Article Text

Statistics from Altmetric.com
Introduction
Endovascular treatment (EVT) is a safe and effective therapy for acute ischemic stroke caused by large vessel occlusion.1–3 It is highly time-dependent, and even small reductions in treatment delays can lead to notable improvement in patient outcomes: a 20 min decrease in time-to-treatment translates into an average gain of 3 months of disability-free life.4 Simple changes in in-hospital workflows such as pre-notification of the medical team, registering the patient as unknown, limiting non-essential interventions in the emergency department (ED) and bypassing of the CT scanner can substantially decrease time to treatment.5–7 Avoiding general anesthesia can further reduce treatment delays.8 However, EVT has only become standard of care recently, and workflow processes in many centers might not be fully optimized yet. There is no standardized way to measure workflow efficiency, and conducting systematic studies on this topic is therefore difficult. It is, however, of utmost importance to identify areas with potential for time-savings, since they can serve as a starting point for efforts to minimize treatment delays. In this study, we used a survey-based approach to explore how endovascular stroke treatment processes are currently structured across different countries and hospital settings, and to evaluate how workflow efficacy could be improved.
Methods
A web-based survey (Qualtrics.com) was conducted at a major neurointerventional meeting (Advanced Live Interventional Course of Essen 2020, Essen, Germany) involving a multinational neurointerventional audience to determine current workflow patterns in acute ischemic stroke treatment.9 In the first part of the survey, participants were asked to provide their demographic baseline characteristics (age, gender, specialty, career stage, years of experience, personal and institutional thrombectomy caseload, institution’s catchment population, number of physicians taking neurointerventional calls). In the second part, physicians were asked specific questions about the stroke workflow characteristics in their department and provided an estimate for the time saving (in minutes) that could be achieved by optimizing/implementing a solution for this particular step in the workflow. The survey link was sent out to all registered meeting participants and additional selected neurointerventionalists in Europe and North America 48 hours before the meeting. Response data were obtained from November 4 to 28, 2019. Survey data were summarized using descriptive statistics. Differences between subgroups were assessed with a χ2 test, and differences in the distribution of continuous variables with the Wilcoxon rank-sum test. Subjective estimates of time-savings for particular workflow steps were compared with reported time-savings in the literature. Two-sided p values <0.05 were considered statistically significant. All analyses were performed in Stata 15.1. Figures were created in Microsoft PowerBI 2016 using the Visualmapbox plugin. Consent was obtained from all survey participants before the start of the survey, and participation was voluntary. Since no patients were involved, ethics approval was not necessary for this study.
Results
Out of 327 physicians who received survey invitations, 248 physicians from 48 countries participated and completed the survey (response rate 75.8%). The participants’ demographic baseline characteristics are shown in online supplementary table 1.
Supplemental material
Subjective estimates of potential time savings and comparison with the literature
Physicians’ subjective estimates of potential time-savings that could be achieved through optimization of particular steps in the acute stroke treatment workflow (implementation of pre-notification tools, streamlining ED workflows, optimizing the spatial setup of the department, all-time availability of anesthesia in the angiography suite, use of a pre-prepared stroke kit) ranged from 13 min for the use of a pre-prepared stroke kit to 19 min for pre-notification tools. Table 1 compares physicians’ estimates with the time-savings that have been reported in the literature.
Physicians’ estimated time-savings that can be achieved through optimization of particular workflow steps in comparison with time-savings reported in the literature
Pre-hospital workflow: pre-notification of the neurointerventional team
Overall, 70% of the participants stated that they use a pre-notification tool, with slight differences across specialties and countries that did not reach statistical significance (p>0.05, respectively, figure 1).

Use of tools to pre-notify the neurointerventional team for acute stroke treatment overall (lower right corner). and for different countries. Circles represent responses from individual institutions. Yellow color indicates no use of pre-notification tools, while green color indicates that pre-notification is used in a particular institution. Please note that Europe has been magnified in this illustration.
Intra-hospital workflow: emergency department
When asked which steps are currently performed in an acute stroke patient in their ED before EVT, 24/183 (13.1%) of the physicians stated that they completely bypass the ED and transport the patient directly to the angiography suite by default for all stroke patients. Vital parameters were assessed in the ED in 77.6% (77/183) in the participants’ current local setting, patient registration was performed in 76.0% (139/183), an intravenous line was inserted in 74.9% (137/183), and the clinical history was taken in 74.3% (136/183). Blood samples were routinely taken in 61.2% (112/183), an electrocardiogram (ECG) was performed in 26.2% (48/183), a Foley catheter inserted in 6.0% (11/183), and a chest x-ray obtained in 3.8% (7/183).
Intra-hospital workflow: spatial setup
Online supplementary figure 1 illustrates the spatial location of the ED, CT scanner and angiography suite in relation to each other in participants’ current local hospital setup: 23% of the participants stated that the ED and the CT scanner were on different floors in their hospital; and 38% of the participants stated the CT scanner and angiography suite were on different floors. Location of the ED relative to the CT scanner, and the CT scanner relative to the angiography suite, differed neither significantly across countries nor between physicians affiliated to interventional neuroradiology, neurosurgery and neurology (p>0.05).
Supplemental material
Intra-hospital workflow: anesthesia protocol
Overall, 42.5% (76/179) of the physicians used general anesthesia as a default for EVT in their current local setting, followed by conscious sedation (61/179, 34.1%), and 23.5% (42/179) did not routinely use anesthesia or sedation at all. Figure 2 provides an overview of the default anesthesia protocols in different countries. The protocols used did not differ significantly across specialties (p>0.05) but we observed significant variations across countries (p=0.018, figure 2). The majority of physicians who used general anesthesia or conscious sedation (97/118, 82.2%) had an anesthesiologist available at all times in the angiography suite.

Default anesthesia protocol for thrombectomies used by survey participants overall (right upper corner) and by country. Red color indicates general anesthesia, orange color indicates conscious sedation and yellow color indicates that neither is used by default. Circle sizes are proportional to the number of respondents from each country. Please note that Europe has been magnified in this illustration.
Intra-hospital workflow: thrombectomy procedure
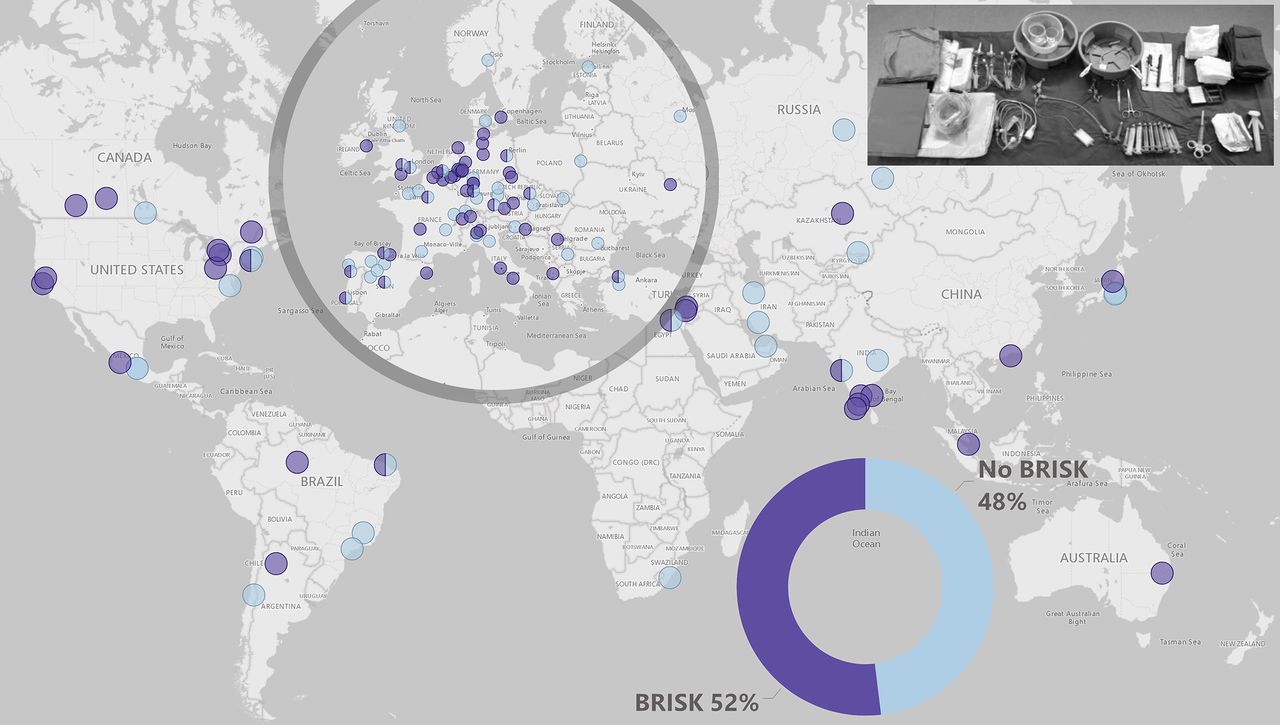
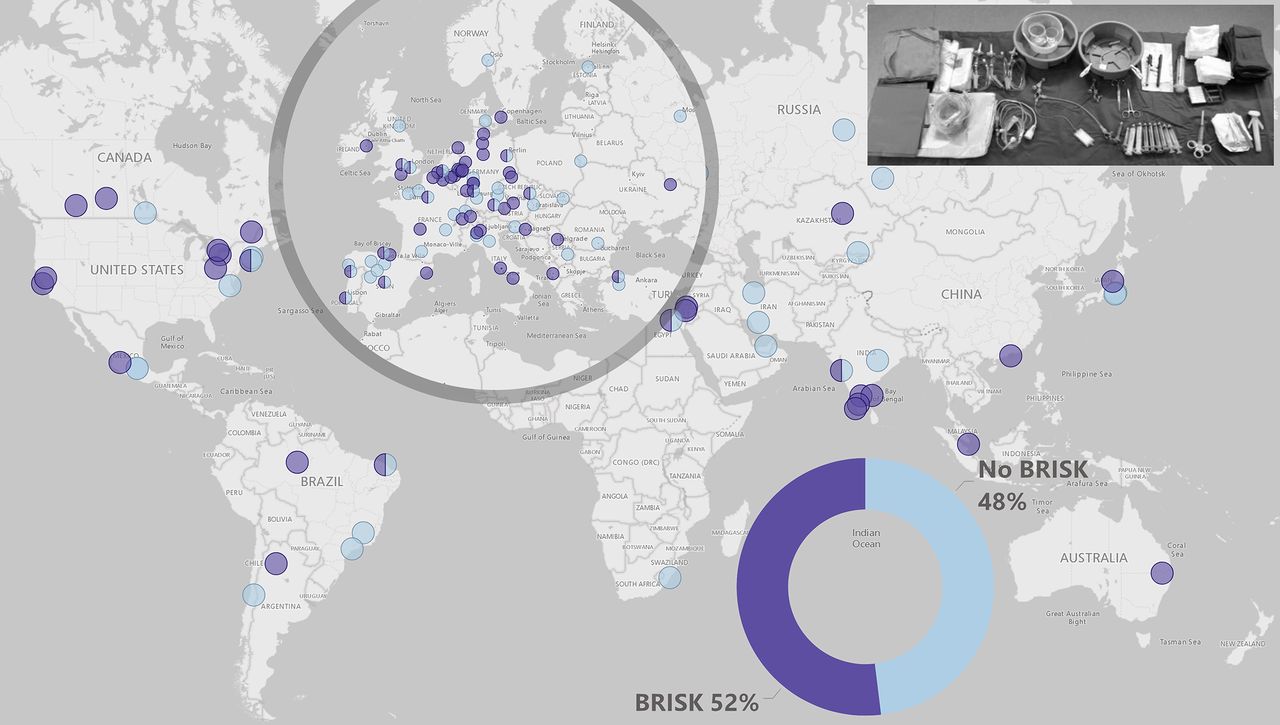
Overall, 52% (93/179) of the respondents routinely used a pre-prepared stroke thrombectomy kit such as BRISK (Brisk Recanalization Ischemic Stroke Kit) that contains the necessary thrombectomy equipment such as needles, syringes and hemostatic valves.10 Figure 3 shows the utilization of a pre-prepared thrombectomy kit across different specialties and countries. The differences across specialties and countries did not reach statistical significance (p>0.05, respectively). There was no association between the use of a pre-prepared kit and age, career stage and individual physicians’ personal annual endovascular stroke treatment volume (p>0.05, respectively). There was, however, a significant association between institutional annual EVT volume and use of a pre-prepared kit (p=0.047): physicians working in centers with an annual volume <10 thrombectomies used a pre-prepared kit least commonly (4/12, 33.3%), while among the physicians working in centers with >100 thrombectomies per year, >50% routinely used a pre-prepared kit.
{kind=link}
{kind=link}
{kind=link}
Utilization of a pre-prepared thrombectomy kit (BRISK) overall (right lower corner) and by country. Circles represent responses from individual institutions. Light blue color indicates no utilization of a pre-prepared thrombectomy kit, while dark blue color indicates that a pre-prepared kit is used in a particular institution. Please note that Europe has been magnified in this illustration. BRISK, Brisk Recanalization Ischemic Stroke Kit.
Discussion
In this survey, we explored in detail how endovascular stroke treatment processes are currently structured in different countries and hospital settings, and the magnitude of potential time-savings that could be achieved through optimization of different workflow aspects. A comparison with the literature revealed that, except for pre-notification tools, survey paticipants generally underestimated the potential time-savings that could be achieved through optimization of particular workflow steps (table 1). Several bottlenecks to rapid EVT treatment have emerged, such as unnecessary procedures (ECG, chest x-rays) in the ED, or preparation times for thrombectomy equipment.11 In theory, there are solutions to overcome all of these; for example, parallel processing could shorten patients’ length of stay in the ED, and pre-prepared stroke kits minimize the time needed to sort EVT equipment.10 However, while some of these solutions have been successfully established and sustained in competitive environments in which workflow metrics are publicly presented and discussed, implementation in most clinical settings where this is not the case is often lagging behind.12 Several studies have described the possibilities for and impact of workflow optimization in acute stroke treatment. Most analyzed data are from clinical trials or academic centers with high caseloads, and less is known about the potential for stroke treatment workflows in smaller community hospitals.5 8
Pre-notification of the medical team, and particularly the neurointerventionalist, for example, through a phone-call or an app, has been proven to reduce treatment delays.13 However, in a large North American registry study, pre-notification occurred only in approximately two thirds of all stroke patients, and this number varied widely across hospitals.14 Our results match these findings and highlight the potential for optimization. Pre-notification was used by 70% of the survey participants, with slight, non-significant variations across specialties and countries. Centers which did not yet use pre-notification should be encouraged to do so by their physicians and local policymakers, since this is a relatively easy and inexpensive way to reduce treatment delays.
It is well-known that inefficient workflows and unnecessary procedures in the ED delay acute stroke treatment. We asked physicians which procedures are routinely performed in their ED in acute stroke patients. In the majority of cases, blood samples were taken, an ECG was obtained in 26%, a Foley catheter inserted in 6% and chest X-rays performed in 3.8%. This clearly shows the need to cut back on redundant procedures—obtaining a routine chest X-ray before EVT, for example, does not have any consequences but unnecessarily delays treatment, thereby compromising patient outcomes. Only a minority of the physicians stated that they completely bypass the ED. This is a commonly used concept in the treatment of ST elevation myocardial infarction in many hospitals. If the clinical and ECG findings are unambiguous, the patient is taken to the cardiac catheterization laboratory straight away. EVT has now become standard of care for large vessel occlusion strokes; it is therefore possible that more hospitals will set up a similar process for acute stroke, in which the patient is taken directly to the neuroangiography suite if the likelihood of a large vessel occlusion is high, or if a large vessel occlusion is known because of prior imaging at a smaller community hospital or in a mobile stroke unit.
Most hospitals were built in the pre-EVT era, and the spatial setup might not be optimized for EVT. The ED, which is where stroke patients are usually admitted, is often not close to the CT scanner, where imaging is performed, and the neuroangiography suite, where the patient is finally treated, might be somewhere else altogether. In our survey, the ED and CT scanner were located on different hospital floors in 23%, and the CT scanner and neuroangiography suite in 38%—that is, most stroke patients had to change hospital floor at least once during the course of their treatment. While this problem cannot be immediately solved, it is an obvious planning consideration when hospital buildings are built or renovated. Location of the ED, CT scanner and neuroangiography suite close by each other could most likely reduce treatment delays, for example, due to waiting times at elevators.
Anesthetic management of EVT patients is currently a controversially discussed point. While some studies indicate that the utilization of general anesthesia is associated with time delays and worse clinical outcomes, smaller single-center randomized trials have reported non-inferior outcomes with general anesthesia.8 15–18 Regardless, it is clear that suboptimal anesthesia workflow results in time delays.8 Particularly long waiting times can result if general anesthesia is used but an anesthesiologist is not available in the angiography suite by default. In our survey, general anesthesia was used as a default protocol by the majority of physicians (42%), and 82% stated that they have an anesthesiologist available in the angiography suite at all times for this purpose. Given the high reported rate of anesthesia utilization, it is worthwhile investigating whether in some cases general anesthesia could be abandoned, thereby allowing for faster initiation of the thrombectomy procedure. If not, an all-time available anesthesiologist seems indispensable to avoid delays.
We have long advocated for a pre-prepared stroke kit (BRISK) that contains the basic equipment needed for thrombectomy.10 Only 52% of the survey participants stated that they currently use such a kit. Pre-prepared stroke kits are relatively inexpensive and simple to implement, but can reduce thrombectomy preparation time very effectively. Thus, in centers in which pre-prepared stroke kits are not already used, a discussion on whether to do so should be initiated with the members of the stroke team.
Limitations
Our study has several limitations. The vast majority of participants were neurointerventionalists, and the perspective of other non-interventional specialties involved in stroke care was not broadly represented. Most of the participants were European while the number of participants from certain other countries such as the USA was low. The generalizability of our results to other regions is therefore limited. Survey results are able to provide an overview about current workflow patterns but they cannot cover every detail in depth; the specific reasons why some potential solutions have not been implemented in certain hospital settings, for example, have not been captured in this survey. Most importantly, the subjective estimated time-savings for particular workflow steps were based on the physicians’ personal opinions; they therefore lack objectivity and are of limited validity. This methodology of assessing workflow efficiency is not ideal; objective workflow assessment would require large and detailed prospective registries, which are difficult to maintain and often succumb to selective reporting bias. We therefore think that, despite its limitations, our study provides important information on how endovascular stroke treatment is structured around the world and offers possible starting points for individual institutions to improve their workflow efficacy.
Conclusion
Our survey results highlight the potential for optimization of endovascular stroke treatment workflows in different countries and hospital settings. While some bottlenecks require structural changes and cannot easily be resolved, other easy-to-implement measures, such as pre-notification tools, elimination of unnecessary procedures in the ED and pre-prepared stroke kits, could help to decrease workflow times and thereby improve patient outcomes.
Acknowledgments
The authors are most grateful to all survey participants.
References
Footnotes
Twitter @johanna_ospel, @AlmekhlafiMa, @mihill68
Correction notice Since the online publication of this article, the authors have noticed that affiliation 8 'Neurology, University of Minnesota, Minneapolis, Minnesota, USA' is incorrect. Affiliation 8 has now been corrected to 'Valley Baptist Medical Center, Harlingen, TX, USA'
Contributors MG: conceptualization, drafting and critical revision of the manuscript. JMO: drafting and critical revision of the manuscript and figures. NK: drafting of the figures, critical revision of the manuscript. RC: data curation, critical revision of the manuscript. Remaining authors: critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on these maps does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The maps are provided without any warranty of any kind, either express or implied.
Competing interests MG is a consultant for Medtronic, Stryker, Microvention, GE Healthcare, Mentice. JMO is supported by the University of Basel Research Foundation, Julia Bangerter Rhyner Foundation and Freiwillige Akademische Gesellschaft Basel.
Patient consent for publication Not required.
Ethics approval Since no patient data were used for this study, ethics approval was not required. Consent from the survey participants was obtained before completing the survey.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.