Article Text

Abstract
Background The transradial approach (TRA) is frequently used for neurointerventional procedures as it is safer, improves patient comfort, and decreases costs and procedural time in comparison with the transfemoral approach (TFA). Patients with arteria lusoria, or an aberrant right subclavian artery (ARSA), provide a unique challenge for cerebral angiography and interventions when using the TRA.
Objective To examine the hypothesis that the extreme angulation encountered while accessing the great vessels from the right TRA could be overcome by reversing the approach to the left distal TRA (dTRA).
Methods A prospectively maintained database of transradial neurointerventional cases since 2018 was searched. Six cases from 850 were identified, in which the left dTRA was used. Three cases were for patients with an ARSA. For the three cases of interest, patient history, pathology, imaging, and access techniques were reviewed.
Results Two diagnostic cerebral angiography cases and one intervention were successfully performed through a left dTRA.
Conclusions Proper positioning of the left wrist and familiarity with forming the Simmons catheter can overcome this anatomical challenge. This technique and results further demonstrate that the left distal radial artery is a feasible access site for catheterization of bilateral carotid, left vertebral, and right subclavian arteries for patients with an ARSA.
- angiography
- intervention
- technique
Statistics from Altmetric.com
Introduction
The transradial approach (TRA) has recently emerged as a feasible alternative for neurointerventional procedures as it has been shown to be safer, improve patient comfort, and decrease costs and procedural time in comparison with the traditional transfemoral approach (TFA).1 In the majority of cases, the right radial artery is the preferred access site rather than the left radial artery given operator preference and traditional angiography suite layouts. In certain congenital anatomic variations such as arteria lusoria, also known as aberrant right subclavian artery (ARSA), it is challenging to access the great vessels through the right TRA.
In the majority of patients, the right subclavian artery arises from the brachiocephalic trunk, the first major vessel off the aorta. In patients with an ARSA, the right subclavian artery is the last great vessel to arise from the aorta. This variant, seen in 0.5–2% of the population, is known to cause catheterization problems during the right TRA. The aberrant artery takes a retro-esophageal (or less commonly, retro-tracheal) route towards the right and resumes its normal course as a lengthier and more tortuous right subclavian artery (figure 1A).2 3 It proceeds distally towards the right upper extremity, where it continues as the axillary, deep brachial, and brachial arteries. At the elbow, the brachial artery then normally bifurcates into the ulnar and radial arteries.2 4 5 In neurointerventional cases, the ARSA poses a unique challenge when attempting to catheterize the great vessels through the right TRA. Other than catheterization problems, ARSA may cause dysphagia in 20–40% of patients, more commonly affecting the pediatric and geriatric populations.6–8 Bayford first reported this anatomical variant in 1789 as a 'lusus naturae' ('jest of nature') in a case of 'obstructed deglutition' or as he coined it, 'dysphagia lusoria'.3 9
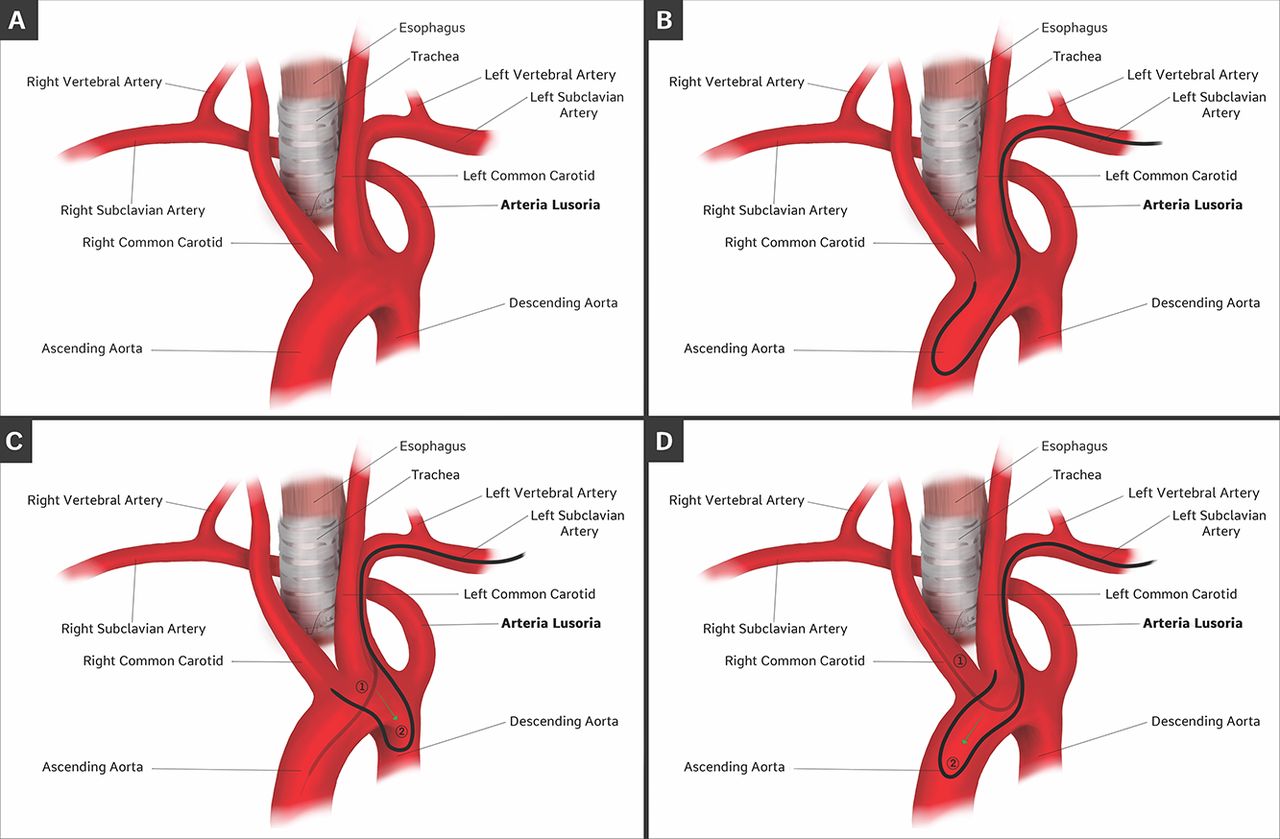
Shown is the arteria lusoria (aberrant right subclavian artery; ARSA) anatomical variant. (A) The various branches coming off the aortic arch are labeled. The ARSA typically courses left to right, as the last major branch. It typically courses behind the trachea and esophagus. (B) One way to form the catheter is by bouncing the wire off the aortic valve back onto itself and advancing the catheter over it. (C) The catheter can also be formed by retracting the wire back proximal to the elbow of the catheter and then advancing the catheter into the descending aorta. (D) The right common carotid artery can be directly accessed with the wire. Once the catheter is advanced into the right common carotid artery, the wire can be pulled back proximal to the catheter elbow, and the catheter can be pushed down into the ascending or descending aorta.
Traditionally, when this variant is encountered for neurointerventional procedures, conversion to the TFA is required. Publications have discussed patients with an ARSA undergoing coronary angiography, but the left TRA for neurointerventional procedures in these patients has not been described. We hypothesized that we could overcome the extreme angulation encountered while accessing the great vessels from the right TRA by reversing our approach to the left distal TRA (dTRA). We present the first reported case series of patients with an ARSA undergoing the left dTRA for neurointerventional procedures. We also provide details of our technique and nuances for this useful approach.
Methods
At our tertiary-care institution, we have an institutional review board-approved prospectively maintained database of all neurointerventional cases using the TRA since its implementation in 2018. From of a total of 850 cases, we identified six in which the left dTRA was used. Three cases were for patients with an ARSA. For the three cases of interest, patient history, pathology, imaging, and access techniques were reviewed.
Illustrative cases
Procedural technique
In all cases, either conscious sedation (diagnostic angiograms) or general anesthesia (interventions) was used. The patients were positioned supine on the angiography table with the left arm crossed over the abdomen near the right femoral artery access site.10 With the use of padding under the elbow, the left wrist was elevated and placed in a neutral position for distal left radial access (figure 2). We used the dTRA as opposed to the proximal TRA on the left as the dTRA allows the wrist to be positioned in a more natural and ergonomic position. The distal radial artery was measured with an ultrasound to ensure that the sheath to radial artery ratio was equal to or greater than 1, and that the artery was at least 2 mm so that a 5Fr or 6Fr sheath could be used. Once the puncture site was identified with ultrasound guidance, approximately 2 mL of 1% lidocaine was injected into the subcutaneous tissue. The left distal radial artery was then cannulated through the anatomic snuffbox with a single anterior wall puncture technique. A 5Fr or 6Fr sheath was placed and secured. A radial artery 'cocktail' containing 2.5 mg of verapamil and 200 g of nitroglycerin was administered through the sheath. A bolus of 70 U/kg of heparin was given through the intravenous route to maintain an activated clotting time of between 250 and 300 s in all interventional cases. A left radial artery angiogram was obtained in order to visualize both the caliber and the course of the radial artery, ensuring that there were no loops or vasospasm.

The left wrist is positioned across the abdomen in a neutral position as close as possible to the right femoral artery access site. (A) Prior to the start of the procedure, the left arm is brought across the abdomen. Additional padding can be placed under the left elbow and upper arm to facilitate bringing the arm across the abdomen. (B) This image demonstrates the angle of cannulation for the operator. The distal transradial approach is much easier to perform from the right side than the conventional proximal transradial approach as the arm can be left in a neutral position.
In the diagnostic cases, we used a 5Fr Simmons-2 Glidecath catheter (Terumo, Somerset, New Jersey, USA) over an 0.35” glidewire (Terumo- Somerset, New Jersey, USA). In the interventional case, we used a Benchmark 071 catheter (Penumbra, Alameda, California, USA) over a 5Fr Simmons Select catheter (Penumbra, Alameda, California, USA) over an 0.35” glidewire.
After advancing the wire and catheter combination into the ascending aorta, we turned our attention to shaping the Simmons catheter, which can be done in a number of ways. The catheter can be formed over the aortic valve as is commonly done with the right TRA by advancing the wire into the ascending aorta and bouncing it off the aortic valve so that the wire travels back towards the supra-aortic vessels. The Simmons catheter can then be advanced over the wire until it assumes its formed shape (figure 1B). The catheter can also be formed by advancing the wire and catheter combination into the ascending aorta, pulling back the wire proximal to the catheter curve, and advancing the curve into the descending aorta (figure 1C). The third way of forming the Simmons catheter is by directly catheterizing the right common carotid artery with the wire followed by the catheter. Next, the wire is pulled back proximal to the curve of the Simmons catheter. The catheter can then be pushed, with the curve falling into either the ascending (figure 1D) or descending aorta.
Once the catheter was reshaped, the desired vessels requiring angiography were catheterized. After completion of the procedure an external compression band (Merit, South Jordan Utah, USA) was applied over the left distal radial puncture site with a pulse oximeter on the left thumb. The sheath was removed under radial band compression to achieve patent hemostasis.
Case 1
A young middle-aged patient with a past medical history of moyamoya syndrome, sickle cell disease, and previous ischemic strokes between 2000 and 2013 presented to our institution with a transient ischemic attack. Multifocal areas of high-grade stenosis/vessel occlusion in the anterior circulation were observed on non-invasive imaging. Diagnostic cerebral angiography was performed in order to evaluate the patient’s cerebral vasculature and potential candidacy for cerebrovascular bypass surgery.
As non-invasive imaging had already demonstrated an ARSA, the left distal radial artery was accessed for the diagnostic angiogram. We used the same preparation and access techniques we normally employ in our right transradial access cases.
Diagnostic angiography of bilateral internal and external carotid arteries and the left vertebral artery revealed bilateral stenoses of the terminal internal carotid arteries (ICAs), and extensive collateral formation via pericallosal and pial collaterals from posterior cerebral arteries to the anterior circulation. The patient tolerated the procedure well without any immediate or delayed complications.
Case 2
A young middle-aged patient with no significant past medical history was found to have a right ICA para-ophthalmic bilobed aneurysm and an ARSA on non-invasive imaging. The patient was brought to the endovascular suite for aneurysm embolization. The same technique as described earlier was used, and the left distal radial artery was accessed.
In this case a 6Fr sheath was placed. A Benchmark 071 catheter was used as the guide catheter over a 5Fr Simmons Select catheter, which was advanced over a 0.035” wire. After shaping the catheter, the wire and catheter combination was then navigated into the proximal right ICA (figure 3). The aneurysm was identified and a Pipeline flow diverting stent (Medtronic, Minneapolis, Minnesota, USA) was deployed. The patient tolerated the procedure well with no immediate or delayed complications.

{kind=link}
{kind=link}
{kind=link}
Unsubtracted anteroposterior image demonstrating the wire catheter combination traveling from the left subclavian artery to the right internal carotid artery through a left distal transradial approach.
Case 3
A middle-aged patient with a history of pseudotumor cerebri, ventriculoperitoneal shunt, and previously treated left transverse-sigmoid Cognard III dural arteriovenous fistula presented for a follow-up diagnostic cerebral angiogram. As the fistula was treated at an outside institution, we had no preoperative imaging of the neck to evaluate the vascular anatomy.
First, the right distal radial artery was accessed. After the catheter was advanced into the right subclavian artery, the patient was found to have an ARSA. We then converted to the left dTRA after repositioning the left arm and prepping the left distal radial access site. The previously mentioned techniques for left dTRA were used, and the catheter was shaped, and the bilateral internal and external arteries and left vertebral artery were catheterized. Angiography demonstrated complete obliteration of the dural arteriovenous fistula. The patient tolerated the procedure well, with no immediate or delayed complications.
Discussion
Although an ARSA is found in a very small percentage of patients undergoing neurointerventional procedures, our experience demonstrates that the left dTRA is a feasible alternative to the TFA in this population. Over the past few years, the TRA has become the preferred route for neurointerventional procedures at many high-volume academic centers due to reduced vascular complications, greater patient comfort, and improved cost-effectiveness in comparison with the routinely used TFA.11 While femoral access is still routinely used at most centers for neurointerventional procedures, studies show that patients prefer the TRA.12–14 Our institution has adopted the 'radial first' approach because of the many benefits mentioned above.
In most cases, the right radial artery can be accessed to catheterize bilateral common carotid and vertebral arteries.15 An important factor which may provide favorable outcomes for patients undergoing the TRA is a preprocedural assessment of neck vasculature. Non-invasive imaging using a CT angiography/MR angiography of the neck can assist in planning for a left-sided approach in advance, rather than having to cross over mid-procedure, as described in one of our cases. Prior knowledge of any anatomic abnormality which may argue against the right TRA, including an ARSA, is helpful, especially early on when first transitioning to the TRA.
As mentioned earlier, successfully catheterizing the supra-aortic arteries, mainly the bilateral common carotid and left vertebral arteries, via the right TRA for patients with an ARSA is nearly impossible. This is primarily due to the aberrant artery’s takeoff angle from the aorta, requiring the catheter to be maneuvered in a manner which allows 'reverse' catheterization. In these cases, we thought it feasible to attempt a left dTRA for access to the bilateral internal and external carotid and left vertebral arteries. In cases where the left vertebral artery is the only vessel requiring catheterization or if right radial access is not possible, we have routinely used the left dTRA.
The left TRA has been well reported in the interventional cardiology literature, with several case series and studies demonstrating its safety, but its use for neurointerventional procedures has been reported only once.10 16–18 Despite the lack of neurointerventional literature, the left TRA is an excellent option in select cases, including those primarily requiring left vertebral artery catheterization as well as for patients with ARSA. A multicenter retrospective study demonstrated that the left TRA is a safe and feasible alternative to the TFA when the right TRA is not an option for neurointerventional procedures in patients with otherwise normal anatomy.10 The authors presented 25 cases in which the left TRA was used in 19 patients, with only one case requiring cross over to the TFA.10 Left radial access is used less frequently by neurointerventionalists owing to the challenges in positioning the left wrist for access and the unfamiliarity of forming the Simmons catheter from the left side. Placing the wrist in a neutral position across the abdomen as close as possible to the right femoral access site overcomes the ergonomic challenge of having a left-sided access site while standing on the right side of the patient. Thus, positioning for the dTRA is easier than for the traditional proximal TRA. In addition, the Simmons catheter can be reshaped in a number of ways from the left side. Although the catheter is shaped in the opposite direction, the principles remain the same. Our technique and results further demonstrate that the left distal radial artery is a feasible access site for catheterization of bilateral carotid, left vertebral, and right subclavian arteries for patients with ARSA.
Conclusion
The presence of an ARSA does not exclude patients from undergoing the TRA. When encountering patients with an ARSA, the left dTRA is a feasible alternative to the TFA. Most interventionalists will use the traditional TFA for patients with this rare anatomical variant. We have presented three cases in which the left dTRA was used successfully. Once the operator is familiar with the left dTRA techniques, the increased risks and morbidity involved with the TFA for these patients may be avoided.
References
Footnotes
Contributors All authors have contributed to this manuscript. NM, AG, and PP drafted and edited the manuscript. The manuscript was edited by, and project was overseen by, PKA, GG, and PK. NVP edited and provided illustration assistance.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval IRB Pro2018002912.
Provenance and peer review Not commissioned; externally peer reviewed.