Article Text

Abstract
Background Conventionally, ‘successful’ endovascular thrombectomy (EVT) had been defined as achieving revascularization of thrombolysis in cerebral infarction (TICI)−2B or greater, rather than as ‘complete’ (TICI-3) versus ‘incomplete’ (TICI-2B) revascularization.
Purpose We performed a systematic review and meta-analysis of studies comparing clinical outcomes between patients with TICI-2B and TICI-3 revascularization.
Methods Multiple databases were searched for relevant publications between January 2003 and March 2018. Studies comparing outcomes between the TICI-2B and the TICI-3 group of acute ischemic stroke (AIS) patients treated with EVT were included. Random effects meta-analysis was performed to evaluate outcomes among TICI-2B and TICI-3 groups. The following outcomes were assessed: good neurologic outcome (modified Rankin Scale (mRS)≤2 at day 90), mortality, and intracerebral hemorrhage (ICH).
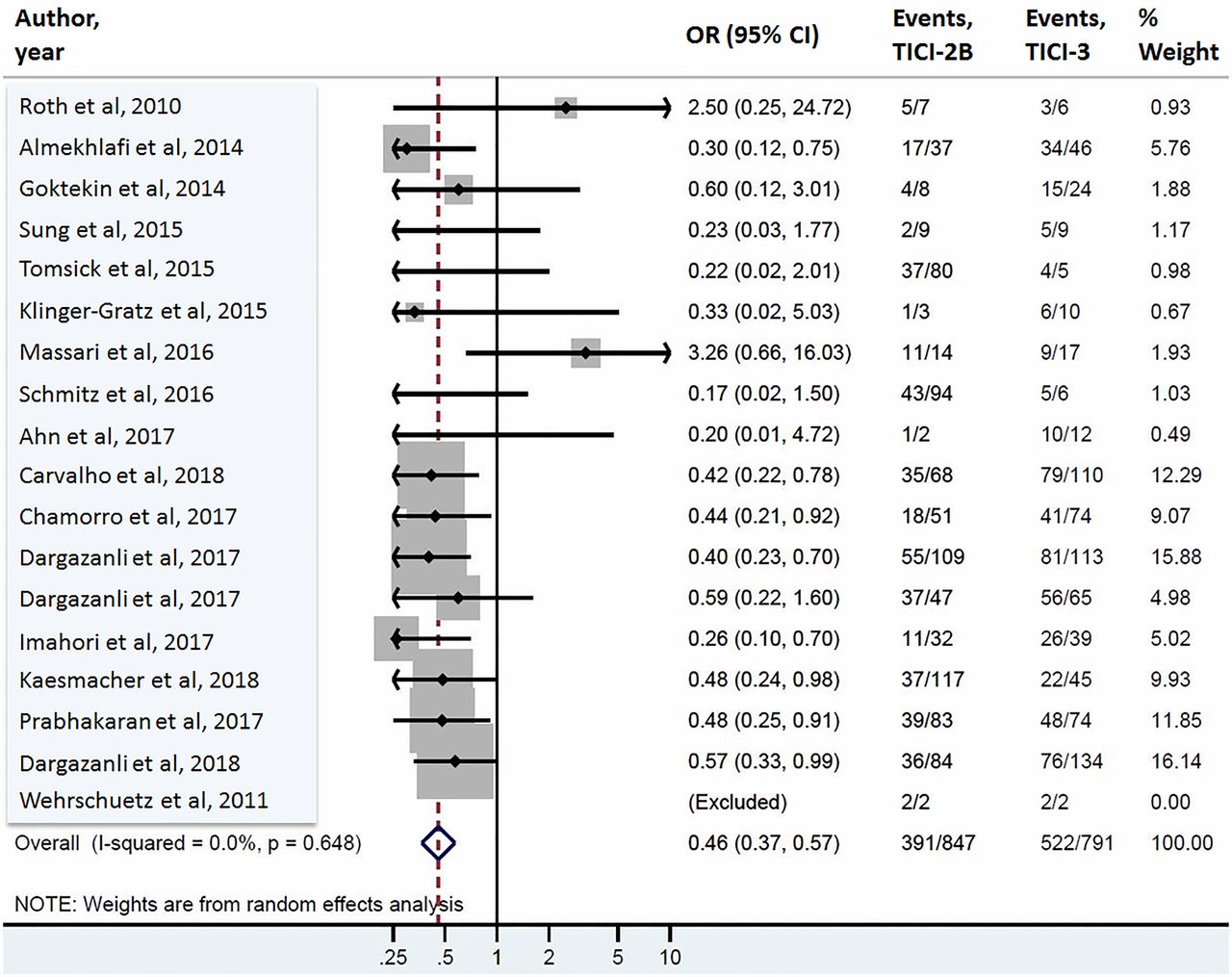
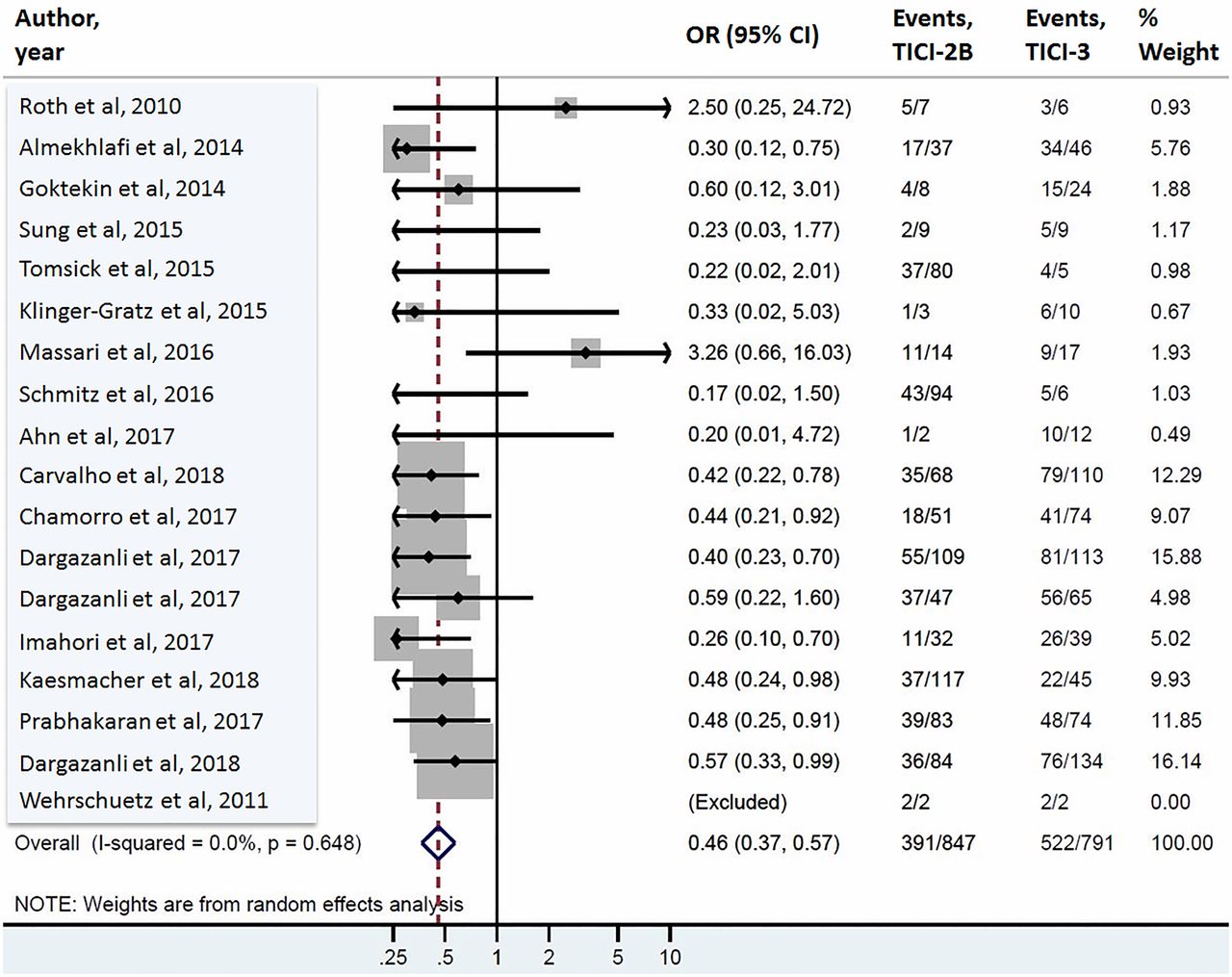
Results Twenty-one studies comprising 2747 patients were identified. Patients with TICI-2B revascularization had mRS≤2 at day 90 rates of 46% (391/847) compared with 66% (522/791) for TICI-3 patients (OR 0.46, 95% CI 0.37 to 0.57). Mortality rates were significantly higher in the TICI-2B group (78/570, 14%) than in the TICI-3 group (55/709, 8%) (OR 2.00, 95% CI 1.38 to 2.91). The ICH rates were also significantly higher in the TICI-2B group as compared with the TICI-3 group (31% [134/439] vs. 22% [108/490]; OR 2.20, 95% CI 1.47 to 3.30).
Conclusions Differences in all major outcome measures were markedly better in patients with complete versus incomplete but still ‘successful’ revascularization using prior thresholds, with ORs in the order of those seen in recent definitive trials comparing EVT to an intravenous tissue plasminogen activator.
- stroke
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
Introduction
Angiographic scales focused on the degree of revascularization represent a key outcome, either primary or secondary, in essentially all modern endovascular thrombectomy (EVT) studies.1 2 The vast majority of such studies define ‘successful’ revascularization as thrombolysis in cerebral infarction (TICI)−2B or greater.3 4 While that widely-applied threshold of ‘success’ has proved extremely valuable in demonstrating better clinical outcomes with successful revascularization, growing evidence suggests that ‘complete’ or TICI-3, rather than ‘incomplete’ or TICI-2B, revascularization may provide remarkable benefit in outcomes.5–7 If complete revascularization is associated with substantial benefit over incomplete revascularization in clinical outcome, then development of future devices and techniques might focus on complete revascularization as the primary goal.
In order to clarify the differences in key clinical outcomes between incomplete and complete revascularization, we performed a systematic review and meta-analysis of studies comparing outcomes between TICI-2B and TICI-3 revascularization in patients with acute ischemic stroke (AIS) treated with EVT.
Methods
Literature search
The current study adheres to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The electronic databases Ovid MEDLINE, Ovid EMBASE, and Scopus were systematically examined to locate relevant studies using predefined search criteria. The search strategy was designed and conducted by a medical reference librarian with input from the authors. Controlled vocabulary supplemented with keywords was used to search for endovascular thrombectomy and TICI-2B and TICI–3. The search was confined to investigations that were published between January 2003 and March 2018. The search strategy is available in the online supplementary appendix.
Supplementary file 1
Two investigators independently scanned all manuscripts and performed data extraction. Abstracts or conference papers were excluded because of insufficient data. All retrieved studies were examined and any potential overlapping data were omitted. Both independent reviewers performed the final screening of reports for inclusion in the meta-analysis. In the event of any disagreement, a general consensus was met between reviewers after further extensive review of the full text articles. In addition, all references cited in the identified articles were manually searched for potentially relevant studies.
Study eligibility
The inclusion criteria for studies in the analysis were: studies comparing outcomes of two groups (TICI-2B and TICI-3) among AIS patients treated with EVT; and studies reporting separate outcomes between TICI-2B and TICI-3 groups wherein sufficient data were available so that a 2×2 contingency table of results could be constructed. Studies with posterior circulation stroke or AIS patients with posterior circulation occlusion were excluded from this meta-analysis. Additionally, studies were excluded if AIS patients were treated with intravenous tissue plasminogen activator (IV-tPA) alone, animal or in-vitro studies, no information with regards to modified Rankin Scale (mRS)≤2 at 90 days or National Institutes of Health Stroke Scale (NIHSS) score at discharge ≤5, and articles not in the English language.
Data collection
Two independent investigators (AR and SMS) extracted data with subsequent verification. The following data were collected for each eligible investigation: year of publication; patient demographics; and occlusion location (table 1).
Study characteristics
Risk of bias assessment
Risk of bias assessment of the studies was performed using a modified Newcastle Ottawa Scale. Each study is judged on eight items categorized into three groups: selection of the study groups; comparability of the study groups; and ascertainment of the outcome of interest.8 For the purpose of the current study, we determined that the risk of bias depended mainly on two factors: adjustment or matching for age and sex; and the independent or blinded assessment of clinical outcomes.
Outcome variables
For the current study purposes, patients were divided into two groups: TICI-2B and TICI-3. Patients with TICI 0–2a were excluded. The following outcomes were assessed: good neurologic outcome, defined as a mRS of ≤2 at 90 days following endovascular treatment and/or National Institutes of Health Stroke Scale (NIHSS) at discharge ≤5, mortality, and intracerebral hemorrhage (ICH). In studies that did not explicitly report ICH, cases of parenchymal hematoma were classified as ICH.
Statistical analysis
From each eligible study, a 2×2 contingency table was extracted for binary outcomes. Random effects meta-analysis was used for pooling across studies.9 The I2 statistic was used to express the proportion of heterogeneity that is not attributable to chance.10 Meta-analysis results were expressed as OR with respective 95% confidence intervals (95% CIs). A sensitivity analysis was performed to compare clinical outcomes between the TICI-2B and the TICI-2C group of AIS patients treated with EVT. Furthermore, a sensitivity analysis was conducted for studies including data only from prospective randomized controlled trials (RCTs) to compare clinical outcomes between the TICI-2B and TICI-3 groups.11–13 The impact of publication bias was assessed by construction of funnel plots and testing their symmetry. Meta-analysis was conducted using STATA Version 14 (StataCorp LP, College Station, Texas, USA).
Results
Literature search
A systematic search revealed 857 articles from the literature search. After removing 40 duplicates, 817 articles were screened by title and abstract. Of these, 75 articles were read full-text. A total of 21 studies met the eligibility criteria and were included in the meta-analysis. A PRISMA flow chart of the search and selection process of the articles is shown in figure 1.

PRISMA flow diagram.
Baseline characteristics of each study are listed in table 1. Of a total 2747 patients (TICI-2B, n=1158; TICI-3, n=1024), the mean age within the studies ranged from 55 to 79 years. The largest study had 299 patients and the smallest study had seven patients.14 15 All patients in the included studies were treated with EVT. Eight studies were multi-center, while 13 were single-center studies. The risk of bias was low to moderate in all included studies (online supplementary table 1).
Supplementary file 7
Clinical outcomes
Acute ischemic stroke patients treated with EVT in whom TICI-2B revascularization was achieved, had mRS ≤2 at day 90 rates of 46% (391/847) compared with 66% (522/791) for patients in whom TICI-3 was achieved (OR 0.46, 95% CI 0.37 to 0.57; figure 2). The TICI-2B group revealed NIHSS≤5 at discharge in 34% (57/170) of patients as compared with 53% (82/154) in the TICI-3 group (OR 0.47, 95% CI 0.30 to 0.74; online supplementary figure 1). Mortality rates were significantly higher in the TICI-2B group (78/570, 14%) than in the TICI-3 group of patients (55/709, 8%) (OR 2.00, 95% CI 1.38 to 2.91; online supplementary figure 2). The rates of ICH were also significantly higher in the TICI-2B group as compared with the TICI-3 group (31% [134/439] vs. 22% [108/490]; OR 2.20, 95% CI 1.47 to 3.30; online supplementary figure 3). These data are summarized in table 2.
Supplementary file 2
Supplementary file 3
Supplementary file 4
{kind=link}
![[SP2.jpg]](https://jnis.bmj.com/content/neurintsurg/11/1/9/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
![[SP3.jpg]](https://jnis.bmj.com/content/neurintsurg/11/1/9/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
![[SP4.jpg]](https://jnis.bmj.com/content/neurintsurg/11/1/9/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
{kind=link}
Forrest plot for modified Rankin Scale (mRS)≤2 at day 90.
Categorical outcomes
Heterogeneity and publication bias
The I2 values were 0% for mRS≤2 at day 90 and NIHSS score ≤5 at discharge. The I2 values were 0% for mortality and 18% for ICH. The P-values for publication bias using Egger’s regression were 0.35 and 0.65 for mRS≤2 at day 90 and mortality, respectively (online supplementary figure 4), suggesting no bias.
Supplementary file 5
![[SP5.jpg]](https://jnis.bmj.com/content/neurintsurg/11/1/9/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Sensitivity analysis
A sensitivity analysis for comparison of outcomes among AIS patients achieving TICI-2B versus TICI-2C revascularization revealed similar results by demonstrating that TICI-2C was associated with superior clinical outcomes. The TICI-2B patients had significantly lower odds of good neurological outcomes than TICI-2C with no heterogeneity (mRS ≤2 at day 90: OR 0.55, 95% CI 0.37 to 0.83, I2=0%; and NIHSS score ≤5 at discharge: OR 0.47, 95% CI 0.26 to 0.85). Mortality and ICH rates were also higher in the TICI-2B versus the TICI-2C group of patients (mortality: OR 3.20, 95% CI 1.36 to 7.53, and ICH: OR 1.64, 95% CI 0.92 to 2.92, I2=0% for both). A sensitivity analysis for studies including data only from RCTs also revealed significantly lower odds of good neurological outcomes among TICI-2B patients as compared with TICI-3, with no heterogeneity (mRS ≤2 at day 90: OR 0.51, 95% CI 0.30 to 0.85, I2=0%; online supplementary figure 5).
Supplementary file 6
![[SP6.jpg]](https://jnis.bmj.com/content/neurintsurg/11/1/9/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
Discussion
Our current meta-analysis revealed that TICI-3 revascularization, as compared with TICI-2B, was associated with marked, statistically significant, and clinically relevant improvements in functional outcomes, both early and delayed, mortality, and ICH. Indeed, the ORs and absolute percentage differences in rates of good outcome were similar to differences seen in the pivotal trials comparing EVT to IV-tPA. Those pivotal trials and their attendant difference in outcome were hailed as a revolutionary achievement. Thus, it stands to reason that complete revascularization, with its attendant benefit over incomplete revascularization, should be strongly considered as a more clinically relevant threshold for ‘success’. This clarion call for a new definition of success should be heard by researchers, industry, and funding agencies, in order that novel techniques, devices, and approaches to EVT focus on the ‘right’ target for success.
Over the past years, multiple single-center and small multi-center studies have conventionally used TICI-2B/3 sub-summation as ‘successful’ revascularization and thereby predicting good neurological outcomes.16–18 However, more recent data suggests that among patients treated with EVT, ‘incomplete’ revascularization or TICI-2B has demonstrated poorer outcomes as compared with ‘complete’ revascularization or TICI-3.14 16 19–21 Furthermore, the endovascular field has adopted several modifications of the TICI grading system which specifically impact the TICI-2B category, using 50% vs 66% reperfusion as a threshold, whereas others are grading ‘near-complete revascularization without any visible occlusion’ as TICI-2C, which may have been classified as TICI-3 in the past. To this end, it was not surprising that the ORs for TICI-2B versus TICI-2C were similar to that of TICI-2B versus TICI-3 in the current study: truthfully, most of us cannot tell the difference between TICI-2C and TICI-3. These facts not only highlight the significance of the standardization of revascularization grading schemes, but also demand formal modification of reperfusion targets. The current study brings robust meta-analytic techniques to further underscore the need for complete revascularization and represents a systematic aggregation of clinical outcomes between the TICI-2B and the TICI-3 group of AIS patients. It extends the findings of smaller studies, which may be limited by factors such as small sample size or single-center design, and it broadens generalizability.
A growing number of experts have made a compelling argument to set TICI-3 only as the new standard for technical success.11 14 Additionally, the recent data from a multi-center DEFUSE-3 (ENDOVASCULAR THERAPY FOLLOWING IMAGING EVALUATION FOR ISCHEMIC STROKE 3) RCT parallels with the current study findings and have revealed significantly improved functional outcomes among TICI-3 versus TICI-2B patients (67% vs 46%).22 However, previous information lacked sufficient strength when individually considered. By rigorously consolidating available evidence, the current meta-analysis provides strong support to redefine successful revascularization as a TICI-3 score and targeting complete revascularization in all cases of EVT. Most notably, our findings suggest lower rates of ICH among TICI-3 group of patients, thereby negating the notion that complete revascularization might result in a greater risk of reperfusion hemorrhage.
This study has limitations. Many studies including some RCTs and studies with core laboratory adjudication did not provide data stratified in a way that helps answer this question and therefore were not included in the current meta-analysis. Not having core laboratory adjudication may introduce ascertainment bias. Additionally, the outcome results for a small number of studies were based on NIHSS scores rather than functional mRS scores, which is the most commonly used outcome measure. Publication bias was not assessed for NIHSS at discharge and ICH outcomes due to the small number of studies. Despite this, no bias was observed for the mRS and mortality outcomes.
Conclusions
Differences in all major outcome measures were markedly better in patients with complete revascularization compared with those with incomplete but still ‘successful’ revascularization using prior thresholds, with ORs on the order of those seen in recent definitive trials comparing EVT to IV-tPA. The research community should consider the redefinition of successful revascularization to reflect these patient-centric findings.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.References
Footnotes
Contributors AR, MHM, WB, AAR, and DFK have made substantial contributions to the: conception or design of the work or the acquisition, analysis, or interpretation of data for the work; and drafting of the work or revising it critically for important intellectual content. AR and SMS made substantial contributions to data collection. All authors have provided final approval of the version to be published. All authors are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data can be made available by contacting the corresponding author via email.