Article Text

Abstract
Background Intra-arterial therapy (IAT) is increasingly used to treat patients with acute stroke with large vessel occlusions. There are minimal data and guidelines for treatment indications and performance standards. We aimed to gain a better understanding of real-world practice patterns for IAT.
Methods An internet-based survey was launched to address six specific areas of IAT: practice setting, operator background, operational protocols, quality/safety, decision-making and treatment strategies. The survey invitation was distributed to members of multiple neurointerventional societies.
Results Responses from 140 neurointerventionalists worldwide were analyzed. The median annual volume of IAT cases per institution was 40, and the median neurointerventional group size was three staff members. Independent predictors of case volume were presence of comprehensive stroke services and telestroke capability. The median minimum National Institutes of Health Stroke Scale score for treatment consideration was 8, although 60% of respondents reported no minimum score cut-off. There was no strict time window from symptom onset to treatment among 41% of respondents for anterior circulation strokes and among 56% for posterior circulation strokes, instead basing treatment decisions on clinical and imaging findings. Despite the emphasis on imaging-based selection, there was pronounced variability in the criteria used. Only 27% used one imaging approach exclusively. IAT following full- or partial-dose intravenous tissue plasminogen activator was performed by 89%. Mechanical devices were the predominant first-line therapy, but specific device usage depended on practice location. Approximately half preferred conscious sedation during IAT.
Conclusions This survey illustrates significant variation among neurointerventionalists in the real-world use of IAT. Our findings highlight the need for evidence-based practice guidelines.
- Stroke
- Intervention
Statistics from Altmetric.com
Introduction
Of the estimated 700 000 ischemic strokes occurring in the USA annually, approximately 20% are due to proximal intracranial artery occlusions.1 ,2 Such occlusions are associated with increased odds of major morbidity and mortality,1 but outcomes may be improved with timely recanalization.3 Because intra-arterial therapy (IAT) yields significantly higher recanalization rates than intravenous tissue plasminogen activator (tPA),4–6 IAT is increasingly being used to treat patients with acute ischemic stroke with proximal occlusions,7 particularly those who do not respond to intravenous tPA.8
Only one randomized controlled trial to date has formally demonstrated the clinical efficacy of endovascular stroke treatment.4 Consequently, minimal evidence-based guidelines exist for indications and performance standards for IAT, unlike for intravenous tPA use.9 Moreover, poorly standardized research methods in IAT studies may underestimate or neglect the impact of potentially important factors such as local stroke care delivery, treatment selection criteria and therapeutic approaches.9 It is therefore likely that marked heterogeneity exists in the real-world endovascular treatment of stroke. Such heterogeneity may account for the variable results reported in the literature and may serve as a barrier to our understanding of clinical outcomes following IAT.
Our aim was to gain a better understanding of real-world IAT practice patterns among neurointerventionalists, with a focus on operational protocols, criteria used for IAT decision-making and treatment strategies.
Methods
Survey development
This study was designed by the Division of Neurointerventional Radiology within our medical center and received approval by an independent Institutional Review Board (IntegReview, Austin, Texas, USA). The survey was piloted among five neurointerventionalists and revised prior to launch. The survey period was from July to December 2011. The Google (Mountain View, California, USA) Form template was used to create an internet-based survey platform. A study website was launched containing a statement on rationale and a survey link.
Participant selection
Members of the major neurointerventional societies (Society of Vascular and Interventional Neurology, Society of NeuroInterventional Surgery, World Federation of Interventional and Therapeutic Neuroradiology) were invited to complete the survey. The study was open to physicians from any primary specialty (neurology, radiology, neurosurgery) in practice or training in neurointervention.
Survey content
Forty-five questions were categorized into six specific areas related to endovascular treatment of acute ischemic stroke: practice demographics, operator background, operational protocol, quality/safety assessments, decision-making and treatment strategies. The answer formats were text, multiple choice or checkboxes.
Survey administration
Survey invitations were sent electronically to neurointerventional society members for whom contact information (ie, email addresses) was available (n=295). The notifications contained a study description, eligibility criteria and instructions for completion. Monthly reminders were sent to non-respondents.
To maximize participation, invitees were informed that responses would be anonymized prior to analysis and reporting. Additionally, participants were entered into a raffle held at study completion in which three individuals were randomly selected to win Apple (Cupertino, California, USA) products. To prevent duplicate entries and maintain integrity of the responses, participants were required to provide their name and email address and were sent an email confirmation of survey completion.
Data collection and processing
Individual responses were automatically logged into an Excel (Microsoft, Redmond, Washington, USA) database. All fields containing personal identifiers (names, email addresses) were anonymized prior to data analysis.
Statistical analysis
Data were summarized as percentages and medians with IQR. Categorical data were compared using the χ2 test and ordinal data were compared using the Mann–Whitney test. Multiple linear regression was performed to identify independent predictors of institutional annual case volume. MedCalc V.10.0.0 (Mariakerke, Belgium) was used for all statistical analysis. Statistical significance was taken as a two-tailed p value <0.05.
Results
Response rate and physician demographics
The survey response rate was 47.5% (140/295), consisting of 71 neurologists, 53 radiologists, 14 neurosurgeons and two reporting dual training. The majority (n=94; 67%) were attending level physicians. The median duration of neurointerventional training was 2 years (range 0–5); 82% of attending physicians trained for ≥2 years. Radiologists reported the longest duration of neurointerventional practice (median 10 years, IQR 4–16.5), followed by neurosurgeons (8.5 years, IQR 5.5–13) and neurologists (3 years, IQR 2–6).
Practice setting and resources
The practice characteristics are summarized in online supplemental table S1. The majority of participants (76%) were based in North America, followed by Europe (9.3%), Australia/New Zealand (6.4%), East/South Asia (6.4%), South America (1.4%) and Africa (0.7%). Approximately 71% were based at an academic center. The median number of neurointerventionalists performing IAT within each practice was 3 (IQR 2–3, range 1–7); academic hospitals were associated with larger practice size (median 3 vs 2 staff neurointerventionalists; p<0.0001).
Approximately 80% (111/140) of respondents worked at institutions providing all the following stroke services (hereafter referred to as comprehensive stroke centers (CSCs)): a dedicated neuroscience intensive care unit or stroke care unit, open cerebrovascular neurosurgery program, acute stroke team and written acute stroke protocol. There were 77 neurointerventionalists (55%) whose hospitals provided telestroke services (remote audio and/or video evaluations) to nearby centers. The median estimated annual volume of IAT cases per institution was 40 (IQR 21–60, range 1–150). CSCs (median 50 vs 27, p=0.0009) and those with telestroke services (median 50 vs 30, p=0.002) had higher case volumes. The only independent predictors of annual case volume were CSC status (p=0.03) and telestroke capability (p=0.04).
Operational protocol
Results related to operational protocols are shown in online supplemental table S2. Although 84% (n=118) reported monitoring time intervals to IAT, 71% (n=99) had not established a goal time from patient presentation to procedure initiation. Among those with an established goal time (n=40), 30–60 min from the emergency department to IAT was the most common interval (73%). Alert notification to the interventional neuroradiology team for potential IAT cases followed an established protocol (ie, at a specific point in patient evaluation) according to 51 respondents (36%). Only 32 of the 77 (42%) with telestroke capabilities received prehospital notifications.
There was an even distribution between general anesthesia (49%) and conscious sedation (51%) as the primary mode of anesthesia during IAT. Only 26% (28/108) had an established protocol for the use of conscious sedation. For patients treated under general anesthesia with stable respiratory function, only 31% reported extubating patients immediately after the procedure. Timing of extubation was variable in 54% who generally deferred the decision to their intensive care colleagues.
Quality and safety
The assessment of quality and safety measures and their relationship with select neurointerventional practice characteristics are presented in online supplemental table S3. High-volume centers more frequently tracked time intervals to IAT, and participation in clinical trials occurred more frequently in academic hospitals, high-volume centers and CSCs.
Decision-making criteria
Results for decision-making criteria are presented in table 1. For most respondents (74%), the interventional radiology and stroke teams jointly decided whether to pursue IAT. Among 55 (41%) who reported a minimum National Institutes of Health Stroke Scale (NIHSS) score for treatment consideration, the median score was 8 (IQR 6–10, range 3–13). Five respondents (3.6%) stated that aphasia, hemiplegia or hemianopsia would prompt treatment despite scores below their minimum threshold.
Intra-arterial therapy (IAT) decision-making
Less than 8 h from last seen normal (LSN) was the most common (35%) time window for consideration of IAT in anterior circulation occlusions whereas 24 h (31%) was the most frequent time limit in the posterior circulation. Notably, for anterior and posterior circulation strokes, 41% and 56% of participants, respectively, did not impose a firm time limit for consideration of IAT, instead relying on clinical and imaging findings. High-volume centers were more likely not to use strict time windows for either anterior (69% vs 46%, p=0.01) or posterior circulation strokes (67% vs 39%, p=0.002).
Imaging modalities for IAT evaluation consisted of CT alone for 77 respondents (55%), MRI alone for 8 (5.7%), CT and/or MRI for 51 (36%) and were unspecified for 4 respondents (2.9%). There was no association of imaging modality with hospital location, practice type, case volume or CSC services. Perfusion imaging with either modality was reported by 104 (74.3%), and was more common in academic centers (81% vs 59%, p=0.01) and CSCs (79% vs 55%, p=0.02).
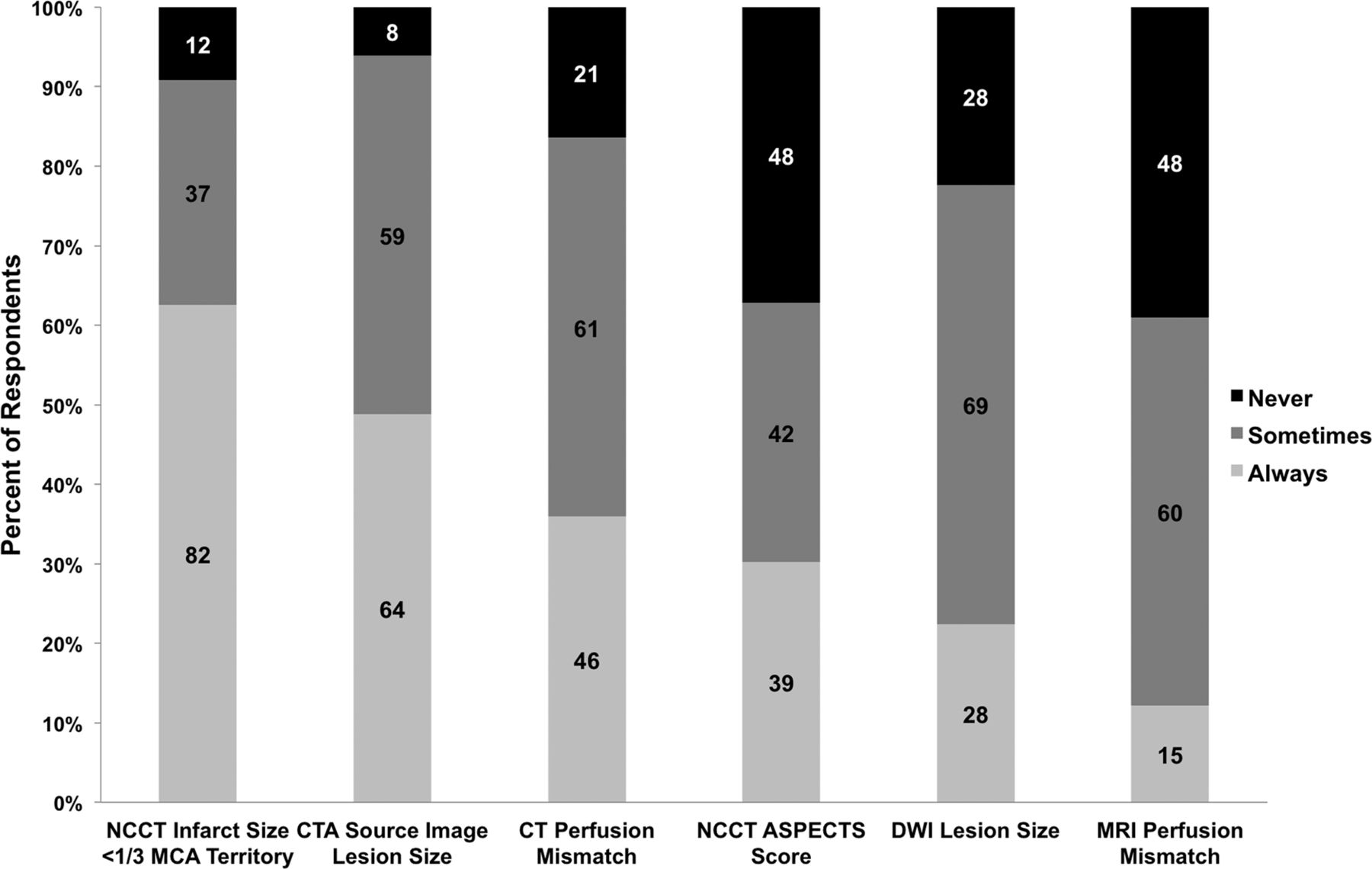
As shown in figure 1, CT-based imaging profiles were the most common criteria always used for patient selection, followed by MRI approaches (p<0.0001). Interestingly, only 27% (n=38) reported always using the same imaging strategy. Almost 60% (83/140) reported more than one approach as always being used, and 14% (19/140) did not report any approach as always being used. When asked to identify a single method for assessing infarct size, the majority (61.4%) reported using visual estimation; 8% (n=11) reported no routine infarct size determination for IAT decision-making. Overall, while nearly all participants (92%) reported measuring infarct size with various methods, only half (71/140) applied an infarct volume and/or Alberta Stroke Program Early CT Score (ASPECTS) score threshold as exclusion criteria (table 1).

Frequency of utilization of various imaging selection criteria for intra-arterial therapy. Data within bars represent absolute number of responses for each category. ASPECTS, Alberta Stroke Program Early CT Score; CTA, CT angiography; DWI, diffusion-weighted imaging; MCA, middle cerebral artery; NCCT, ???.
Treatment strategies
Treatment approaches and procedural characteristics are summarized in table 2. Bridging therapy was performed by 89% (124/140). A standard time interval for assessing response to intravenous tPA before proceeding to IAT was used by 55% (68/124), ranging from 10 to 70 min (median 60, IQR 30–60). Intra-arterial tPA was administered after full- or partial-dose intravenous tPA by 69% of respondents while 18% only used intra-arterial tPA after partial-dose intravenous administration.
Treatment strategies
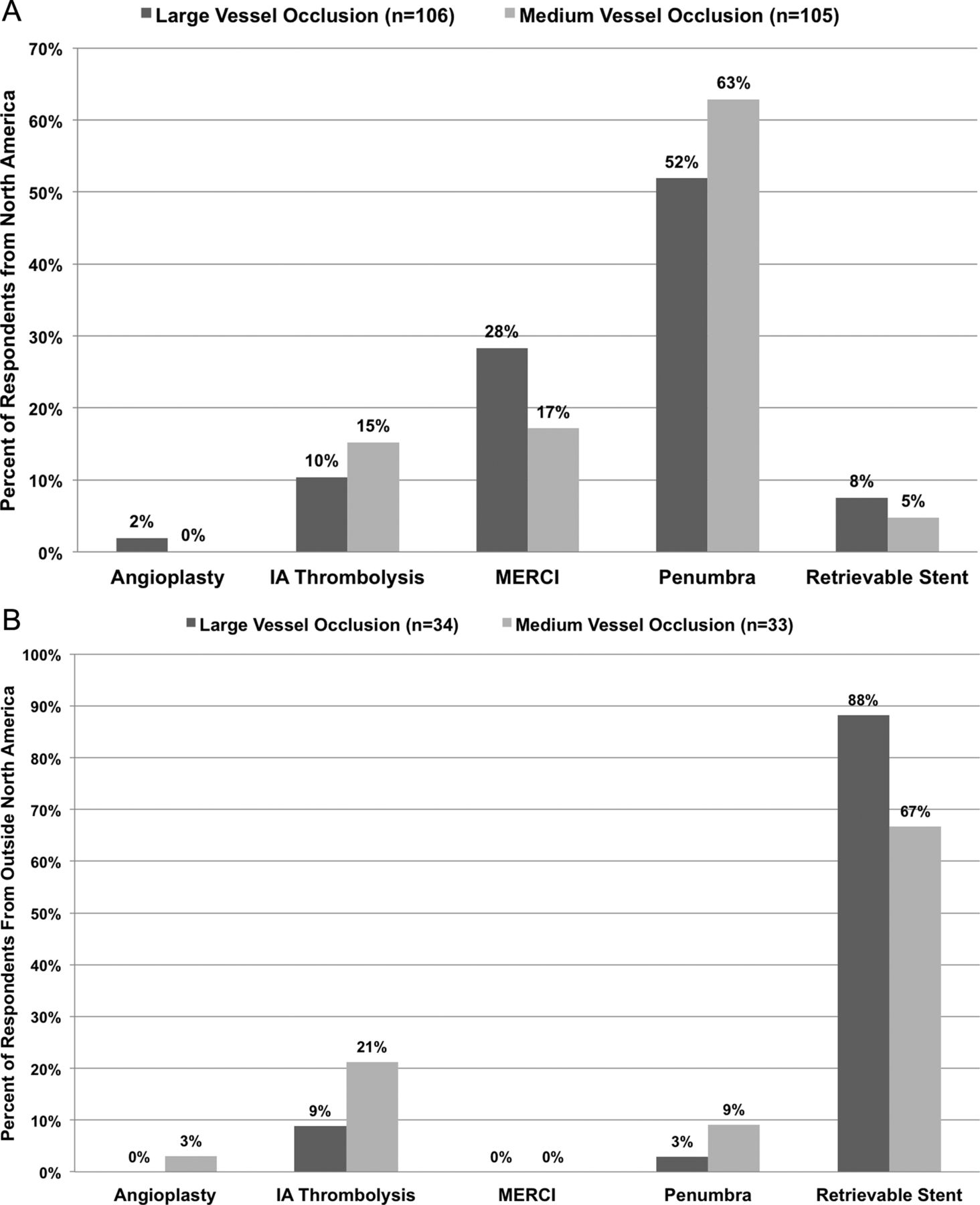
The preferred initial intra-arterial therapies for occlusions of large- and medium-caliber vessels are shown in figure 2. There was a strong dependence of the initial treatment method on geographic location (p<0.0001 for both large and medium occlusions). In North America, where retrievable stents were not widely available outside of trials at the time of this survey, the Penumbra system (Alameda, California, USA) was the first-line treatment for both large (55/106, 52%) and medium (66/105, 63%) vessel occlusions. For operators in other continents, retrievable stents were the first-line treatment for both large (30/34, 88%) and medium (22/33, 67%) vessel occlusions. The median number of device passes (Merci, Penumbra or retrievable stent) to achieve any level of recanalization before switching to alternative therapies was 3 (range 1–8). The usage rates of various adjunctive therapies are shown in online supplemental figure S1.

{kind=link}
{kind=link}
Initial treatment of choice for large and medium vessel occlusions. Penumbra was the first-line treatment among most participants in North America (A), while retrievable stent was the preferred initial treatment by those in the rest of the world (B) for both large (p<0.0001) and medium (p<0.0001) vessel occlusions. IA, intra-arterial.
Discussion
Intra-arterial therapy is increasingly being used to treat patients with major ischemic strokes. Despite this, there are few data on which to base clinical decision-making, confounded further by the wide array of diagnostic and therapeutic tools available to neurointerventionalists. As we hypothesized, the results of this international survey reveal a wide variation in practice patterns for IAT. The strengths of this study include its 48% response rate, which is in line with other published physician surveys,10 inclusion of all neurointerventional specialties and depth of inquiry into practice variables. As such, these results offer a representative overview of real-world IAT.
In order to facilitate quality improvement and develop national performance standards in the USA, the Joint Commission created a designation for primary stroke centers in 2003 and a similar effort is underway for CSCs.11 Not surprisingly, most respondents (80%) of this survey worked at institutions that offered key components of a CSC. Moreover, the majority of these centers assessed quality and safety metrics that have recently been proposed for CSC certification.11
There has been debate over the demand for IAT and whether the available workforce can meet this need.7 ,12 Total annual case numbers are imprecise but are projected to range from 10 000 to 40 000. Our survey findings are concordant with estimates of 1–2 cases per week at most institutions, supporting arguments against further expansion of the field.12 However, our findings also suggest that case volumes may increase with efforts to establish CSCs and develop telestroke networks; these two factors independently predicted higher case volumes, probably by ensuring adequate resources and facilitating patient transfers between community and tertiary care centers.
Goal door-to-CT and door-to-needle times for intravenous thrombolysis have been widely adopted.13 Because time to recanalization has been shown to be a strong predictor of favorable outcomes after IAT,14 monitoring time intervals from hospital arrival to IAT is a proposed core metric in recent guideline recommendations for CSCs, with a target of 2 h to treatment initiation.11 Although 84% of our respondents tracked times to IAT, 71% had not established a goal time and 36% did not have an established alert process for rapid activation of the interventional neuroradiology team. These findings suggest significant room for practice improvement.
Recent studies have examined the relationship between type of sedation during IAT and clinical outcomes,15 ,16 and have demonstrated worse outcomes with general anesthesia compared with local anesthesia. However, there remains an ongoing debate as to whether the root cause is the anesthetic, its effects on blood pressure or patient selection bias.17 An acknowledged benefit of general anesthesia is decreased patient movement which may shorten procedural duration and facilitate successful reperfusion. Participants in our survey reflected the overall state of uncertainty as they were evenly divided in their choice of anesthesia.
A major finding of our survey is the significant variability in IAT decision-making criteria. Although the median minimum NIHSS score of 8 for IAT consideration was similar to that used in device trials,5 ,6 the majority of respondents (60%) reported no minimum cut-off score. This finding is particularly relevant for patient outcomes as almost half of patients presenting with NIHSS <8 improve to 0–1 by 48 h without thrombolysis18 and, regardless of the type of treatment instituted, many have good 3-month functional outcome.19 Moreover, the PROACT II trial demonstrated that there was no benefit from intra-arterial treatment in patients with baseline NIHSSS 4–10.4 In addition, the time window from LSN for treatment consideration was highly variable. There was no strict time limit for the anterior circulation in 41% and for the posterior circulation in 56% of respondents. For these neurointerventionalists, stroke duration was less critical than the clinical and imaging findings in a particular case.
Despite the strong emphasis on imaging selection, there was pronounced variability in the use of imaging technologies and a lack of specific imaging criteria for decision-making. Over half of the respondents (55%) used only CT-based approaches, perhaps reflecting the greater accessibility of this modality. Surprisingly, MRI was used by approximately 40%, either alone or in combination with CT, arguing against its limited availability. Despite recent challenges to the utility of perfusion imaging,20 dynamic perfusion techniques were used by 74%, more commonly in academic centers and CSCs.
In addition to this variability in imaging technique, the approach to image interpretation was highly imprecise. Only 27% of respondents used one imaging criterion exclusively. Although almost all participants (92%) assessed infarct size, the majority used visual estimation which suffers from a high degree of error, and only half applied an infarct volume or ASPECTS score cut-off for excluding patients from IAT. This point bears emphasis as recent data suggest that pretreatment infarct size determines the clinical response to IAT.21 ,22
The largest difference in treatment strategies was the initial treatment method of choice. In North America, the Penumbra system was first-line therapy for both large and medium vessel occlusions. On the other hand, stent retrievers were first-line therapy for these occlusion levels in the rest of the world. At the time of our survey, no retrievable stents were available in North America outside clinical trials. Given the recent US Food and Drug Administration approval of the Solitaire FR device (ev3 Neurovascular, Irvine, California, USA) and more recently the Trevo Retriever (Concentric Medical, Mountain View, California, USA) as well as the widespread enthusiasm for these tools, we anticipate that North American usage will soon mirror international trends. Moreover, this study does not address usage of newer devices such as the Penumbra Separator 3D introduced after the completion of our survey.
Study limitations
This study has limitations inherent to any survey. In order to maximize participation, the scope of topics was limited and necessarily reflects the clinical and research questions of most interest at our institution. There may be responder bias as most of the participants were neurologists and radiologists from academic centers, while the field is comprised of many neurosurgeons as well. Differences between these specialties and their practices may exist, but our numbers were too small to determine statistical significance. Additionally, the responses to some questions could have been subject to recall bias.
Conclusion
This survey provides a comprehensive overview of real-world practice patterns for IAT in acute stroke. Our results reveal a significant variability in operational protocols, decision-making criteria and treatment approaches, which may contribute to the heterogeneous outcomes in the literature. Prospective clinical studies are needed to compare the effectiveness of these variable approaches in order to develop evidence-based guidelines.
Acknowledgments
We would like to extend our gratitude to all the physicians who participated in our survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Funding None.
-
Competing interests JAH is on the MERCI Registry Steering Committee but receives no financial compensation. NSR is supported by the NINDS (K23NS064052).
-
Ethics approval Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.