Article Text

Abstract
Background The prevalence of women physicians is steadily rising, but the field of neurointervention remains one of the most male-dominated subspecialties in medicine. A fear of radiation exposure, particularly during pregnancy and childbearing years, may be responsible for deterring some of the best and brightest. This is the first study to examine the amount of maternal and fetal radiation exposure during a pregnant neurointerventional fellow’s training.
Methods We retrospectively analyzed the radiation exposure of a neurointerventional fellow prior to and during pregnancy from February 2018 to May 2019 in 758 neurointerventional cases. The collar dosimeter was used to measure overall maternal exposure and an additional fetal dosimeter was worn under two lead apron skirts to estimate fetal radiation exposure.
Results There was not a significant difference between pre- and post-pregnancy overall maternal radiation exposure as measured by the collar dosimeter (151 mrem pre-pregnancy and 105 mrem during pregnancy, p=0.129). Mean fluoroscopy time and fluoroscopy emission per procedure also did not differ prior to and during pregnancy. Fetal radiation exposure measurements from both the Mirion Genesis Ultra TLD dosimeter as well as the Mirion Instadose dosimeters worn under double lead apron skirts were 0 mrem for all 6 months.
Conclusion These findings suggest that, when optimal radiation safety practices are implemented, the fetal dose of a pregnant neurointerventionalist is negligible. Further studies and education are necessary to encourage women to choose neurointervention and allow practicing women neurointerventionalists to maintain their productivity during their reproductive years.
- angiography
- complication
- intervention
- malformation
- standards
Statistics from Altmetric.com
Introduction
Neurointerventional procedures are performed by a number of medical specialties including neurosurgery, neurology, and radiology. With a rising need for mechanical thrombectomy as well as the replacement of open transcranial approaches with improving endovascular techniques, both the number of neurointerventional procedures performed and the demand for neurointerventionalists are rapidly rising.1–3 For the third year in a row, women have comprised the majority of medical school matriculants (52.4% in 2019, 51.6% in 2018, and 50.7% in 2017).4 However, neurosurgery and interventional radiology are among the most male-dominated medical specialties (91.6% and 90.5%, respectively).5 Radiation exposure is commonly cited as the largest deterrent for both male and female medical students when choosing interventional subspecialties.6 However, women of childbearing age assume the sole responsibility of potential fetal exposure. As pregnancy remains one of the most important issues for young women in choosing a residency program,7 the risk of radiation to a fetus is likely a chief explanation for a lower number of women physicians choosing a career in neurointervention.
Epidemiologic studies examining occupational radiation exposures in medical workers have found little evidence of health risks in those exposed after 1950.8 However, the majority of studies are of interventional cardiologists and estimated effective doses to the physicians vary significantly. There are very few studies examining occupational radiation exposure in neurointervention. Yet, compared with other interventional procedures, neurointerventions involve biplanar x-ray, are longer, more complex, and often use faster frame rates and imaging views that are unfavorable for operator exposure. In this study we present the first report of occupational radiation exposure of a pregnant neurointerventional fellow pre- and post-conception. We also review the literature on occupational radiation exposure in pregnancy and discuss best practices for radiation safety during pregnancy. Figure 1 provides a list of crucial concepts and units necessary to understand radiation exposure risks.
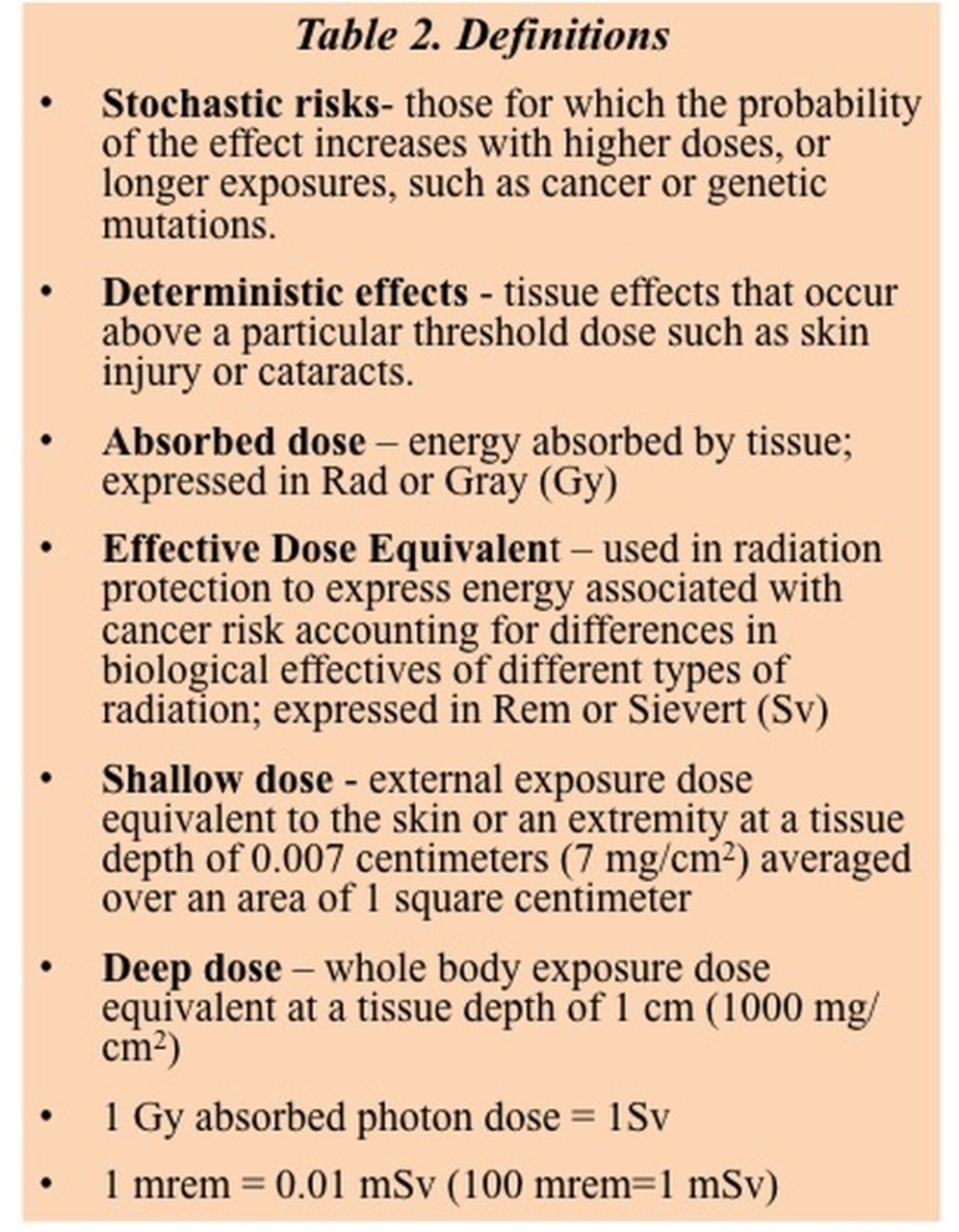
Definitions of common radiation terms.
Methods
We retrospectively analyzed the radiation exposure of a neurointerventional fellow between February 2018 and May 2019 in 758 neurointerventional cases (table 1). The fellowship ended in mid-June 2019 and thus June data were not included. Radiation exposure was measured with a Mirion Genesis Ultra TLD device (Irvine, California, USA) worn on the collar over the thyroid protector as per institutional protocol. Prior to pregnancy, the fellow was wearing a two-piece 0.5 mm lead skirt and vest, thyroid shield, protective glasses, and 0.25 mm head cap. During pregnancy, the fellow electively chose to wear two lead apron skirts and an additional fetal dosimeter was worn under the apron skirt in the center of the lower abdomen. Both collar and fetal dosimeters were monitored monthly with reports provided to the fellow by the institutional Radiation Control Center. The fellow also wore the Mirion Instadose Dosimeter device, which allows real-time radial dose monitoring on the wearer’s smart phone. This device was also worn under both lead aprons. During pregnancy, the fellow maximized her distance from the radiation source when not actively participating but otherwise did not significantly modify her behavior.
Neurointerventional fellow radiation doses over 16 months prior to and during pregnancy
For all cases at our institution, standard IR suite radiation protection consists of a 0.5 mm lead glass overhead mobile shield, lower body lead shield, and additional accessory vertical extension body shield (figure 2). All cerebral digital subtraction angiography and interventions are performed using a Siemens Artis Q or Artis Zee Biplane Machine at a usual pulse rate of 7.5 pulses/s and frame rate of 3 images/s. We obtained the total fluoroscopy time (time in minutes that radiation is being emitted from the fluoroscopy equipment) and total radiation emitted by the fluoroscopy equipment from the report generated by the fluoroscopy systems. Total radiation was converted to the current standard kerma-area product (KAP) in Gy·cm2.

{kind=link}
{kind=link}
Lead shield configuration in biplanar angiography suite with (A) ceiling mounted clear upper body shield with patient contour, (B) detachable lower body shield that mounts to (C) lower body shield mounted on side rail.
Statistical analysis
Data are presented as mean±SD for normal continuous variables and as frequency for categorical variables. Statistics of means were carried out using the unpaired Student t-test, with and without equal variance (Levene’s test) as necessary, and Wilcoxon rank sum tests when variables were not normally distributed. A simple linear regression analysis was performed between radiation emission (Gy·cm2) and radiation exposure (mrem). Statistical analysis was carried out with Graphpad Prism 8.3. A p value ≤0.05 was considered statistically significant.
Results
The fellow performed 758 cases between February 2018 and May 2019 including 381 diagnostic cerebral angiograms and 377 interventional procedures (ie, mechanical thrombectomy, aneurysm embolization, vascular malformation and fistula embolization, tumor embolization, intracranial and extracranial stenting, balloon angioplasty, intra-arterial chemotherapy administration, sclerotherapy, and more). The average number of cases performed per month prior to pregnancy was 47.8±12.7 and during pregnancy was 46.7±11.9 (p=0.862). Radiation reports were available for 10 months before pregnancy from February 2018 to November 2018 and during the first 6 months of pregnancy from December 2018 to May 2019. Prior to pregnancy the mean monthly radiation exposure as measured by the whole body collar dosimeter was 151 mrem shallow (range 20–326) and 147 mrem deep (range 20–326). It should be noted that the dosimetry was combined for July and August 2018. During pregnancy the mean monthly radiation exposure as measured by the whole body collar dosimeter was 105 mrem shallow (range 69–142) and 94 mrem deep (range 66–121). There was not a significant difference between pre- and post-pregnancy overall maternal radiation exposure (p=0.129). Recordings from the fetal dosimeter under double apron skirts were 0 mrem for all 6 months. Fetal radiation exposure via the Mirion Instadose dosimeter was also undetectable throughout pregnancy with 0 mrem cumulative dose.
There were 695 fluoroscopy reports available from the Siemens Artis Zee (241 cases) and Siemens Artis Q (453 cases). Total fluoroscopy time per procedure was not significantly different prior to and during pregnancy (31.4±34.5 min and 34.9±45.2 min, respectively, p=0.249). Total radiation emitted per procedure was also not significantly different prior to and during pregnancy (145.4±130 Gy·cm2 and 130.7±121.2 Gy·cm2, respectively, p=0.143). There was a significant positive linear correlation between the sum of total radiation emissions per month and the monthly radiation exposure measured by the collar dosimeter (F(1,13)=8.754, p=0.011 with R2 of 0.402). Of note, total radiation emission of the older Siemens Artis Zee was significantly higher than that of the Siemens Artis Q for diagnostic cerebral angiograms (169.9+82.1 and 98.0±89.6 Gy·cm2, respectively, p<0.0001).
Discussion
This is the first study evaluating occupational radiation doses during pregnancy in a neurointerventional fellow. There are few published data on fetal effects attributable to occupational maternal radiation exposure and, thus, there is a significant fear among students and operators. In a recent survey of medical students, 79% were concerned about pregnancy during training and 31% of women were specifically concerned about radiation exposure during training.7 Furthermore, only a minority of programs in radiation-dominated fields have formal guidelines for radiation safety in pregnant operators.9 10 With women constituting over 50% of medical students, it is imperative to understand and communicate the true risks of radiation exposure in neurointervention to attract and retain the best candidates. In this study we found 0 mrem of fetal radiation exposure with the use of proper radiation safety practices without significant changes in the fellow’s case volume, fluoroscopy time, or overall radiation exposure before and during pregnancy. There was a significant positive correlation between radiation emitted by the fluoroscopy machines and dosimeter-detected maternal radiation exposure, but no effect on fetal radiation exposure.
Concerns of sterility and hereditary effects are associated with preconception radiation exposure. The United Nations Scientific Commission on Effects of Atomic Radiation (UNSCEAR) analyzed the scientific data from animal studies and survivors of the atomic bombings at Hiroshima and Nagasaki and reported that the risk of hereditary effects in humans increases by 0.41% to 0.46% per 1000 mGy of exposure. This equates to 20 years of maximum occupational exposure of 5000 mrem per year. They also report that reproductive sterility is a deterministic effect in women at a threshold dose of 12 000 mGy before puberty or 2000 mGy in adults.11 While there are limited data, occupational radiation doses per neurointerventional procedure appear to range from 2 to 18 mrem, which equates to merely 0.18 mGy.12–15 Thus, the risks of sterility and hereditary effects in future children are very low.
Post-conception, it is well known that the human embryo/fetus is highly susceptible to damage from ionizing radiation.16 Exposure can cause significant adverse health effects including congenital malformations, growth retardation, cancer, intellectual disability, and embryonic death. The effects of radiation exposure depend on multiple variables including gestational age, fetal cellular repair mechanisms, and absorbed radiation dose level (table 2). Radiation risks are highest when there are a high fraction of proliferating cells. Thus, the radiation risks are most significant during the first trimester,17 less in the second trimester, and least in the third trimester.18 19 While there is no evidence that low levels of radiation (<100 mGy) have adverse effects on human embryos/fetus, there are also no clear recommendations for the maximal safe radiation dose.
Fetal threshold dosages associated with possible deterministic effects of radiation24
The National Council for Radiation Protection (NCRP) has published recommended dose limits to prevent deterministic effects and minimize the risk of stochastic effects. The occupational exposure annual deep dose equivalent limit is 5000 mrem for the worker and the fetal limit is 50 mrem per month or 500 mrem for the duration of the pregnancy.20 In the USA, the declaration of pregnancy is voluntary. However, once pregnancy is declared, a fetal dosimeter is provided to be worn at the level of the abdomen under protective lead garments for additional fetal monitoring. It should be noted that this dosimeter likely overestimates the true fetal dose, as radiation attenuation by the mother’s tissues is not considered. It is notable that in this study the fetal dose was 0 mrem throughout the duration of pregnancy, as corroborated by two dosimeters.
Marx et al prospectively monitored 30 interventional radiologists over 1 year and found a mean monthly deep dose equivalent of 9 mrem under 0.5 mm lead at the waist and 3 mrem under double lead 1.0 mm lead aprons.21 Similar to our findings, Chandra et al retrospectively examined 14 pregnant interventionalists (radiologists, cardiologists, urologists, and vascular surgeons) and found average overall radiation exposures of 188 mrem before pregnancy, 136 mrem during, and 147 mrem after pregnancy. Despite a non-negligible dose to the mothers, the fetal monitors rounded to 0 mrem during pregnancy.22 Both studies concluded that the maternal and fetal radiation doses of working interventionalists are significantly below the conservative NCRP threshold and there is minimal radiation risk during pregnancy when following the appropriate precautions.
The radiation dose to the patient and medical staff should always be minimized to as low as reasonably achievable (ALARA principle), particularly in the pregnant neurointerventionalist. The key radiation protection concepts are time, distance, and shielding. The majority of the dose to personnel is due to scatter from patients. Thus, positioning the x-ray tube as close as possible to the image receptor and increasing the distance from the operator to the patient all decrease scatter. Operators should also be aware that scatter is higher on the x-ray tube side of the table. Tableside lead drapes should be positioned between the x-ray tube and operator to shield from the bottom of the table and an overhead leaded acrylic shield should be placed close to the patient between the operator and patient. Fluoroscopy strategies to decrease radiation exposure include proper collimation of the x-ray field to the area of interest, minimizing frame rate, and minimizing digital subtraction angiography runs.23 Stepping away from the fluoroscopy table and exchanging proximity to the x-ray tube as operator versus assistant when appropriate can also significantly decrease the amount of radiation experienced.
A pregnant neurointerventionalist should wear at least a 0.5 mm lead protection over her abdomen, ideally a skirt with overlapping vest. There is little evidence to suggest that double or even triple leading significantly contributes to decreasing fetal radiation and may result in an increased risk of back pain or injury. Overhanging lead aprons may be ideal due to their low gravity effect on the already physically taxed pregnant interventionalist; however, only a few institutions currently employ them. Finally, while disclosure of pregnancy is purely voluntary, disclosing may encourage best practices and collaboration among the team as well as close monitoring with fetal dosimeters. Furthermore, using real-time radiation monitors allows for immediate feedback to the operator who can then appropriately improve radiation safety practices.
This study is limited in that it is a report of occupational radiation doses of a single neurointerventional fellow. Operator and fetal radiation exposures may vary among centers with different machines, protective shielding, case volumes, distribution of cases, and practice techniques. Furthermore, time spent as the primary operator versus assistant and thus proximity to the x-ray tube may differ significantly among fellows and attendings. However, the results of this study are encouraging and warrant further attention from the neurointerventional community. A diverse workforce leads to adaptability, innovation, and improved patient–physician relationships. Persistent under-representation of women in neurointerventions hinders recruitment, productivity, salary, and career advancements. Further studies as well as establishment of formal guidelines will encourage the recruitment and retention of the best and brightest to neurointervention.
Conclusion
When optimal radiation safety practices are implemented, the fetal dose of a pregnant neurointerventionalist is negligible. Further studies and education regarding occupational radiation exposure safety are necessary to encourage women to choose neurointervention and allow practicing women neurointerventionalists to maintain their productivity during their reproductive years.
References
Footnotes
Contributors All authors contributed to the conception, data gathering, and drafting of the manuscript. All authors critically reviewed the manuscript and approved its final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Individual de-identified participant data will be shared upon reasonable request.