Article Text

Abstract
Background The COVID-19 pandemic has changed the way medicine is practiced, including the implementation of virtual care in many specialties. In the field of interventional neuroradiology (INR), virtual clinics are an uncommon practice with minimal literature to support its use. Our objective was to report prospective, single-centre data regarding patient and physician experience with virtual INR clinics for routine follow-up appointments.
Methods We surveyed all patients that participated in a virtual INR clinic follow-up appointment at our hospital over a 3 month period. Information gathered included length of appointment delays (ie, wait times), length of appointment times, overall satisfaction, and perceived safety metrics. A survey was also sent out to all physicians who participated in virtual clinics with similar questions.
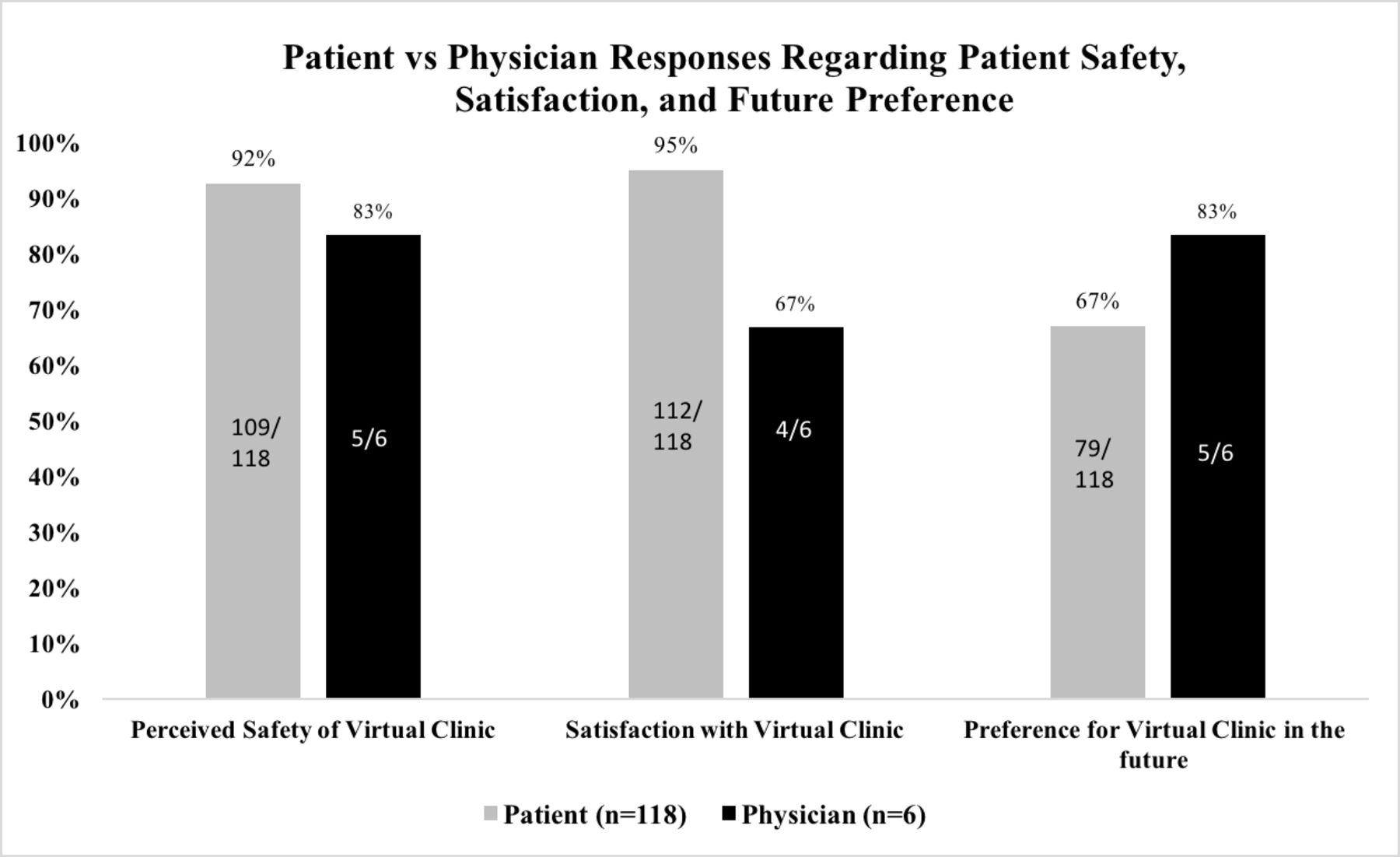
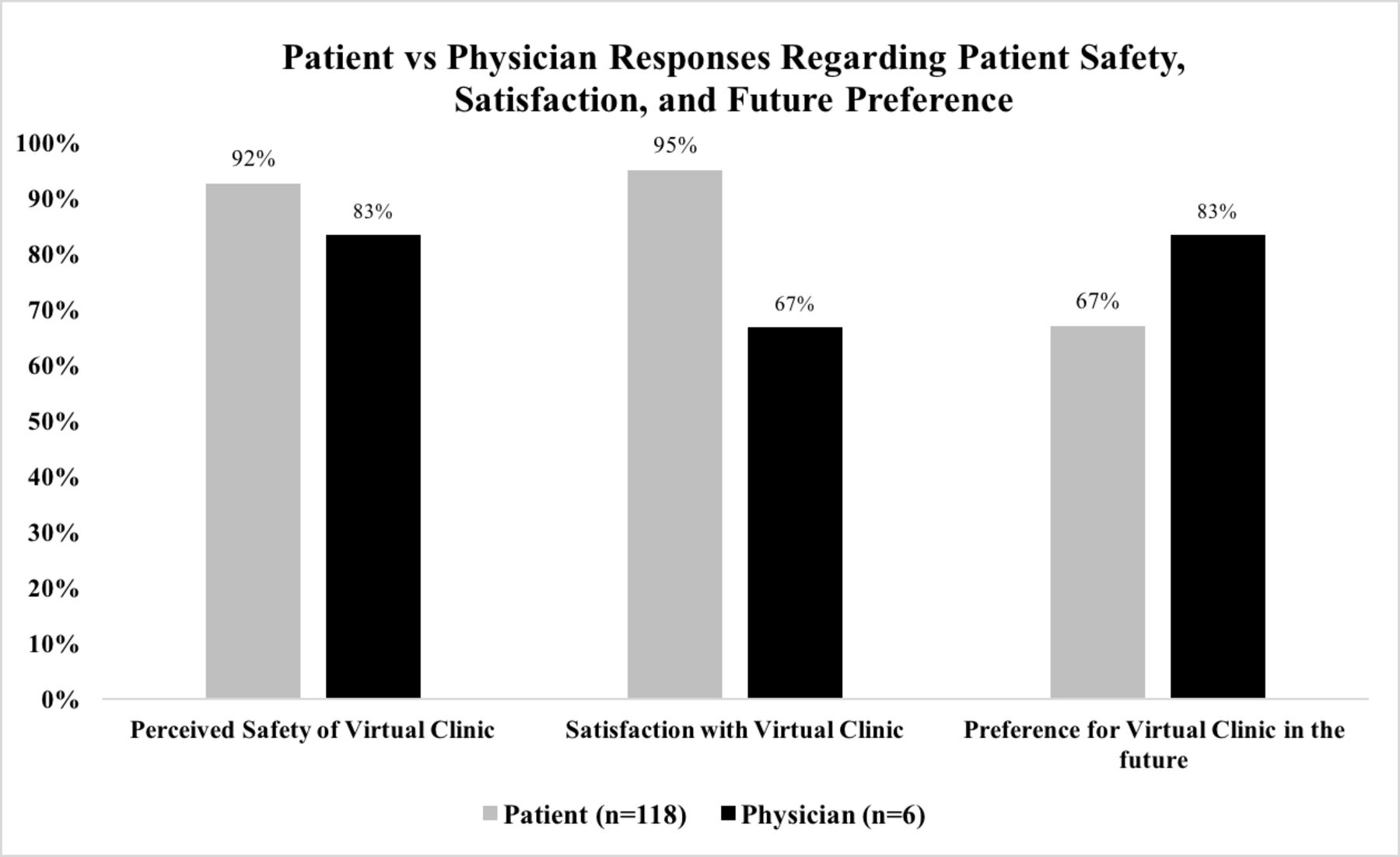
Results 118/122 patients and 6/6 physicians completed the survey. Wait times before previous in-person appointments were perceived to be much longer than virtual appointments, whereas in-person appointment times were longer. 112/118 (94.9%) patients and 4/6 (67%) physicians reported general satisfaction with their virtual clinic experience. There were 8/118 patients who felt their conditions could not be safely assessed virtually, compared with 1/6 (17%) physicians. Lastly, 72.2% of patients reported that they would prefer virtual or telephone visits in the future for non-urgent follow-up, and 5/6 (83%) of physicians reported the same.
Conclusion Virtual INR clinics are more efficient and are preferred among patients and physicians for non-urgent follow-up appointments. Our study demonstrates the feasibility of a virtual platform for INR care, which could be sustainable for future practice.
- standards
- technology
- economics
- intervention
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
The novel Coronavirus Disease 2019 (COVID-19) pandemic has changed the way we live and practice modern day medicine.1 In an effort to practice physical distancing, many specialties have moved routine patient encounters to telephone and virtual platforms.2–4 These changes may not be temporary.
Telemedicine is an emerging tool that precedes the time of COVID-19; its initiation was already implemented in many other specialties, including neurology, as a means of delivering subspecialty care to remote/rural regions.5–7 However, in the field of interventional neuroradiology (INR), virtual clinics are an uncommon practice with minimal literature to support its use. Here, we report data from the first documented INR virtual clinic. Our objective was to evaluate patient and physician satisfaction and self-perceived safety metrics to determine whether a virtual INR clinic was a feasible platform for delivering future care to patients.
Methods
Patient consent and Research Ethics Board approval
The study received research ethics exemption from the Ottawa Health Science Network Research Ethics Board. The study involved implied consent via survey completion. A master list linking identifying information and survey responses was not kept.
Patients, subjects and setting
Our hospital is a quaternary referral center with an INR service that provides the entire spectrum of INR care to a population of approximately 2 million patients. Our team consists of three fellows and five fellowship-trained, experienced INR attending physicians: two from a neurosurgery residency background, two from neuroradiology, and one from neurology. All fellows and attendings participated in in-person and virtual clinics. From March 13, 2020 onward, our INR service moved all clinical visits to “virtual”, and all in-person clinics were postponed with the exception of urgent or emergent visits necessitating physical examination. Virtual platforms consisted of computer-based video conference calls via encrypted apps such as Zoom, or telephone-based encounters. The studied patient population included patients with aneurysms, dural fistulas, arteriovenous malformations, tumours and large vessel atherosclerotic disease. All appointments were booked as 15 min follow-ups. All of the patients had either been previously seen in clinic for in-person consultation prior to the pandemic, or had an emergency INR procedure done and were being seen in follow-up, weeks later. None of the surveyed patients had experience with virtual INR clinics before. There were no new consultations included in our study.
Before the appointment, patients were asked if they had the technology necessary to perform a virtual follow-up appointment. If video capability was not available, telephone encounter was used instead. We collected data from 118 consecutive patients from March 13 to June 25 who participated in a virtual routine follow-up visit in lieu of the postponed in-person visit. Patients were all surveyed after, but on the same day as, their virtual appointment. A sample copy of the survey questions asked can be accessed through the online supplemental materials. “Wait times” were defined as time spent in the waiting room before seeing the physician for in-person appointments, or time spent waiting for the virtual appointment past the scheduled time for virtual appointments. Length of appointment was a self-reported metric by patients, and indicates the amount of time spent with the physician during the appointment, and does not include wait times or delays. Post-appointment data collection was done over the phone following the patient’s visits with the INR service by either a trained research assistant or physician.
Supplemental material
Survey feedback was also collected from the INR physicians who attended the clinics. A sample copy of the survey questions asked can be accessed through the online supplemental materials. Four attending physicians and two fellows participated.
Statistical analysis
Age was reported as median (±IQR), given its non-normal distribution, as assessed graphically by histogram. Wait times and appointment times were collected as ranges (ie, <10 min, 10–20 min, 20–30 min, etc). Therefore, all variables were categorical and were summarized as frequencies and percentages. Given that we surveyed all patients, rather than a sample, no confidence intervals were presented. Overall satisfaction with virtual care was graded on a 7-point scale, ranging from “very dissatisfied” to “very satisfied”. Statistical analysis was performed with dichotomization of satisfaction score: “satisfied” (includes “very satisfied”, “satisfied”, and “somewhat satisfied”) versus “not” (which included all other points on the scale). Comparisons between groups were performed using χ2 test, Fisher’s exact test or Mann-Whitney U test, as appropriate. Spearman correlation coefficients were calculated to identify associations between variables and overall satisfaction and future preference for virtual visits. Statistical testing was conducted at the two-tailed α level of 0.05. All statistical analyses were performed with SPSS v26.0 (IBM, Armonk, NY).
Results
Patient data
We surveyed a total of 122 patients, and 118/122 patients completed the survey, giving us a completion rate of 96.7%. Of the 118 patient survey responses, 92 were administered by a research assistant not involved in patient care, and 26 were administered by an INR fellow. Four patients had incomplete survey responses. The mean age was 60 (±13.7) years. There were 58 males (49.2%). The diseases being treated included vascular malformations (ie, fistulas, aneurysms, arteriovenous malformations), carotid stenosis and intracranial stenting.
Of the 118 patients surveyed, 10 had never had an in-person appointment before because they had only had an emergency INR procedure done previously. All 108 patients with a previous in-person appointment reported at least some delay to their appointment associated with in-person visits in the past. In contrast, 76/118 patients (64.4%) reported they experienced no wait time prior to their virtual appointment (figure 1). Length of average appointment times were shorter with virtual visits than in-person: 93/118 (78.8%) patients reported their virtual appointments were <20 min, but 37/108 (34.6%) patients reported in-person appointments lasting <20 min (figure 1).

Length of in-person versus virtual wait times (A) and appointment times (B) for non-urgent routine follow-up appointments with the interventional neuroradiology department at our hospital. Results were collected from 118 patients over a 3 month period.
Patient satisfaction was graded on a 7-point scale, ranging from “very dissatisfied” to “very satisfied” (see online supplemental appendix 1): 112/118 (94.9%) patients reported general satisfaction (ie, either “somewhat satisfied”, “satisfied” or “very satisfied”), with the majority of those patients (72/112 or 64.3%) reporting maximum satisfaction, with “very satisfied” as their answer. The remaining 6/118 (5.1%) patients gave a neutral response (ie, “neither satisfied nor dissatisfied”). No patient reported an unsatisfactory response (ie, “somewhat dissatisfied”, “dissatisfied”, “very dissatisfied”) (figure 2). There was a negative correlation between virtual wait times and overall degree of satisfaction (Spearman’s correlation coefficient of −0.369; p<0.001). There was no statistically significant difference in age or gender between patients who were satisfied versus those who were not.

Overall satisfaction rating by patients and physicians after their experience with the virtual interventional neuroradiology clinic at our hospital.
Of the 108 patients who previously had an in-person clinic visit, 78 (72.2%) reported that they would prefer virtual or telephone visits in the future for non-urgent follow-up. There was no difference in age or gender between those who wanted in-person versus virtual follow-up in the future (p=0.823 and p=0.244, respectively). However, those who preferred in-person visits seemed to have longer virtual wait times: 34% of patients who preferred in-person visits experienced no wait time before their appointment, whereas 73% of patients who preferred virtual visits had no wait. Length of appointments were also shorter in the group of patients who preferred the virtual platform: 69/78 (88.4%) patients had an average appointment length that was <20 min, whereas 24/39 (61.5%) of patients who preferred in-person visits had the same (p<0.001).
Lastly, 8/118 patients felt either unsafe or were concerned that their condition could not be assessed accurately over virtual platforms. None of them were redirected to seek emergency medical attention. Of the eight patients who felt unsafe, seven of them said they would prefer in-person visits in the future (figure 3).
{kind=link}
{kind=link}
{kind=link}
Patient versus physician responses regarding safety of virtual clinics, overall satisfaction with virtual clinic experience, and preference for future appointments.
Physician data
All physicians have held both in-person and virtual clinics. The length of virtual appointments were perceived to be shorter than in-person visits, with virtual appointments reported to last 10–20 min on average by 5/6 physicians, and <10 min by one physician. In contrast, in-person appointments were reported to be 20–30 min on average by 5/6 physicians, and 30–40 min by one physician (figure 1). Overall, 4/6 INR physicians were “very satisfied” (ie, maximum satisfaction) with their virtual clinic experience, while the other 2/6 physicians were “neither satisfied nor dissatisfied” (figure 2).
Only 1/6 physicians felt the safety of their patients could not be accurately assessed with a virtual appointment, and 2/6 physicians had to direct a patient to the nearest emergency department or for urgent in-person examination at least once during the 3 month period. Both of those physicians reported that they had only done that rarely (ie, less than five times total). Finally, 5/6 physicians said they would prefer virtual clinic visits in the future for routine, non-urgent follow-up (figure 3).
Discussion
This is the first report of a virtual platform for delivering INR care to patients for routine, non-urgent follow-up appointments. Our results show that overall virtual appointments have shorter wait times, shorter appointment times, high rates of patient and physician satisfaction, and are preferred over in-person visits by most patients and physicians, even in the absence of physical distancing recommendations in the future. We identified that longer wait times and perceived safety concerns were associated with a preference for future in-person visits.
The benefits of telemedicine are numerous. From a patient perspective, it allows the delivery of subspecialty care to patients in rural regions, limiting the need for transportation and improving healthcare access in remote areas.5 It also allows for patients with reduced mobility to stay home for assessments and decision-making. Those who were assessed by video conference platforms were also able to view relevant images shared with them from the physician’s screen. From a physician’s perspective, our data suggest that virtual appointments are associated with shorter wait times and appointment times, thus improving our efficiency. It is important to note that despite the general healthcare slow down and reduced volumes associated with the pandemic,8 the volume of patients seen in virtual clinic at our center did not significantly decrease compared with pre-pandemic times. However, it’s still unclear to us if these shorter virtual wait times may or may not persist beyond the pandemic, and future follow-up data are warranted. Nevertheless, during the pandemic period when physical distancing is key, virtual appointments serve as an effective alternative to in-person appointments and prevent the build-up of backlogs during this time of uncertainty. Furthermore, its use may be extended to research settings, given the widespread disruption of research during the pandemic.9
The limitations of virtual care are largely related to the inability to physically examine a patient. However, many aspects of the neurological examination can be adapted to be virtually assessed, particularly if screen-sharing is available through the video conference platform.10 11 While crucial aspects of the examination such as funduscopy, muscle tone and reflexes cannot be assessed virtually, the physician may organize an in-person visit or direct the patient to seek emergency care if necessary. In patients who had previously been examined in person, virtual follow-up appointments were felt to be appropriate, although we recognize that a standardized triage system may be beneficial for new consultations in the future.12 Furthermore, many of the follow-up visits in an INR clinic are based on reviewing imaging results from cerebral angiograms, interventions, ultrasounds, CTs and MRIs. Other limitations include technological challenges and potential breaches of confidentiality. At our hospital, video conference links were encrypted through the Zoom application, which was quickly built into our Electronic Medical Record system at the beginning of the pandemic. Encryption gives Zoom the added security advantage and the ability to perform a comprehensive virtual examination, thus making video conferencing platforms preferable to telephone encounters. However, we recognize that its use may be limited by the technological or financial challenges faced by some patients, as it requires a device with access to high-speed internet, speakers, and microphone. Lastly, vast implementation of virtual care may be vulnerable to regional differences in insurance/renumeration patterns, which is a challenge that is beyond the scope of this study.
The main limitation of this study is that it was restricted to a single center, resulting in a small sample size, particularly for physician survey responses, despite every INR physician at our center participating in the study. In addition, 22% of the patient surveys were administered by a physician, which may result in social desirability biases. However, the remaining 78% of survey responses were collected by a research coordinator not involved in patient care. We did not perform subgroup analysis stratified by survey administrator. Finally, these results come from a population of follow-up patients who have previously had an in-person examination, and therefore may not be accurately extrapolated to new INR consultations. However, virtual methods of conducting initial consultations have been implemented in other specialties at our hospital, including neurology, and this may be an area for future research for our INR service.
Conclusion
Virtual INR clinics are more efficient and are preferred among patients and physicians for non-urgent follow-up appointments. Our study demonstrates the feasibility of a virtual platform used to deliver INR care, which could be sustainable for future practice.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rondalun1
RL and GW contributed equally.
Contributors RL and GW contributed equally to this paper. GW, RF, and BD conceptualized the project. GW and ZD performed data acquisition. RL performed data analysis. All authors participated in interpretation of the data. RL drafted the manuscript, and all authors contributed to revising/editing for intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study received research ethics exemption from the Ottawa Health Science Network Research Ethics Board. The study involved implied consent via survey completion. A master list linking identifying information and survey responses was not kept.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.