize the safety and efficacy of large woven stents in the treatment of vertebrobasilar dolichoectasia (VBD).
Methods We retrospectively reviewed 19 consecutive patients with VBD treated with large woven intracranial stent (Leo stents) between January 2016 and December 2018. The clinical symptoms and angiograms of all the patients were recorded.
Results The patients were treated with 1–3 large Leo stents (5.5 mm x 75 mm, 5.5 mm x 50 mm, or 4.5 mm x 40 mm), with or without coiling. They had follow-up angiography and MRI between 3 months and 1 year. Digital subtraction angiography showed 16 patients with complete reconstruction of the target vessels, one patient with almost complete reconstruction, and two patients with partial reconstruction. All patients had symptomatic improvement shortly after treatment, but two patients developed recurrent dysphagia at 8 and 18 months, respectively.
Conclusions Deployment of woven stents with or without supportive coiling may offer symptom relief and reconstruction in patients with VBD.
- aneurysm
- angiography
- embolic
- stent
- intervention
Statistics from Altmetric.com
Introduction
Symptomatic vertebrobasilar dolichoectasia (VBD) is an uncommon disease with high morbidity and mortality. Some reports suggested a mortality of up to 43%.1–3 VBD can result in unfavorable outcome by several mechanisms.1 The tortuous, elongated, and ectatic vertebral and basilar arteries can directly compress the brainstem. Turbulence and stasis in VBD can lead to thrombosis and ischemic symptoms. Weakened vessel walls may rupture, causing intracranial hemorrhage.
There have been reports advocating antiplatelet therapy or anticoagulation to treat the ischemic symptoms. Because the mechanisms of ischemic symptoms are variable, including arteriosclerosis, turbulent flow, and stasis, antiplatelet and anticoagulant treatment is not always effective to prevent the progression of ischemia but may increase the risk of hemorrhage.4
Some authors have suggested surgical occlusion of vertebral arteries combined with bypass, but the ectatic basilar artery could still grow and compress the adjacent brainstem and cranial nerves even when both the vertebral arteries are occluded.5
Although aggressive treatment has been advocated for this disease, the existing treatments using flow- diversion stent or stent-assisted coiling are not very effective and carry a high risk of complications.1 A series of patients with VBD treated with flow diversion showed a high mortality of 57.1% and an overall infarct rate of 71.4%.6 Lower complication rates of 38.4–44.4% have been reported using laser-cut stents, but good outcomes ranged only from 55.56–69.23%.7 8
Large woven stents have pore sizes between those of laser-cut stents and flow-diversion stents. When placed in an overlapping or telescoping fashion, they can have some degree of flow diversion, allowing for slow thrombosis and healing of VBD, reducing the risks of occlusion of perforators. They are easier to deploy than flow-diversion devices and can be precisely placed to cover the entire lesion. We thus treated 19 consecutive patients with VBD with large woven stents between January 2016 and December 2018. We hereby report the safety and efficacy of this treatment and compare the results with previously published results.
Materials and methods
We retrospectively reviewed 19 consecutive patients with VBD treated with large self-expanding woven intracranial stents (Leo stents, Balt, Montmorency France) in our department between January 2016 and December 2018. VBD was identified by CT angiography (CTA) or MR angiography (MRA) and confirmed by DSA. The unproven nature of the treatment technique and alternative treatment methods were discussed with the patients and their families before treatment. All patients agreed to the treatment plan and signed the informed consent forms.
Assessment of VBD
We used the following CTA criteria to define VBD according to Smokers et al 9 ,1bifurcation of the basilar artery higher than the saddle pool or located beside the perimedian region, and a diameter of the basilar artery ≧4.5 mm. We adopted the following semiquantitative MRA standard as reported by Ubogu et al 10 ,2: length of the basilar artery >29.5 mm, and >10 mm lateral shift from the vertical line between the initial point and bifurcation of the basilar artery; length of the intracranial vertebral artery >23.5 mm and >10 mm shift of either vertebral artery from the line between the initial point of the intracranial vertebral artery and the initial point of the basilar artery. Patients meeting either CTA or MRA criteria were diagnosed as VBD.
Clinical manifestation
Eight patients had brainstem compression symptoms, such as dysphagia, choking, quadriplegia, or hemiparesis. Six patients had brainstem infarctions. Three patients had cerebellar infarction. One patient had trigeminal neuralgia and another patient had brainstem hemorrhage.
Endovascular technique
All patients received dual antiplatelet therapy of daily 100 mg aspirin and 75 mg clopidogrel for at least 5 days before the treatment. The postprocedural antiplatelet regimen consisted of daily aspirin for 3 months and clopidogrel for life.
For patients with brainstem hemorrhage or acute ischemia, the endovascular treatment was performed at least 2 weeks after the onset of symptoms. For patients with chronic or progressive symptoms, the treatment was carried out urgently after dual antiplatelet therapy for 5 days.
The primary strategy was to place a Leo stent across the entire segment of the dolichoectatic vertebrobasilar artery. According to the lesion length, a Leo stent of 5.5 mm x 75 mm, 5.5 mm x 50 mm or 4.5 mm x 40 mm (Balt, Montmorency, France) was deployed to cover the distal end of the lesion. After the stent was released, the microcatheter was tracked into the basilar artery again along the stent delivery wire. If one stent was not long enough, a second Leo stent was telescoped into the first stent to bridge the entire lesion (figures 1 and 2). In this situation, efforts were made to match the overlapping portion of the stent with the most severely ectatic segment. When additional radial force was needed to improve wall apposition, a self-expanding stent was placed inside the woven stent. When wall apposition was not satisfactory due to curvature of the vessel, or focal fusiform dilatation, up to four large and long coils were placed outside the stent to provide buttressing on the ventral side, so that the stent would touch the dorsal side of the basilar artery, where perforators could originate. The coils were not intended to occlude the lumen outside the stent (figure 1).
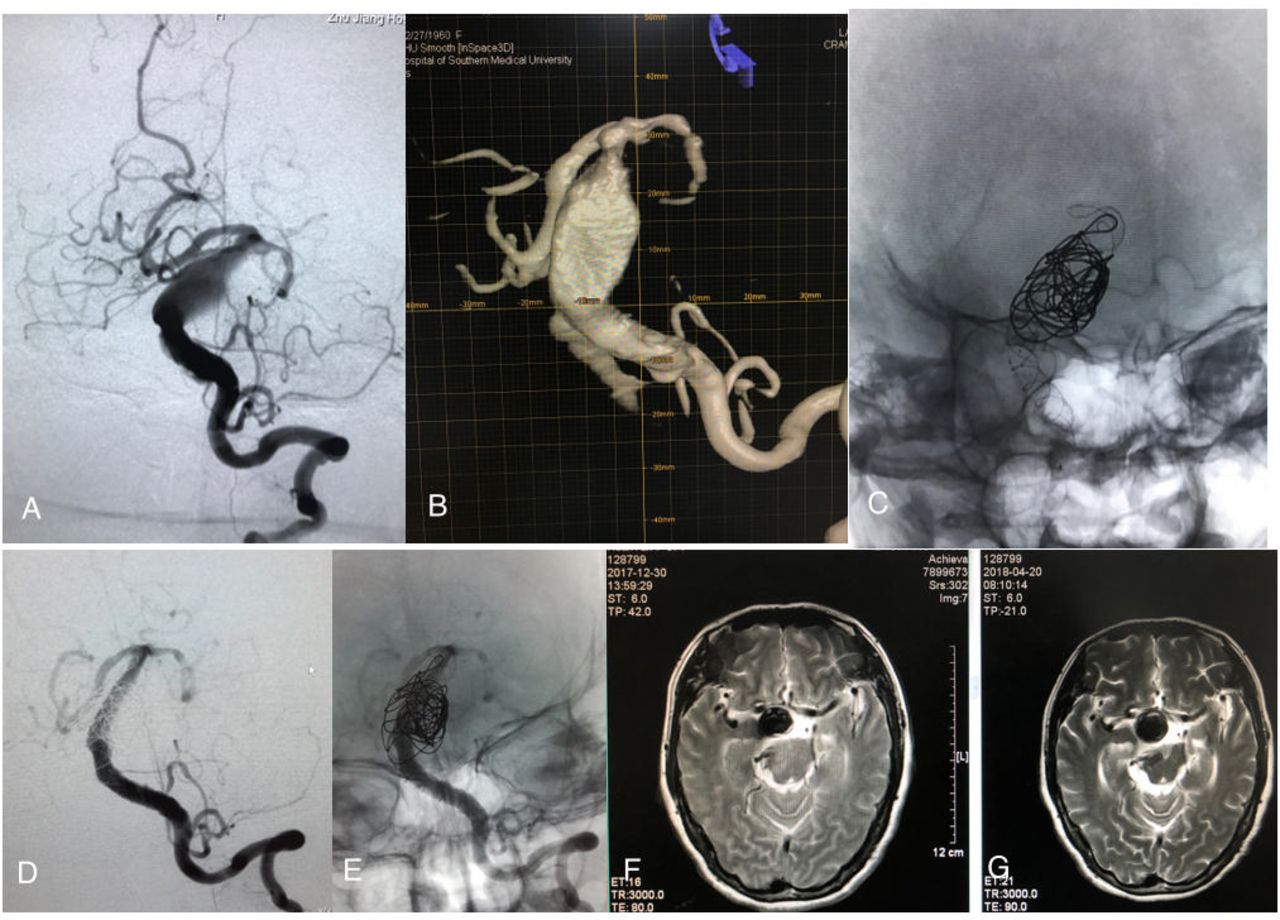
This patient had high blood pressure, drowsiness, and quadriplegia. (A,B) DSA showed ectasia and elongation from the distal part of the left vertebral artery to the whole basilar artery; (C) two Leo stents (5.5×75 and 5.5×50) covered the whole ectatic part. A solitaire stent (6×30) and a few coils were added in the fusiform aneurysm segment. (D,E) Angiography 3 months after treatment showed the whole lesion was reconstructed well. (F,G) MRI after treatment showed no change of the outer diameter of the dolichoectatic basilar artery but reduced edema in the brainstem.

{kind=link}
{kind=link}
This patient had brainstem hemorrhage. (A,B) DSA showed dilatation and elongation from the distal part of the left vertebral artery to the whole basilar artery; (C–E) three Leo stents (5.5×75, 5.5×50, 4.5×40) covered the whole ectatic part. (F,G) Angiography at 7 months after treatment showed the whole lesion was well reconstructed. CT (H) and MRI (I) at 7 months after treatment showed stable dolichoectasia of the basilar artery.
After general anesthesia and heparinization, an 8 F sheath was inserted into the right/left femoral artery. An 8 F guiding catheter was placed into the origin of the target vertebral artery, and a 5 F/6 F Navien guiding (Medtronic Inc, Irvine, California, USA) was advanced into the v2–v3 segment of the vertebral artery. If coiling of the severely ectatic segment or fusiform aneurysm was planned, another 5 F/6 F guide was placed into the same or contralateral vertebral artery through the contralateral femoral artery access. A Vasco + microcatheter for a Leo stent deployment (Balt, Montmorency, France) was advanced into the basilar artery through the Navien guiding catheter. If the entire basilar artery was ectatic, the Vasco + microcatheter were placed into one of the posterior cerebral arteries (PCAs) such that the Leo stent could cover the entire basilar artery. Another microcatheter was advanced into the severely ectatic segment or the fusiform aneurysm through the other 5 F/6 F guide to place the coils.
Outcomes assessment
All patients had follow-up cerebral angiography and MRI between 3 months and 1 year after embolization. Annual examinations with MRI/MRA were also planned after the initial follow-up. Modified Rankin Scale (mRS) scores were assessed before treatment and at 3 months after the procedure. Neurological assessments were obtained at the time of discharge, at the 3-month follow-up, and follow-up imaging.
Statistical analyses
Frequencies and percentages were calculated for categorical variables. Means and SD were calculated for continuous variables. A paired t-test was used to compare mRS scores before and after treatment. A p value <0.05 was regarded as significant. The Statistical Package for the Social Sciences version 13 (SPSS, Chicago, Illinois, USA) was used for all analyses.
Results
The demographics of the patients and results of embolization are shown in table 1. The 19 patients included two women and seventeen men with the mean age of 52 years (range 43–68). A 5.5 mm x 75 mm Leo stent was placed in each patient as the first stent. Five patients received only one Leo stent, 13 patients received a second Leo stent; and one patient received three Leo stents. Two patients had a 6 mm x 30 mm Solitaire stent and another patient had two 4.5 mm x 28 mm Enterprise stents placed inside the Leo stents.
The demographics of the patients and results of embolization
Two procedural complications (10.5%) occurred. One patient had migration of a pre-existing thrombus in the basilar artery to bilateral PCAs during access of the basilar artery. The PCAs were recanalized with intra-arterial thrombolysis and mechanical thrombectomy using a 4 mm x 15 mm Solitaire stent (Medtronic Inc, Irvine, California, USA). This patient had only drowsiness without focal neurological symptoms. He recovered completely in 2 weeks. The other complication was in the Leo stents at the site of a focal stenosis in the left vertebral artery 2 days after the operation. Although the artery was recanalized with intra-arterial thrombolysis, the patient remained in a deep coma and their family took them home for hospice care against medical advice.
Eighteen patients had follow-up DSA and MRI between 3 and 24 months. The follow-up angiography of 15 patients (15/18, 83%) showed complete reconstruction of the vessel (figures 1 and 2). The dilated parts of the vertebrobasilar arteries were reconstructed and the tortuous vessel was straightened, with reduced turbulence and restoration of laminar flow. MRI follow-up showed decreased edema in the brainstem, although the mass effect remained unchanged (figure 1). Two patients had very tortuous vertebral arteries, prohibiting the advancement of the Vasco + catheter into the PCA. As a result, the Leo stent covered only the proximal two-thirds of the lesion. The portion of basilar artery covered by the Leo stent shrunk to the size of the stents, but the distal portion of the lesion remained unchanged. In another two patients, follow-up DSA at 3 months showed residual flow to part of a fusiform aneurysm covered by the stent.
All patients showed clinical improvement after the treatment except for one patient with a procedural complication. Two patients were found to have new worsening dysphagia at 8 and 18 months, respectively, after the treatment. Clinical improvement was sustained in the other patients at 1-year follow-up. Overall, the mean mRS score was 3.00±1.15 before treatment and improved to 1.89±1.33 after treatment (p<0.01 by paired t-test).
Discussion
This series of 19 patients had a variety of clinical symptoms, including brainstem hemorrhage, brainstem compression, local ischemia, and distal embolism. The treatment of these patients using a woven stent with occasional reinforcing self-expanding stents and supportive coiling had a low complication rate. The treatment lowered the mRS score and demonstrated good clinical and angiographic outcomes up to 1 year.
These results compare favorably with the reported series of VBD treatment using flow-diversion stents. Early reports of VBD treatment with flow diversion showed a very high complication rate of >50%.5 6 11 12 A recent series by Natarajan et al showed a <10% rate of major complications, but their series consisted of 12 fusiform vertebrobasilar aneurysms without dolichoectasis.7 Treatment of these aneurysms has a lower complication rate than that of dolichoectatic or transitional aneurysms. Bhogal et al presented a large series of 58 non-saccular aneurysms within the posterior circulation treated with flow diversion.8 They included 24 patients (41.3%) with fusiform aneurysms without dolichoectasis, which is different from our series. According to the authors, this group of patients had a 75% complete occlusion rate and another 12.5% had a good response to treatment with only a minor aneurysm remnant. Only one death occurred in this group. All patients with pure dolichoectasia had good angiographic results. Nonetheless, in patients with transitional aneurysms, which were most similar to those in our series, only 42.8% of patients had good angiographic results. Moreover, only 37.9% patients of their series were symptomatic. The overall complication rate was 15.5%, but mortality in the symptomatic group was 22.7%. Although clinical improvement was seen for the asymptomatic patients, fewer symptomatic patients had a mRS score of ≤2 after treatment, dropping from 72.7% to 54.5%. In comparison, 78.9% of the patients in our series had an mRS score of ≤2 after treatment, increased from 47.4% before treatment. Furthermore, many patients required multiple treatments with multiple flow-diversion devices. Up to 19 stents were used and up to five treatments took place. An average of 1.86 treatments was carried out for transitional aneurysms. The cost of flow-diversion treatment was thus much higher than using large woven stents.
Other stents have been used in combination with coiling to treat VBD. van Oel et al 13 treated 13 basilar fusiform aneurysms with coils and laser-cut stents. In their 6–72 months' follow-up, 9 (69.2%) patients had good clinical and angiography results, whereas three patients had subarachnoid hemorrhage and two of them died. Wu et al 14 treated nine patients with symptomatic VBDs with stent-assisted coiling. Five of the patients had good clinical outcomes, but two patients had brainstem infarct and two patients died. Chen et al 15 reported the endovascular treatment of 10 patients with large vertebrobasilar fusiform aneurysms. Five patients were treated with self-expanding stents alone. Overall nine patients had good clinical outcomes. It is not clear how many of these patients were symptomatic. As the Bhogal series has demonstrated asymptomatic patients with fusiform aneurysms without dolichoectasia may have better outcomes than patients with transitional aneurysms.
Placement of stents in VBD can be challenging. The use of an intermediate catheter provided good support for the navigation of stent catheters into the PCA, allowing the entire VBD to be sealed with a stent. Nonetheless, the catheters could not reach the PCA in two patients and stents had to be deployed in the basilar artery. Despite incomplete covering of the basilar artery, healing was observed and symptoms improved.
A large woven stent may help the reconstruction of VBD by several mechanisms. First, the pore sizes of woven stents are smaller than those of laser-cut stents. They might have provided some degree of flow diversion, at least acting as a barrier to dampen the pulsatility of flow.16–18 MRI showed reduced flow voids outside the stent in all patients, supporting the flow-diversion effects of the woven stents. The placement of coils outside the stent could further reduce pulsatility and vessel wall pressure. None of the patients who showed improvement of mass effective symptoms had a reduction of VBD size on follow-up MRI, suggesting that dampening of pulsatility could be sufficient to alleviate the mass effect of VBD. Second, the stents could straighten the tortuous vessel, thus reducing turbulence, restoring laminar flow, and improving flow in distal branches. Combined with antiplatelet therapy, this treatment could decrease distal ischemic events. Third, overlapping woven stents or woven stents plus loose coiling might have allowed slow thrombosis of VBD outside the stent, gradually remodeling the VBD.
Brainstem infarction is a major concern for endovascular treatment of VBD. Some reports showed a brainstem infarct rate of up to 22.2%.14 Rapid thrombosis of VBD after flow-diversion stent placement or coiling and subsequent occlusion of the perforators are probably the culprit. Staged treatment and reduced coils have been advocated to reduce this complication.19 No brainstem infarction occurred in this case series, probably owing to the weak flow-diversion effect of Leo stents and loose coil implantation. As thrombus formed slowly and partially in the outside lumen, channels could have been maintained to the origin of the perforator. The outflow of these perforators might have provided enough draw of flow to keep them open under dual antiplatelet therapy. Alternatively, the patient might have developed collaterals to stay asymptomatic when the perforating arteries slowly occluded.
The woven stents have little radial force. They are not suitable for deployment in vertebral or basilar arteries with severe stenosis, where they may not fully expand. When the stents are constrained, they can become rigid and have poor wall apposition. One of the thrombotic complications in our series happened in this situation. Angioplasty and placement of additional self-expanding stents may be necessary to keep the stent fully open but may carry a risk of vessel rupture.
This study is limited by the small number of cases and rather short follow-up period. Two patients showed recurrent symptoms beyond 8 months, despite early clinical improvement and good restoration of angiographic appearance.
Conclusions
Patients with VBD treated with large woven stents with or without supportive coiling may have good clinical and imaging results in the short- to mid-term. Further studies are warranted to assess the long-term outcome of this treatment.
References
Footnotes
Contributors XH: substantial contributions to the conception, design of the work, analysis of date for the work, and drafting the work;. JZ: substantial contributions to acquisition of data for the work;. XL: substantial contributions to interpretation of data for the work;. XZ: revision of the article; ZL:substantial contributions to acquisition of data for the work; CD: revision of the article critically for important intellectual content and final approval of the version to be published. All authors: agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This article was supported by the National Key Research Development Program (2016YFC1300804 and 2016YFC 1300800) and National Natural Science Foundation of China (81400943).
Competing interests None declared.
Ethics approval Institutional review board approval of Zhujiang Hospital was obtained for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.