Article Text

Abstract
Background The transfemoral approach has been a common technique for carotid artery stenting (CAS). When aortic or peripheral arterial conditions limit the transfemoral approach, the transbrachial approach may be used as an alternative. The purpose of our study was to report initial experiences of CAS with a novel sheath guide specifically designed for transbrachial carotid cannulation.
Methods Patients who underwent transbrachial CAS with a novel sheath guide between May 2011 and July 2012 were analyzed. The sheath guide has an internal diameter of 6 Fr (2.24 mm, 0.088 inch) and is 90 cm long with a soft distal part and a particular distal shape like a modified Simmons catheter.
Results Sixty-two patients underwent transbrachial CAS with the sheath guide. Transbrachial carotid cannulation was easy and successful and CAS procedures were performed easily through the sheath guide in every case. No sheath-related periprocedural complications occurred.
Conclusions The sheath guide specifically designed for transbrachial carotid cannulation is useful for transbrachial CAS.
- Angioplasty
- Stent
Statistics from Altmetric.com
Introduction
The transfemoral approach is commonly used for carotid artery stenting (CAS).1 However, it is difficult to advance a guiding catheter into the carotid artery through the femoral route in patients with a tortuous aortic arch or those with an unfavorable supra-aortic take-off, aortic disease or occlusion of the femoral artery.2–8 Some previous studies have reported that transbrachial CAS is effective in cases unsuitable for transfemoral CAS due to aortic or peripheral arterial conditions.2–7 Indeed, the transbrachial approach may be an alternative to the transfemoral route, but no sheath guides have been specifically designed for transbrachial carotid cannulation which is sometimes difficult. A sheath guide specifically designed for transbrachial carotid cannulation has recently become commercially available. We report our initial experience of CAS with this novel sheath guide.
Materials and methods
We evaluated the results of transbrachial carotid cannulation in patients who underwent elective transbrachial CAS between May 2011 and July 2012. The patients were given details of the purpose, drugs, risks and benefits, and alternatives to transbrachial elective CAS and gave their written informed consent. For at least 3 days before CAS they were given oral aspirin (100 mg/day) and clopidogrel (75 mg/day).
Technique
The MSK-guide 7.5×90 (Medikit, Tokyo, Japan) sheath guide with an internal diameter of 6 Fr (2.24 mm, 0.088 inch) and 90 cm long was used. It has a U shape (figure 1) specifically designed for transbrachial carotid cannulation like a modified Simmons catheter and for stability during procedures. It has a very soft distal part of 7.5 cm length for direct and safe carotid cannulation. Catheters of 6 Fr or less can be inserted smoothly through it.
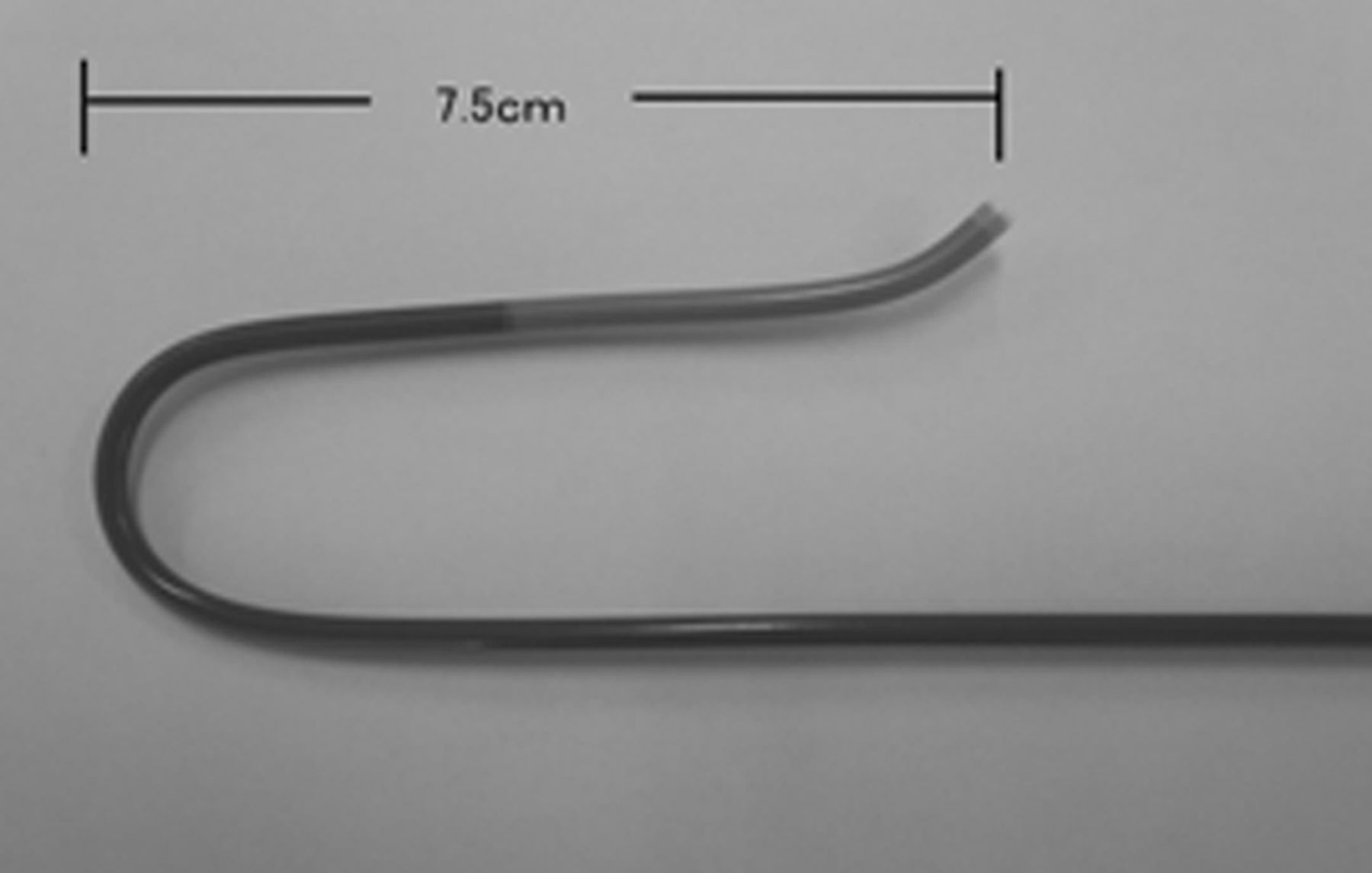
Sheath guide of 6 Fr internal diameter and 90 cm in length (MSK-guide 7.5×90) specifically designed for transbrachial neuroendovascular therapy.
The right brachial artery was used as the access route unless there were any problems, in which case the left brachial artery was selected as the access route. First, the MSK-guide 7.5×90 was positioned in the ascending aorta with the coaxial technique consisting of a 5 Fr outside diameter catheter of 130 cm length (5 Fr MSK; Medikit) (see figure 2A–D and videos in online supplementary files), and introduced directly into the affected common carotid artery (CCA) like a modified Simmons catheter (see figures 3A,B and 4A,B and videos in online supplementary files). When the activated clotting time became shorter than 150 s, the sheath guide was removed and hemostasis was obtained by manual compression.
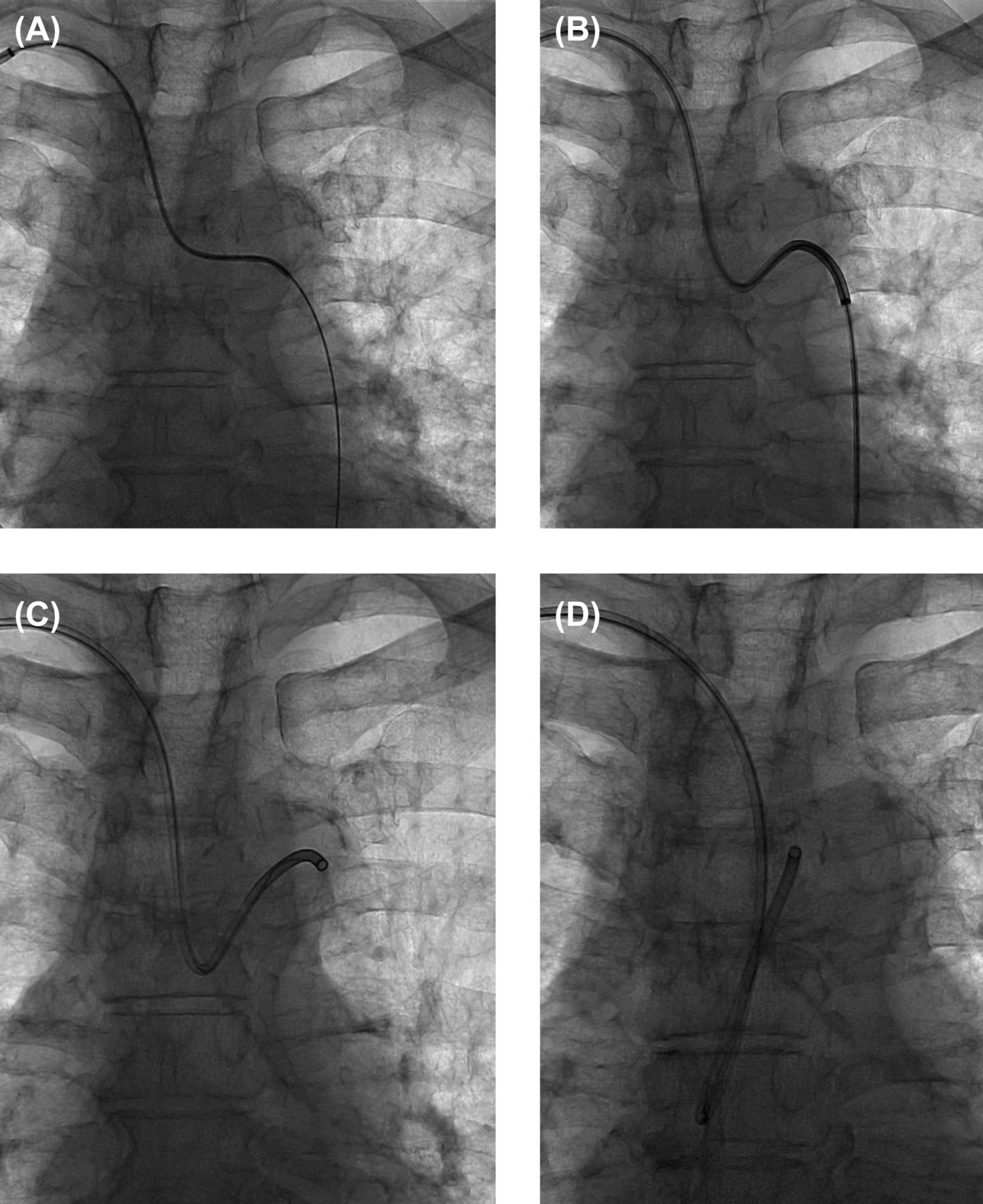
Navigating the MSK-guide 7.5×90 into the ascending aorta. The 5 Fr MSK catheter was advanced to the descending aorta over a 0.035 inch guidewire (A). The MSK-guide7.5×90 with the 5 Fr MSK catheter was advanced coaxially to the descending aorta (B), positioned in the aortic arch (C) and then positioned in the ascending aorta (D).

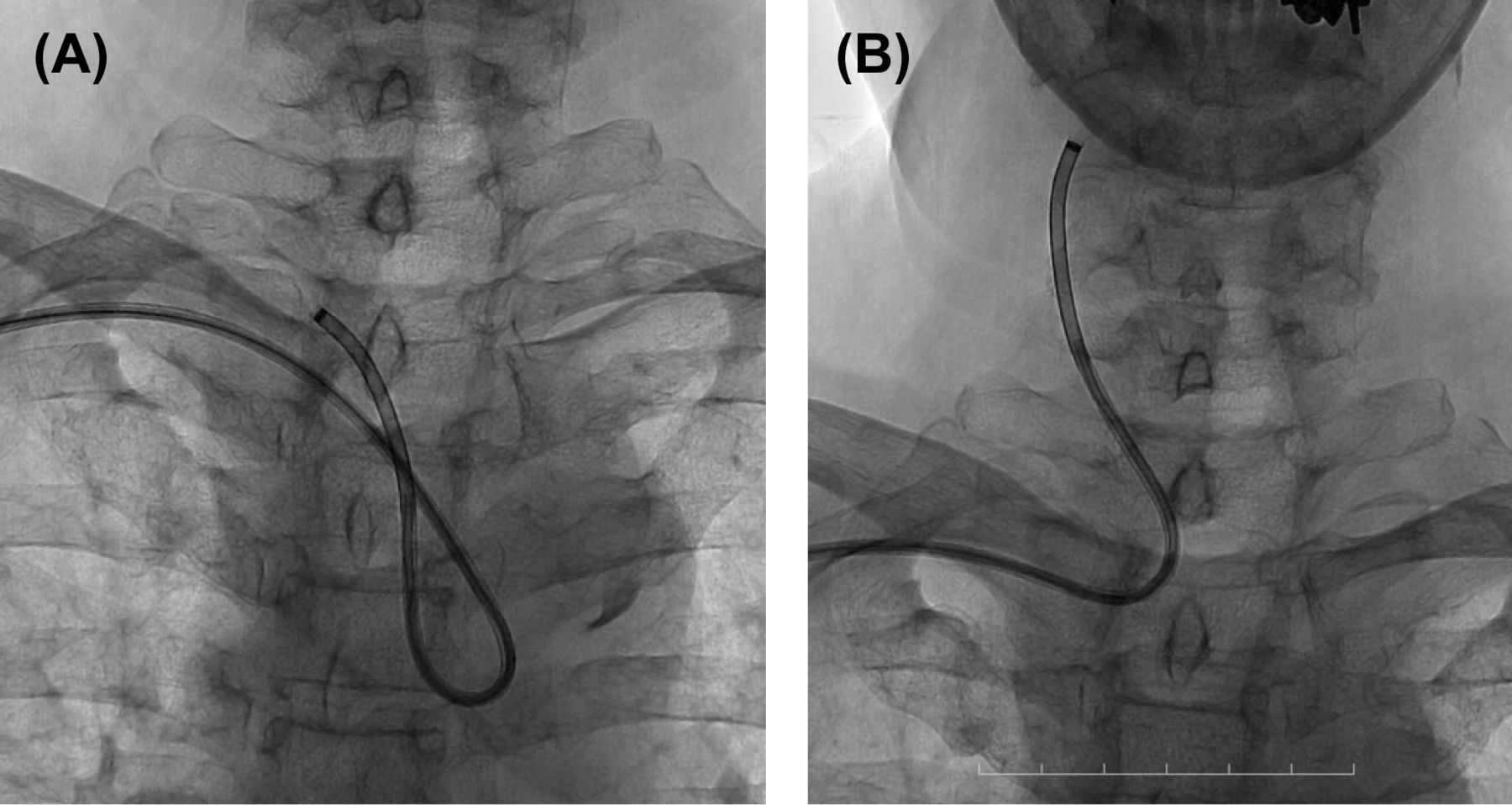
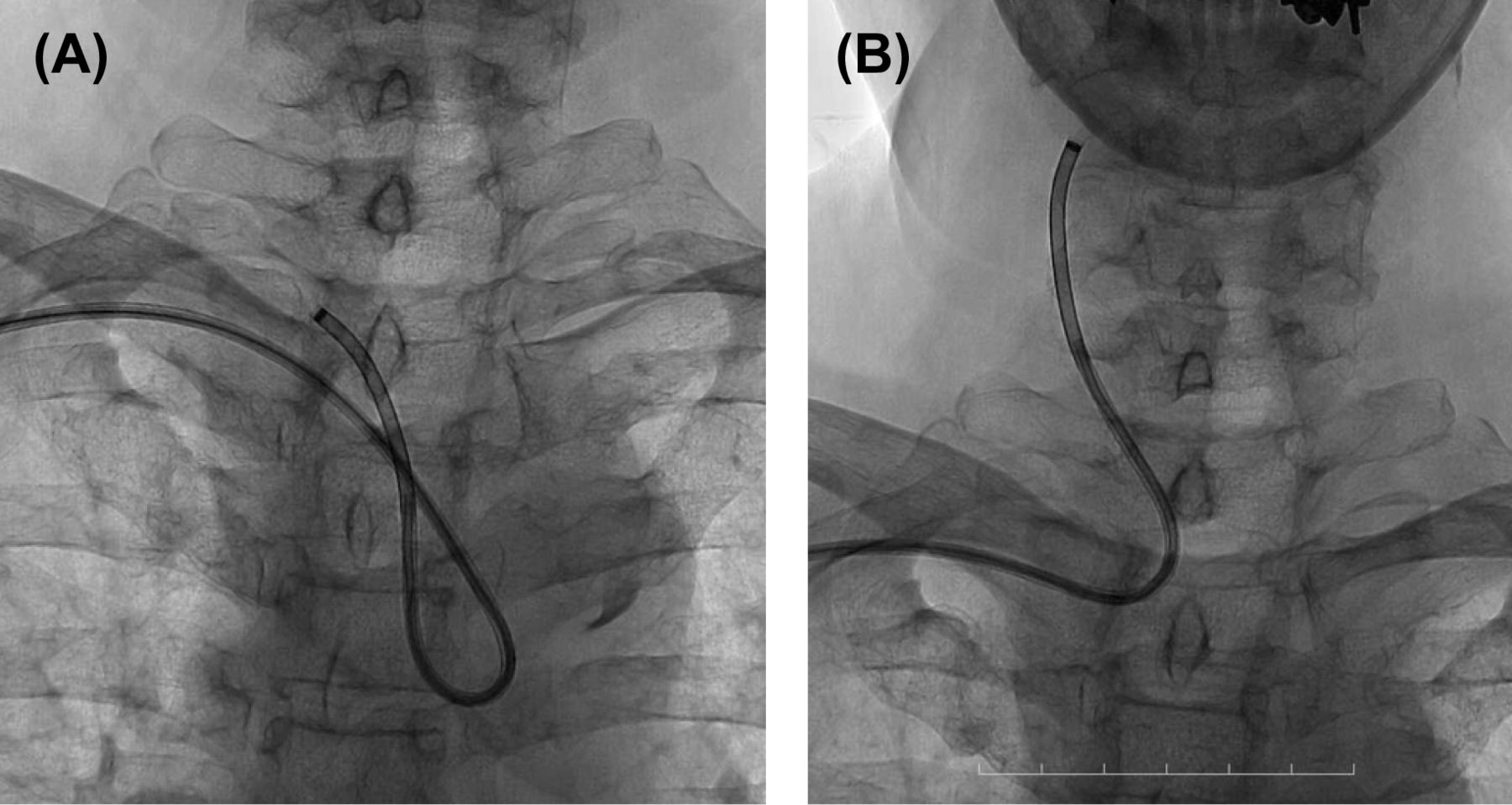
Navigating the MSK-guide 7.5×90 into the left common carotid artery (CCA). The MSK-guide 7.5×90 was cannulated directly into the left CCA like a modified Simmons catheter without an exchange wire (A) and then introduced directly into the left CCA (B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Navigating the MSK-guide 7.5×90 into the right common carotid artery (CCA). The MSK-guide 7.5×90 was cannulated directly into the right CCA like a modified Simmons catheter without an exchange wire (A) and then introduced directly into the right CCA (B).
Carotid artery stenting
Distal protection devices such as Angioguard (Cordis, Johnson and Johnson, Warren, New Jersey, USA) or FilterWire EZ (Boston Scientific, Natick, Massachusetts, USA) were used. Carotid Wallstent (Boston Scientific) or Precise (Cordis, Johnson and Johnson) stents were deployed over the residual stenosis after predilation with Sterling balloon catheters (Boston Scientific), Rx-Genity (Kaneka Medix, Osaka, Japan) or Shiden (Kaneka Medix).
Evaluation
The success of the procedure and its duration were evaluated retrospectively. Procedural success was defined as successful carotid cannulation and/or successful dilation by balloons and/or deployment of stents. Access site and/or neurological complications were evaluated retrospectively. Two authors (YM or MN) reviewed the angiographic data and medical records.
Results
During the study period a total of 70 consecutive patients underwent CAS (7 patients underwent non-elective emergency CAS and 63 patients underwent elective CAS). Of the 63 patients, 62 underwent CAS with the MSK-guide 7.5×90 (table 1) and the remaining patient underwent CAS with proximal flow control via the femoral route due to thrombi around the carotid stenosis.9 The 62 patients underwent transbrachial or transradial diagnostic angiography via the right-sided access route with a 3.2 Fr catheter (125 cm, 3.2 Fr MSK catheter; Medikit) in our institution, which demonstrated that they had a high-grade carotid stenosis and had no problems using the right brachial artery route. The right brachial artery was therefore selected as the access route for the MSK-guide. Of the 62 patients, 55 (89%) were men; 17 had type I, 22 had type II and 23 had type III aortic arch type.10 Thirty-seven patients (60%) had right carotid artery stenosis and 25 (40%) had left carotid artery stenosis. Three of the 25 patients with left carotid artery stenosis had a so-called ‘bovine type lesion’11 and carotid lesions in 4 of the 25 patients were localized at the distal CCA (table 1). We were successful in carotid artery cannulation in a similar way to manipulation of a diagnostic catheter (see videos in online supplementary files) and stent deployment was successful in all 62 cases. The procedures through the right brachial route were successful in all 62 patients. The median total procedural time was 68 min. No sheath-related periprocedural complications occurred, but nine complications following CAS occurred (hypotension in four cases, headache in two cases, transient hemiparesis in one case, confusion in one case, delirium in one case; table 2). All nine patients returned to their previous state within a few days and had no neurological deficits.
Patient features
Post-carotid artery stenting in-hospital adverse events
Discussion
Our results suggest that transbrachial CAS with the sheath guide specifically designed for transbrachial carotid artery cannulation is feasible and safe.
Some previous studies have reported that the transbrachial approach for CAS is effective in cases unsuitable for transfemoral CAS due to aortic or peripheral arterial conditions.2–7 Indeed, the transbrachial approach may be an alternative to the transfemoral route, but no guiding catheter or sheath guide has been specifically designed for safe and stable transbrachial carotid cannulation. It was therefore sometimes difficult to position the guide catheter in the carotid artery and there was a need for a guide catheter or sheath guide specifically designed for safe and stable transbrachial carotid cannulation. The MSK-guide 7.5×90 could be cannulated simply and directly into the right or left CCA like the diagnostic catheter without the looping or retrograde engagement technique reported by Fang et al.12
Some previous studies have reported that the transradial approach is effective for CAS.13 ,14 They used the 6 Fr or 7 Fr sheath guide (Destination, Terumo, Tokyo, Japan or Shuttle SL Flexor Tuohy Borst, Cook, Bloomington, Illinois, USA) for the transradial approach.13 ,14 Pinter et al13 reported procedural success in 18 of 20 patients (90%); one failure resulted from intense radial artery vasospasm and the second failure occurred in a patient with a left-sided carotid lesion and type I arch. Radial artery occlusion occurred in one of the 18 patients. Similarly, Levy et al14 reported radial artery occlusion in one patient who underwent transradial CAS. With transradial CAS, post-CAS radial artery occlusion may occur, although post-CAS brachial artery occlusion rarely occurs. We have no data on the incidence of radial artery occlusion following CAS using the 6 Fr MSK-guide sheath because we have no experience of transradial CAS with it.
The Endarterectomy Versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) trial15 reported a median total procedural time of 70 min in patients who underwent usual transfemoral CAS. Our total procedural time of 68 min is therefore probably acceptable.
The MSK-guide with the form of the Simmonds type can give good and stable support in bovine arches and left carotid interventions. It can be cannulated into the CCA without a coaxial small catheter or guidewire. Its cannulation is therefore easy and safe in cases of stenosis at the distal CCA because the length of the distal soft segment of the MSK-guide 7.5×90 is 7.5 cm. Stenosis at the distal CCA can probably be stented without any problems. However, very proximal lesions involving the CCA probably limit its cannulation.
There are possible risks with manipulating the MSK-guide in calcified aortic arches, even though the guide has a soft distal segment and a soft tip. In addition, three probable risks with the transbrachial approach for CAS2–7 are pseudoaneurysm of the brachial artery, median nerve palsy and brachial artery occlusion.2–7 The current 6 Fr MSK-guide is not a balloon-guide catheter and cannot block proximal flow. This limits the application of the 6 Fr MSK-guide, which is not appropriate for patients in whom the flow reversal technique is required.9 ,16
Because of the small number of cases in the present study, a larger number of cases is required to confirm our results.
Conclusions
The sheath guide specifically designed for transbrachial carotid cannulation is useful for transbrachial CAS.
Acknowledgments
The authors acknowledge the secretarial assistance of Nozomi Chiba and the specialized assistance of nurses and radiological technicians in our neuroendovascular catheterization room.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video 1
- Data supplement 2 - Online video 2
Footnotes
-
Contributors TI authored the manuscript. TM proofread the manuscript and images. TI, TM, YT and KM participated in patient care. YM and MN analyzed and interpreted the data.
-
Funding None.
-
Competing interests TM: royalties (Medikit, Tokyo).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.