Article Text

Abstract
Background Trials of endovascular thrombectomy (EVT) mostly excluded patients with large core strokes so the safety and efficacy of EVT is not well established in such patients. Moreover, the definition of large core and its measurement differ between semi-quantitative (ASPECTS) and quantitative (core volume) imaging modalities. We evaluated functional and safety outcomes in studies reporting large core stroke patients treated with EVT and compared them with patients treated with medical management (MM) only.
Methods A systemic search using three large databases was performed to identify studies evaluating functional and safety outcomes in patients with large core strokes (ASPECTS<6 or core volume ≥50 cc) on CT, MRI, and Perfusion imaging according to PRISMA guidelines. A random-effect meta-analysis model was used to pool reported outcomes.
Results Twelve studies reporting outcomes for patients treated with EVT compared with MM in large core strokes were included. A pooled random-effect meta-analysis of large core patients by either definition (ASPECTS <6 or ischemic core volume ≥50 cc or both) demonstrated increased functional independence (mRS-scores 0–2) rates with EVT (EVT: 122/491 (25%), MM: 45/691 (7%), pooled OR: 4.39 [95% CI: 2.53 to 7.64], overall effect Z-score: 5.25, P<0.00001, I2=37%, P for Cochran Q:0.15) and decreased mortality (EVT: 101/439 (23%), MM: 215/645 (33%), pooled OR:0.53 [95% CI: 0.40 to 0.71], overall effect Z-score:4.32, P<0.0001, I2=0%, P for Cochran Q:0.78) at 90 days, without significant increase in symptomatic intracranial hemorrhage (ICH) (EVT: 42/462 (9%), MM: 35/663 (5%), pooled OR: 1.68 [95% CI: 0.92 to 3.09], overall effect Z-score:1.68, P=0.09, I2=26%, P for Cochran Q:0.24). Similar effects were observed in studies reporting large core outcomes based on ASPECTS <6 and ischemic core volume ≥50 cc. We observed no heterogeneity between quantitative vs semi-quantitative large core definitions, different ischemic core thresholds, and studies reporting outcomes over different time windows in subgroup analyses.
Conclusion In large core stroke patients, EVT is associated with improved functional independence and lower mortality at 90 days without significant increase in symptomatic ICH across various definitions, thresholds of large core size, and time windows. Further randomized evidence is warranted to establish EVT efficacy and safety in this population.
- stroke
- thrombectomy
- CT perfusion
- CT
- MRI
Statistics from Altmetric.com
Introduction
Endovascular thrombectomy (EVT) improves outcomes in selected acute ischemic stroke (AIS) patients with large vessel occlusion (LVO).1–7 However, EVT trials in the early time window (up to 6 hours from last known well (LKW)) largely enrolled patients with favorable imaging profiles using restrictive imaging selection criteria on either non-contrast CT (REVASCAT: CT ASPECTS≥7 and DWI ASPECTS≥6, ESCAPE: CT ASPECTS≥6, SWIFT-PRIME: CT/DWI ASPECTS≥6) or Perfusion imaging (EXTEND IA: ischemic core <70 cc and part of SWIFT PRIME≤50 cc with favorable penumbral mismatch profile).2–5 In the late time window (>6 hours from LKW), both DAWN and DEFUSE 3 used specific inclusion criteria for both CT (DAWN: ischemic changes involving <1/3 of MCA territory; DEFUSE 3: CT/DWI ASPECTS≥6) and Perfusion imaging (DAWN: ischemic core ≤50 cc, ≤30 cc, or ≤20 cc with appropriate age and NIHSS criteria; and DEFUSE 3: ischemic core <70 cc with favorable penumbral mismatch profile).6 7 As a result of these restrictive imaging criteria, AIS patients with significant ischemic changes (ie, large core) were largely excluded. Thus, EVT efficacy and safety is untested in the large core population using either CT or Perfusion imaging.
The likelihood of achieving functional independence with EVT is lower in large ischemic core patients due to the significant established tissue damage and perceived irreversible neurological deficits. Also, there is a higher risk of hemorrhagic transformation with reperfusion therapy in these patients. Thus, the risk-benefit ratio of EVT is not well established in LVO patients with large core. However, the natural history in this population is usually very poor with high risk of stroke progression, neurological worsening, hemorrhagic transformation, and ultimately death.
Stroke practices use different imaging modalities to triage patients for EVT. The definition of large core varies by the different triage imaging modalities. Early ischemic changes on non-contrast CT are measured using ASPECTS, a semi-quantitative measure, assessing tissue density.8 Perfusion imaging, on the other hand, assesses quantitative cerebral blood flow patterns to identify areas with critical blood flow deficits. MRI measures tissue water content to identify ischemic core, which can be measured in a semi-quantitative (ASPECTS) or quantitative (ischemic core size) manner.
Due to the limited direct evidence from randomized controlled trials (RCTs) assessing EVT efficacy and safety in large ischemic core patients, we sought to evaluate the current available evidence of EVT efficacy and safety in this population from sub-analyses of RCTs, pooled meta-analyses, and observational studies using a systematic review. Furthermore, we synthesized and compared thrombectomy outcomes in patients with large core based on the different imaging modalities using a meta-analytical approach.
Methods
Our meta-analysis adopted the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines (PRISMA) and is reported in accordance with the Meta-Analysis of Observational Studies in Epidemiology proposal.9 10 We used publicly available published studies, and our study was exempt for approval from the Institutional Review Board.
Criteria for studies' consideration
Database search
A total of three comprehensive scientific literature databases (PubMed, SCOPUS, and Medline) were searched to identify candidate studies using a pre-defined search strategy. Efforts were put in place to ensure similar representation of search terms across the databases. The database search was executed on 8 January 2020, limited to articles published on or before 1 January 2020. The search terms are provided in the online supplementary table 1. After removing duplicates, the studies were evaluated initially using abstract review, followed by full text review. Two authors (DP and FS) independently assessed the studies for inclusion in the systematic review and meta-analyses, with disagreement resolved by the third author (AS). The search strategy used for identifying the candidate studies is included in the online supplementary table 1. The search flow diagram according to the PRISMA guidelines is provided in figure 1 .9
Supplemental material
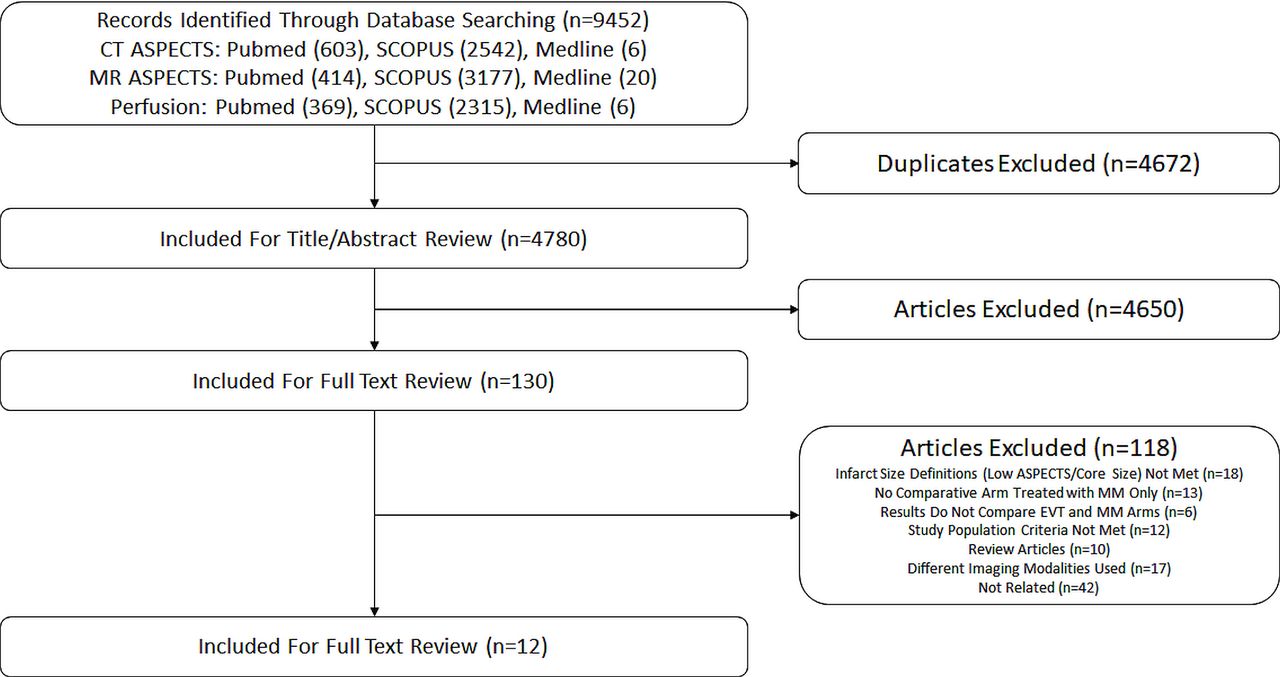
PRISMA flow diagram for studies included in the meta-analyses.
Selection criteria for the studies included in the systematic review and meta-analyses
We planned to review published studies from RCTs, their pooled meta-analyses, prospective and retrospective observational studies with description of outcomes in patients who received medical management only (MM) and MM plus EVT. For observational studies, cohort studies and case control studies were included in the review. The study population was limited to years 2009 and beyond. When two or more studies overlapped in population, all the studies were described for systematic review, but the study with largest population was included in the given meta-analysis. The selection criteria for the studies include: patients diagnosed with acute ischemic strokes; the study population consisted of large core stroke patients, either as the focus of the study or as a subpopulation; used semi-quantitative (ASPECTS <6) criteria on non-contrast CT or DWI or ischemic core ≥50 cc criteria on CT Perfusion imaging or MRI DWI to define large core strokes; reported rates of functional independence (mRS-scores of 0–2) at 90 days as well as at least one of two safety outcomes (symptomatic intracranial hemorrhage (ICH) and mortality at 90 days); and reported outcomes in patients based on the treatment they received separately; MM only and MM plus EVT. The MM group included also patients treated with intravenous thrombolysis.
Imaging modalities and large core definitions and thresholds
Studies using non-contrast CT, MRI using diffusion weighted sequences, and Perfusion imaging (both CT and MRI) for detection of stroke size were included. Assessment was initially obtained between studies using ASPECTS score and ischemic core volume definitions, respectively. Since some studies combined large core population on either CT/MRI DWI using ASPECTS score, both imaging modalities were allowed to assess thrombectomy outcomes. A combined analysis of studies using both definitions was also attempted.
Study outcomes
EVT outcomes were assessed using functional independence rates defined as modified Rankin Scale score of 0–2 at 90 days. Safety profile was assessed using symptomatic intracranial hemorrhage (sICH) and mortality at 90 days. The definition of symptomatic ICH was not pre-defined and was deferred to each individual study.11 12 To reduce potential heterogeneity between reported outcomes, studies reporting 90-day mRS of 0–3 or mRS 0–4 without reporting rates of functional independence (mRS 0–2) were not included.
Data quality
The Newcastle Ottawa Scale (NOS) was used to assess the quality of the studies included in the systematic review and meta-analyses. Two authors (DP and FS) independently assessed the quality of the studies, with disagreements resolved by a third author (AS).
Statistical analysis
The number of individual participants were considered the unit of analysis. Proportion of the participants as well as 95% CI were obtained for each outcome in each study cohort. Heterogeneity assessment was done using visual inspection of the confidence intervals on the forest plots, exploring for non-overlapping CIs. Eggar’s test was not performed due to the low number of studies included in the meta-analyses. Higgin’s I2 statistics were also calculated for each study cohort for all outcomes and interpreted in conjunction with the magnitude and direction of effects, and strength of evidence for heterogeneity. For a general guide, values≤40% were classified as heterogeneity not important, 30%–60% classified as moderate, 60%–90% substantial heterogeneity, and ≥75% classified as considerable heterogeneity. Cochran’s Q statistics were also reported. Bias assessment was completed using funnel plot. Pooled odds ratios (OR) were obtained using DerSimonian and Laird random-effects models for meta-analyses for pre-specified outcomes. RevMan 5.3 (Review Manager (RevMan) (Computer program). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014), and Stata 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC) were used for meta-analyses. All comparisons were two-sided and P<0.05 was considered statistically significant.
Results
Systematic review of studies assessing outcomes in large core stroke patients treated with EVT as compared to MM only
A total of 12 studies were included in the systematic review describing a comparison of EVT vs MM in patients with large core strokes.13–24 Of these, eight studies13 14 16–18 22–24 defined large core using ASPECTS score and five studies13 15 19–21 used ischemic core volume. A single study13 described large strokes using both ASPECTS score and ischemic core volume. Imaging modalities used to define large core also varied. In studies using ASPECTS score, one used CT only,13 one defined ASPECTS score using DWI only17, and five allowed a study population that were assessed using either modalities.14 18 22–24 One study did not specify the imaging modality used to assess the ASPECTS score.16 Similarly, three studies used ischemic core volume to define large stroke on CT Perfusion,13 15 19 while two used ischemic core on both CT Perfusion/DWI to define large core strokes.20 21 The characteristics of the studies as well as included patients and their outcomes, are described in table 1. Further inclusion and exclusion criteria for studies can be found in online supplementary tables 2 and 3.
Characteristics and reported outcomes for studies included in the systematic review
Quality assessment of the included studies
Online supplementary table 4 provides detailed assessment of the quality of the studies included in the systematic review, using the NOS. Two studies were completed as a secondary analysis of a prospective cohort,13 14 whereas three studies represented results from a retrospective cohort.16 17 20 Six studies represented patients with the large stroke only as the study cohort,13 14 16 17 19 20 whereas for six studies,15 18 21–24 results of patients with large stroke were not the focus and were presented as a subgroup analysis of a larger cohort including both small and large strokes. Overall, the analysis reported nine studies as having low risk of bias (9/9 in NOS)13 15 16 18 19 21–24 and three studies at moderate risk of bias (7-8/9 in NOS).14 17 20
Meta-analysis
Outcomes in large core defined as ASPECTS <6
A total of five studies describing outcomes with ASPECTS <6 were included in the meta-analysis.13 14 16–18 414 patients received EVT, whereas 583 received MM. The risk of publication bias was low based on visual inspection of the respective funnel plots (online supplementary figure 5). EVT was associated with significantly higher odds of functional independence at 90 days (EVT: 25% (101/414) vs MM: 7% (38/583), pooled OR: 4.29 [95% CI: 2.08 to 8.85], overall effect Z-score: 3.95, P<0.0001, I2=0.54, P for Cochran Q: 0.07), whereas the odds of sICH (EVT: 9% (35/409), MM: 5% (28/578), pooled OR: 1.66 [95% CI: 0.79 to 3.50], overall effect Z-score: 1.35, P=0.18, I2=0.40, P for Cochran Q: 0.16) were similar between the two groups. 90-day mortality was significantly lower with EVT (EVT: (20%) 75/362, MM: (30%) 173/537, pooled OR: 0.49 [95%CI: 0.36 to 0.68], overall effect Z-score: 4.25, P<0.0001, I2=0%, P for Cochran Q:0.45), figure 2. There was evidence of moderate heterogeneity across the included studies for the outcome of functional independence and sICH. There was no heterogeneity across the included studies for the outcomes of 90-day mortality.

Forrest plot comparing the unadjusted likelihood of (A) 90-day functional independence, (B) symptomatic ICH, and (C) 90-day mortality in patients with ASPECTS <6 between mechanical thrombectomy and medical management
Outcomes in large core based on ischemic core volume (≥50cc or ≥70 CC)
Four studies used ischemic core volumes to define large stroke,13 19–21 two with the threshold of 50 cc, whereas the other two used the 70 cc threshold. 139 patients received EVT and 195 received MM. Based on a random-effect meta-analysis, EVT was associated with higher odds of 90-day functional independence (EVT: 32/139 (23%), MM: 15/195 (8%), pooled OR: 3.76 [95% CI: 1.66 to 8.54], overall effect Z-score: 3.17, P=0.002, I2=18%, P for Cochran Q: 0.30) and lower 90-day mortality odds (EVT: 45/139 (32%), MM: 81/195 (42%), pooled OR: 0.60 [95% CI: 0.38 to 0.96], overall effect Z-score: 2.11, P=0.03, I2=0%, P for Cochran Q:0.85). Symptomatic ICH rates did not differ between the two groups (EVT: 11/115 (10%), MM: 18/173 (10%), pooled OR: 0.88 [95% CI: 0.38 to 2.05], overall effect Z-score: 0.29, P=0.77, I2=0%, P for Cochran Q:0.44), figure 3. There was no evidence of heterogeneity across included studies for all the outcomes of interest.
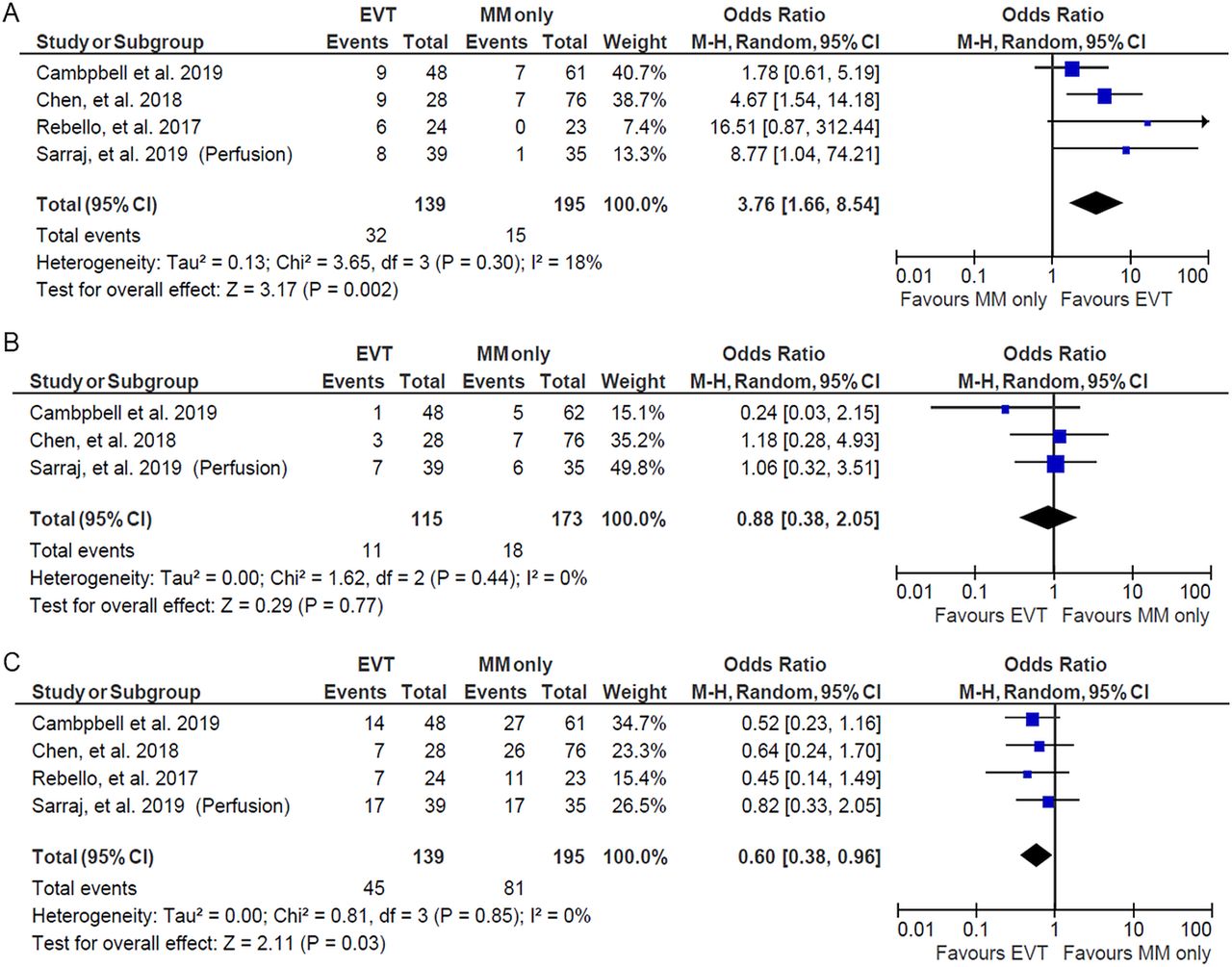
Forrest plot comparing the unadjusted likelihood of (A) 90-day functional independence, (B) symptomatic ICH, and (C) 90-day mortality in patients with ischemic core ≥50 cc between mechanical thrombectomy and medical management.
A combined analysis of EVT outcomes in patients with large core on ASPECTS or ischemic core volume or both
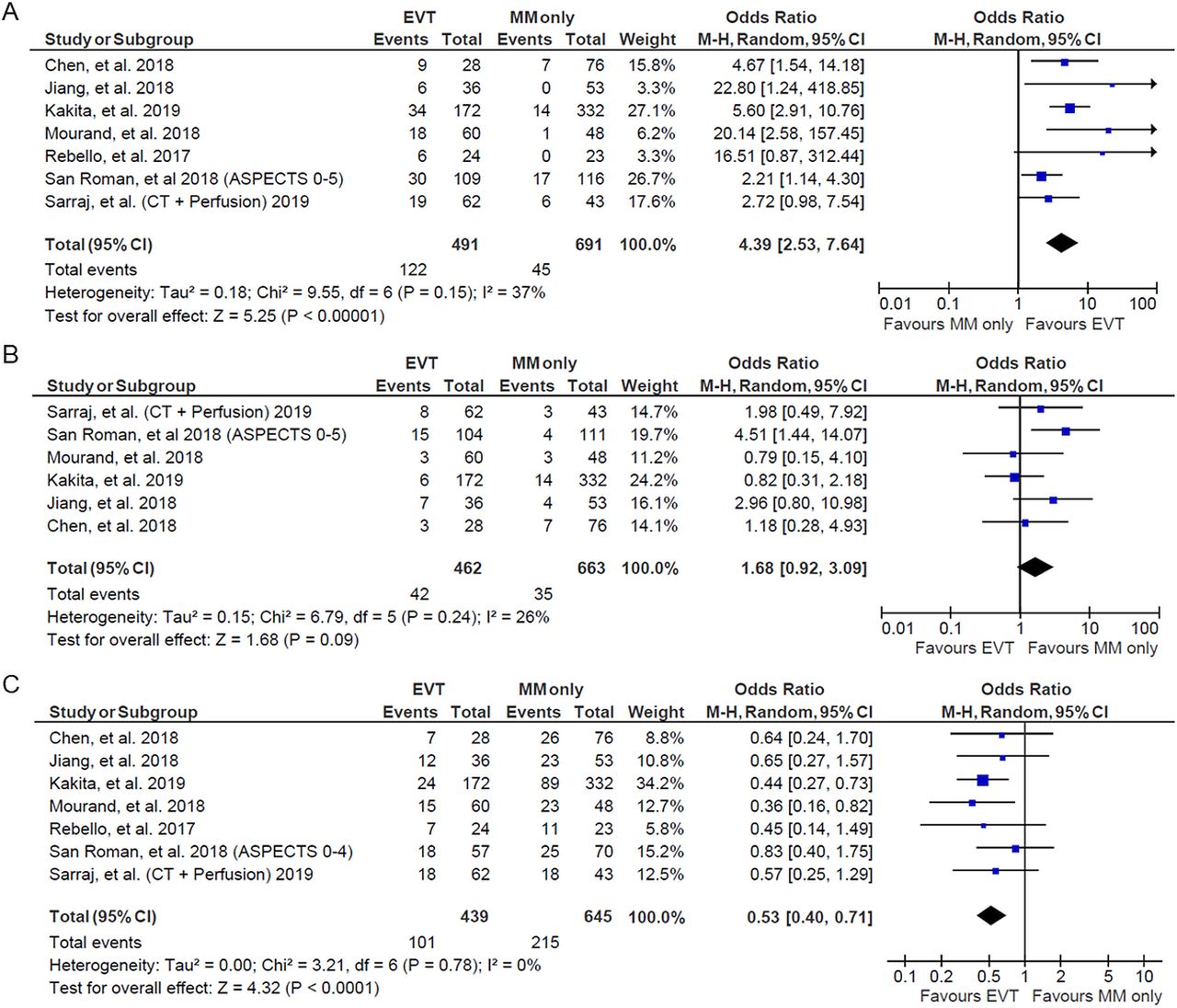
A combined random effect meta-analysis of all studies describing EVT outcomes in large stroke as compared with MM was also conducted. Since the HERMES meta-analysis reported data stratified based on both ASPECTS score and ischemic core volume,18 21 the study describing large stroke with higher sample size was used in the combined meta-analysis.18 491 patients received EVT and 691 received MM. Overall, EVT was associated with higher odds of 90-day functional independence (EVT: 122/491 (25%), MM: 45/691 (7%), pooled OR: 4.39 [95% CI: 2.53 to 7.64], overall effect Z-score: 5.25, P<0.00001, I2=37%, P for Cochran Q:0.15) and lower odds of 90-day mortality (EVT: 101/439 (23%), MM: 215/645 (33%), pooled OR: 0.53 [95% CI: 0.40 to 0.71], overall effect Z-score: 4.32, P<0.0001, I2=0%, P for Cochran Q:0.78). Symptomatic ICH rates were higher in the EVT arm, but the difference did not reach statistical significance (EVT: 42/462 (9%), MM: 35/663 (5%), pooled OR: 1.68 [95% CI: 0.92 to 3.09], overall effect Z-score: 1.68, P=0.09, I2=26%, P for Cochran Q:0.24), figure 4. There was no evidence of heterogeneity across included studies for all the outcomes of interest in the combined analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forrest plot comparing the unadjusted likelihood of (A) 90-day functional independence, (B) symptomatic ICH, and C) 90-day mortality in patients with ASPECT 6 or ischemic core ≥50 cc between mechanical thrombectomy and medical management.
A sensitivity analysis by including results reported by Campbell et al21 for large core outcomes on Perfusion imaging from the HERMES meta-analysis demonstrated similar effects on functional independence (EVT: 101/430 (23%), MM: 35/636 (5%), pooled OR: 4.54 [95% CI: 2.57 to 8.00], overall effect Z-score: 5.22, P<0.00001, I2=29%, P for Cochran Q:0.21), mortality (EVT: 97/430 (23%), MM: 217/636 (34%), pooled OR: 0.49 [95% CI: 0.37 to 0.66], overall effect Z-score: 4.76, P<0.00001, I2=0%, P for Cochran Q:0.96), and sICH (EVT: 28/406 (7%), MM: 36/614 (6%), pooled OR: 1.16 [95% CI: 0.65 to 2.05], overall effect Z-score: 0.51, P=0.61, I2=4%, P for Cochran Q:0.39), online supplementary figure 1. There was no evidence of heterogeneity across included studies for all the outcomes of interest in the sensitivity analysis.
Subgroup analyses: assessment of the effect of time, ASPECTS score, volume sizes, and IV thrombolysis on thrombectomy outcomes
Based on enrollment times, we divided the studies into those reporting enrollment up to 6, 12, and 24 hours from stroke onset/LKW. The results are presented in online supplementary figure 2. Overall, no statistically significant difference was observed in the odds of functional independence with EVT across the subgroups (P=0.86).
Subgroup analysis comparing functional independence in large core patients based on large core definition (ASPECTS vs ischemic core volume) excluded studies which used large core definitions using both ASPECTS score and ischemic core,13 or the study population had two studies published based on two different large core definitions (HERMES meta-analyses assessing ASPECTS score and ischemic core volumes).18 21 Overall, the test for subgroup differences failed to demonstrate statistical significance (P=0.65) (online supplementary figure 3).
Subgroup analysis based on different ischemic core definitions (ischemic core ≥50 cc and ≥70 cc, respectively) also failed to show significant differences (P=0.18, online supplementary figure 4).
There was no interaction between EVT and IV thrombolysis on functional independence rates (P for interaction=0.95, online supplementary table 5).
Assessment of publication bias
Overall assessment of publication bias using visual inspection of funnel plots demonstrated low risk of publication bias in both subgroups (ASPECTS<6 and ischemic core volume ≥50 cc) as well as overall combined analysis (online supplementary figure 5).
Discussion
Our systematic review identified 12 studies reporting outcomes in patients with large core strokes on CT, MRI DWI, or Perfusion imaging.13–24 Our findings were consistent across the different imaging modalities. Overall, EVT, as compared with MM, resulted in 4.5 times higher odds of functional independence and reduced mortality by half. The rates of symptomatic ICH, while not statistically significant, were reported to be higher in patients who were treated with EVT, especially in those with large core on Perfusion imaging.
Our results showed higher functional independence rates in patients with large core either by ASPECTS or ischemic core volume definitions, individually. Only one study reported outcomes based on both definitions individually,13 and the results were consistent with the pooled meta-analyses presented here. We further performed a subgroup analysis comparing outcomes between these two definitions and did not find significant heterogeneity in the results when large core strokes were defined based on ASPECTS or ischemic core volume.
Furthermore, there can be discordance between these imaging modalities with one showing large core (unfavorable profile) while the other does not show that but rather small core (favorable profile). Those patients with discordant profiles may account for a significant proportion of all LVOs with prospective cohort data suggesting higher functional independence rates with EVT.25 We could not pool outcomes on those discordant profile patients since all the studies, but one, did not report them.
Additionally, we assessed the effect of time on thrombectomy outcomes in subgroup analyses that did not show a significant heterogeneity between studies reporting <6 hours,<12 hours, and <24 hours treatment time windows. Prior studies have reported a decline in functional outcomes for EVT as time progresses in patients with large core strokes.13 This could be due to the fact that the later patients with large core present, it would be less likely for their neurological deficits to be reversed due to the already established significant infarcts.
Our results could be due to the fact that the studies presented in the meta-analysis included a majority of patients presenting in an early time window. Thus, the lack of difference in treatment effect in the two treatment windows may be due to the limited number of patients presenting beyond 6 hours of LKW, thus heterogeneity could not be detected. It is still plausible though that while the functional independence rates declined with time but EVT treatment effect may be preserved due to the decline in medical management outcomes, thus demonstrating no significant heterogeneity in outcomes as shown in our findings.
Whether the adjunctive benefit of EVT in the large core population extends up to 24 hours similar to the small core population remains to be seen. The ongoing large core RCTs are enrolling patients in different time windows SELECT2 (up to 24 hours), TESLA (up to 12 hours), TENSION (up to 11 hours), and IN-EXTREMIST (up to 6.5 hours)) which will allow for assessment of EVT outcomes and treatment effect in different time windows. Furthermore, the SELECT2 trial has an adaptive design based on treatment window (0–12 hours versus >12–24 hours) which will allow for enrollment enrichment in the earlier window should interim analysis show a lower likelihood of detecting adjunctive benefit as time progresses.
Similarly, no significant heterogeneity was observed in studies reporting outcomes in patients with ≥50 cc of ischemic core vs ≥70 cc of ischemic core. The number of patients with 50–70cc of baseline core infarct included in these studies may be limited, explaining the lack of heterogeneity between the studies. Prior reports suggested lower functional independence rates in large core strokes as the volume size increases and ASPECTS decreases.13 18 21
While prior studies have shown better outcomes with endovascular thrombectomy when advanced imaging selection modalities are used,3 5 26 our results showed no heterogeneity in potential treatment effect based on the different large core definitions on ASPECTS as compared with ischemic core volume on Perfusion imaging. It remains possible that using advanced Perfusion images may result in better estimation of the core infarct size and salvageable tissue. A recent comparative analysis of thrombectomy outcomes based on non-contrast CT vs CT Perfusion showed similar correlation of the two modalities with functional independence, however, patients with large core infarcts on CTP had higher rates of intracranial symptomatic hemorrhage and mortality with thrombectomy.25 Furthermore, another analysis of the large core population did not show heterogeneity of EVT treatment effect based on CT as compared with CTP.13 The ongoing SELECT2 trial will further investigate the role of imaging modalities for thrombectomy patients’ selection and if there was a heterogeneity in the outcomes based on the imaging findings on the different modalities. Furthermore, there are several ongoing RCTs assessing thrombectomy efficacy and safety in large core patients with different imaging modalities eligibility criteria (non-contrast CT, Perfusion, and DWI). Results from these trials will allow for a comparison of EVT outcome in large core patients based on advanced vs conventional neuroimaging modalities.
Since the studies in our meta-analyses did not report ischemic core size or ASPECTS subgroups, we could not assess for the effect of increasing core size on EVT outcomes. Similarly, prior reports have suggested a potential ceiling effect with thrombectomy, with studies reporting potential lack of benefit beyond 100 cc and 150 cc.13 21 We could not assess for an upper core volume limit for better outcomes with EVT in this meta-analysis, since the majority of the included studies did not describe those.
We observed lower rates of functional independence with EVT (25%) as compared with the prior thrombectomy RCTs that showed functional independence rates ranging from 33%1 to 70%,5 with a 47%23 overall functional independence rate in the HERMES early window meta-analysis and 44%,7 and 49%6 in the late window trials. These lower functional independence rates are probably a product of EVT being performed in patients with larger areas of infarcted tissue as compared with patients enrolled in prior EVT RCTs since the vast majority of these patients had smaller infarcts (ASPECTS>5, core infarct size <50 cc mostly). However, the functional independence rates with best medical management were much lower (6.5%), suggesting very poor prognosis in patients who received the current standard of care.
Our results may have also been affected by disproportionate IV thrombolysis rates in both treatment arms. However, we could not perform a comprehensive assessment of IV tPA effect on EVT potential benefit since only four studies reported IV tPA proportions with a sole study reporting functional independence odds stratified by thrombolysis status. Still, however, there is a possibility that IV tPA may have a confounding effect on EVT outcomes. Subgroup analyses from the ongoing large core RCTs would shed light on this subgroup.
There are several ongoing randomized-controlled clinical trials to assess EVT efficacy and safety in large core patients. These trials use different imaging modalities and inclusion criteria (TENSION: ASPECTS 3–5, TESLA: ASPECTS 2–5 or MRI DWI volume 70–120 cc, IN-EXTREMIST MOSTE MRI DWI ASPECTS 0–5). The SELECT2 trial is assessing thrombectomy efficacy and safety in patients with large core either on CT (ASPECTS 3–5) or Perfusion imaging [(rCBF <30% or MRI ADC<620)≥50 cc] with an assessment of the effect of different ischemic core volumes cutoffs and reperfusion time on thrombectomy treatment effect. The trial is also evaluating if there is heterogeneity in thrombectomy treatment effect as related to CT and Perfusion imaging profiles.
Our study has several limitations. The data represented different study designs: prospective, retrospective, and post-hoc analyses from RCTs. However, there was limited heterogeneity across the included studies. We only included studies that evaluated outcomes in patients treated with both EVT and MM, but it should be noted that there was no randomization across the two groups, and our findings may be subject to selection bias. Even in the data from RCTs' post-hoc analyses, these trials were not designed to specifically assess the large core subpopulation patients. Also, mixing large core outcomes on different imaging modalities is not ideal but this is a representation of real-life practice. While we did not find heterogeneity in thrombectomy outcomes between studies reporting large cores on CT as compared with MRI or Perfusion imaging, our findings still do not determine whether there is a superiority for large core assessment on one imaging modality versus the other. Definitions of large core, both quantitative (ischemic core volume) and semiquantitative (ASPECTS) may represent different degrees of ischemic core on CT and MRI, however, most of the reported studies considered the definitions on both modalities together to define their study populations. Since different imaging modalities and different large core definitions represent different patient populations, looking at large core as a homozygous stroke population may not be accurate. Results of the aforementioned RCTs will also help us better understand the correlations and effects of stroke sizes on different imaging modalities.
While ischemic core definitions were assessed from Perfusion imaging, the ischemic penumbral profile was not evaluated in the study and may have an impact on the outcomes in these patients. Finally, we evaluated unadjusted associations between treatment modality (EVT vs MM) and outcomes as we did not have patient level data for this meta-analysis. An individual patient data meta-analysis would be more appropriate to clarify whether EVT is superior to MM in patients with large ischemic stroke after adjustment for numerous potential confounders.
In conclusion, the present meta-analysis is the largest to date to provide comparison of clinical and imaging outcomes between LVO patients with large infarct core that have been treated with either EVT or MM. The results demonstrate that EVT may provide adjunctive benefit in patients with large core strokes as measured by different modalities with different definitions. Randomized-controlled clinical trials to assess EVT efficacy and safety in patients with large core strokes based on various definitions are ongoing and should provide a definitive answer to this important clinical question.
References
Footnotes
Twitter @amrsarrajMD, @Faris_Shaker
Contributors Concept and design: Sarraj. Acquisition, analysis, or interpretation of data: Sarraj, Pujara, Shaker. Drafting of the manuscript: Sarraj. Critical revision of the manuscript for important intellectual content: Sarraj, Grotta, Pujara, Shaker, Tsivgoulis. Statistical analysis: Pujara, Tsivgoulis. Obtained funding: N/A. Administrative, technical, or material support: Sarraj. Supervision: Sarraj.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.