Article Text

Abstract
Background Tandem proximal and distal occlusions in the setting of an acute stroke are therapeutic challenges. Treating either lesion first has its respective shortcomings. An approach is described which may lessen the probability of distal embolic events during emergency carotid angioplasty and stenting during an acute stroke, and simplify access to both a distal and proximal lesion.
Clinical presentation A 58-year-old man presented with waxing and waning neurological examination with an NIH Stroke Scale varying from 4 to 21. CT angiography demonstrated a left internal carotid artery occlusion at its origin and a left middle cerebral artery occlusion. The CT scan failed to demonstrate significant ischemic changes so the patient was brought to angiography for treatment under conscious sedation.
Intervention Triaxial access into the distal middle cerebral artery was achieved followed by brief aspiration and clot maceration by opening the vessel completely. An embolic protection device was deployed through the intermediate catheter which was subsequently removed. Stenting and angioplasty were then performed, followed by removal of the embolic protection device which had visibly trapped debris.
Conclusion Embolic protection devices may have a role in the emergency treatment of proximal occlusions in the setting of an acute ischemic stroke. Safe deployment through an occluded vessel may be assisted by use of an intermediate catheter. The Penumbra 054 catheter may be used both to aspirate the distal thrombus and to house the embolic protection device as it is advanced past a proximal occlusion.
- Penumbra
- acute stroke
- tandem occlusion
- carotid occlusion
- embolic protection devices
- stroke
Statistics from Altmetric.com
Acute ischemic strokes may result from emboli derived from proximal atherostenoses. Not infrequently, tandem occlusions of both the internal carotid artery (ICA) origin and a distal location such as an M1 middle cerebral artery (MCA) segment may be encountered. The time to restoration of flow is a parameter likely to influence salvage of parenchyma at risk. As such, approaches that expedite this process are preferable. The order of treatment (proximal or distal) should aim to restore flow to the parenchyma at risk as quickly as possible, tailored to the patient's anatomy and collateral circulation. Treatment of the proximal lesion often requires a stent, which poses a risk of embolism to the distal vasculature.
The authors present an approach to restore distal flow while reducing the risk of distal embolization during ICA revascularization using a distal embolic protection device (EPD) in the setting of an acute ischemic stroke.
Case report
History and physical examination outside hospital
A right hand dominant person in the late 50s with a past medical history significant for hypertension and hyperlipidemia presented with an acute onset of right-sided weakness, confusion and aphasia at 05:30 after a morning shower. The patient improved en route to the outside emergency room with an NIH Stroke Scale (NIHSS) of 4 on admission. A CT scan was performed which was unremarkable for hemorrhage with no significant early ischemic changes. During the CT scan, however, the patient developed worsening aphasia and right-sided weakness, with an NIHSS of 21. Intravenous tissue plasminogen activator was administered at 07:00 and the patient was transferred to our hospital.
Hospital course
Upon arrival the patient's NIHSS was 8. Laboratory examinations were unremarkable. Admission blood pressure was 140/80. A CT scan of the brain showed no evidence of new ischemic changes CT angiography (CTA) showed occlusion of the left ICA origin, as well as a left M1 occlusion. During the CT/CTA the NIHSS worsened again to 20. The patient was then taken to the angiography suite and was placed under conscious sedation.
Operative procedure
The initial angiograms showed occlusion of the left ICA at the origin (figure 1) without ipsilateral reconstitution. Angiography of the contralateral ICA demonstrated cross-filling into the left anterior cerebral artery (ACA) territory without significant MCA opacification. Angiography of the left vertebral artery revealed a robust posterior communicating artery that supplied the ICA, left ophthalmic artery and left ACA. The MCA did not opacify well. ACA to MCA leptomeningeal collaterals were present.

Digital subtraction angiogram of the left internal carotid artery showing an occluded left internal carotid artery (arrow) and stenotic external carotid artery origin.
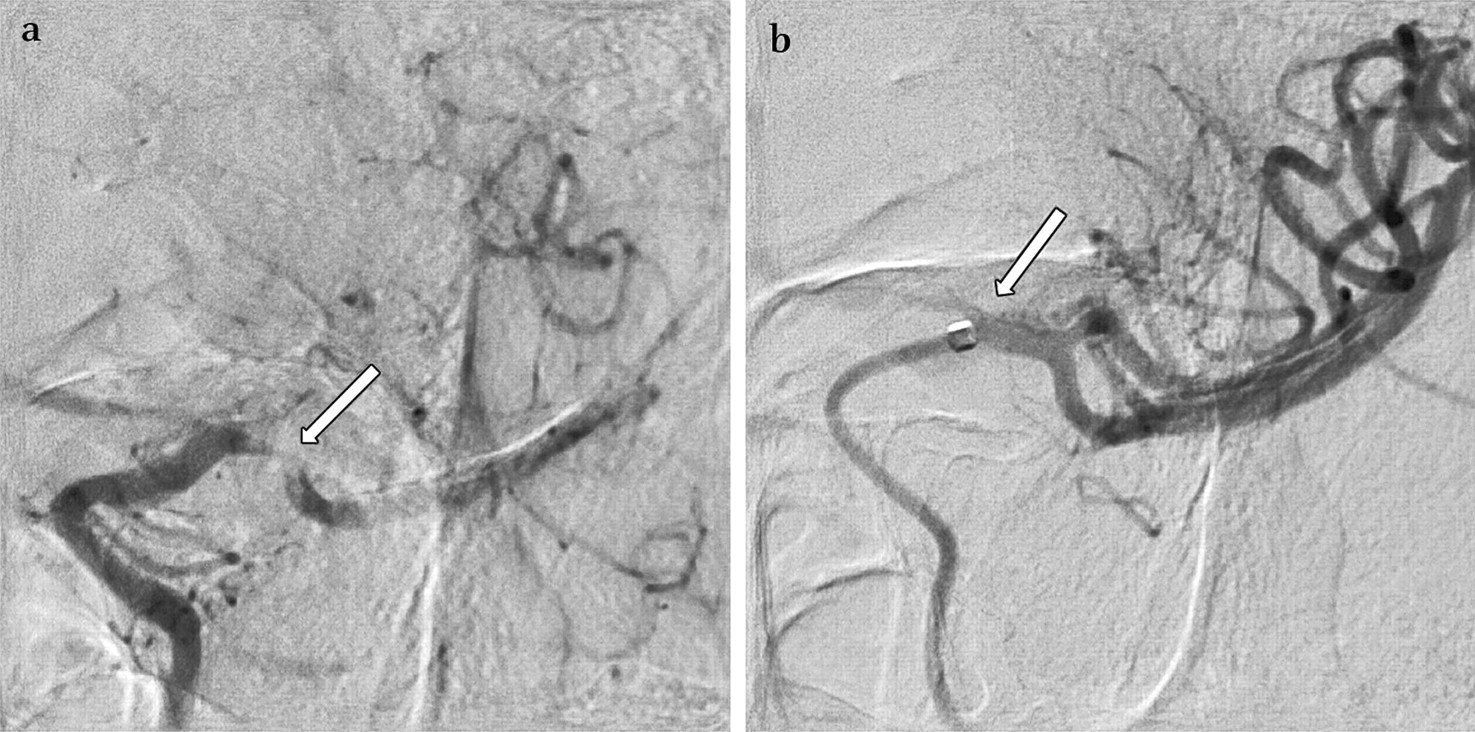
A 6F shuttle catheter was advanced to the left common carotid artery. A coaxial system of a 032 Penumbra aspiration catheter and 054 Penumbra aspiration catheter (Penumbra Inc, Alameda, California, USA) was advanced through the left ICA occlusion over a V18 microwire (Boston Scientific, Natick, Massachusetts, USA) and into the left supraclinoid ICA. A control angiogram was performed gently, demonstrating the left MCA subocclusive thrombus (figure 2A). The 054 catheter was advanced to the clot interface under fluoroscopy and the 054 separator device (Penumbra Inc) was deployed under aspiration for 15–20 s. Follow-up angiography performed at 11:30 (6 h after the initial event) demonstrated resolution of clot (figure 2B) TIMI 3. Neurological examination at this time demonstrated improvement in strength in the right arm and leg. The 054 catheter was then withdrawn into the distal cervical ICA with intermittent puffs of contrast to verify luminal patency.
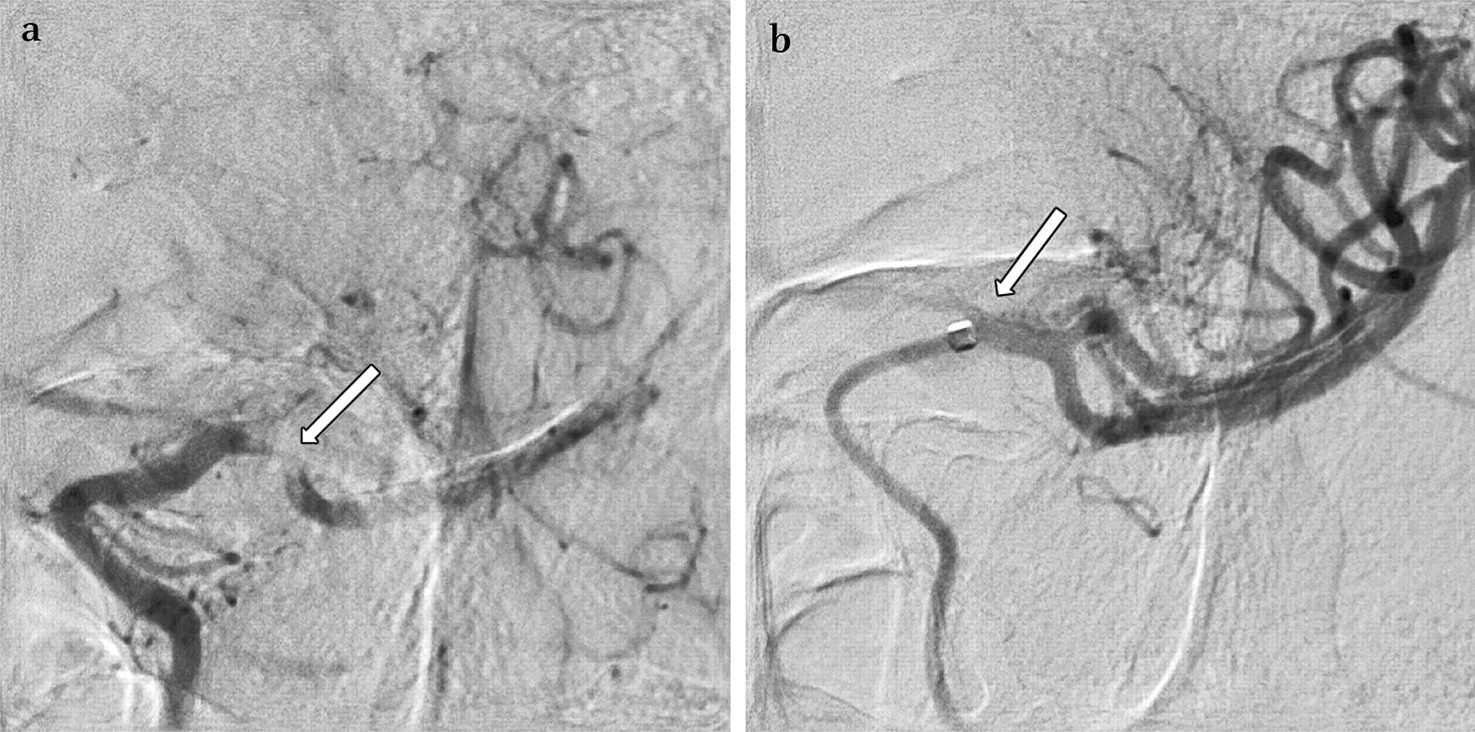
Injections through the Penumbra 054 aspiration catheter. (A) Subocclusive thrombus in the proximal M1 segment. (B) Resolution of the M1 thrombus after aspiration.
An Acculink EPD (Abbott Laboratories, Abbott Park, Illinois, USA) was deployed through the 054 catheter, maintaining access across the ICA occlusion. The 054 catheter was then removed and an Xact stent (Abbott Laboratories) was advanced over the EPD and placed across the ICA origin followed by angioplasty. A serpentine filling defect was noted distal to the ICA stent, limiting flow which prompted placement of an Xpert stent (Abbott Laboratories) over this region (figure 3).

Angiogram of the left internal carotid artery showing the appearance after stenting and angioplasty with two stents.
Follow-up angiography demonstrated loss of the left A1 segment (figure 4); however, due to the pre-existing stenosis in the left A1 segment as well as the good filling of the left ACA territory from the contralateral A1 segment, no revascularization of the left A1 was attempted. The EPD was removed, with macroscopically visible debris within the mesh.

Digital subtraction angiogram of the left common carotid artery showing loss of the left A1 segment (arrow).
The patient's aphasia and right-sided motor weakness resolved on the table with an NIHSS of 2 and minor paralysis of the face and mild dysarthria.
Postoperative course
The patient remained neurologically intact after the procedure with gradual resolution of his residual deficits. He was ultimately discharged with an NIHSS of 0. Ultrasound of the stented left ICA demonstrated no significant stenosis. MRI of the brain performed on the day of intervention showed minimal diffusion restriction foci.
Discussion
Tandem occlusions of the ICA origin and a distal branch vessel represent a difficult treatment challenge.1 Often in such cases there is an underlying atherosclerotic stenosis at the ICA origin that has occluded, generating an embolic thrombus that lodges in a distal vessel with stagnant blood between the ICA origin and the distal occlusion. Despite the availability of intravenous thrombolytic therapy, recanalization rates for tandem occlusions are poor, probably due to poor penetration of the thrombolytic agent.1
Some authors have advocated distal vessel treatments first, citing possible earlier restoration of flow to the end organ.2 However, if the MCA is treated first, the subsequent treatment of the ICA occlusion may result in embolism potentially putting previously normal territories (such as the posterior communicating artery (PCOM)/posterior cerebral artery (PCA) or ACA in cases of MCA occlusions) at risk. Other authors have documented proximal treatment first, citing potential benefits of increased proximal flow in autolysis of the distal occlusion and preservation of parenchyma (at risk by increasing perfusion pressure.3 While treatment of the ICA occlusion first may allow for retrieval by an intra-arterial device of embolic showers, there is also risk of stent damage during distal treatment. Regardless of the approach, treatment of a proximal internal carotid artery stenosis with angioplasty and stenting is necessary if acute stroke intervention of such patients is to be attempted.4–6
In this case, due to the presence of large anterior communicating artery and PCOM collaterals, it was felt that rapid removal of the MCA subocclusive clot would most immediately restore flow to the territory at risk. The use of a coaxial catheter access system reduced the ‘shelf’ effects of the relatively large leading surface of the 054 catheter, allowing smooth access across the ICA origin stenosis and clot, and navigation past the ophthalmic segment. The large inner diameter of the 054 may allow for more rapid clot extraction than the smaller Penumbra catheter systems, in this case with clot removal under 30 s. The ease of extraction may relate to the source of the embolism.7
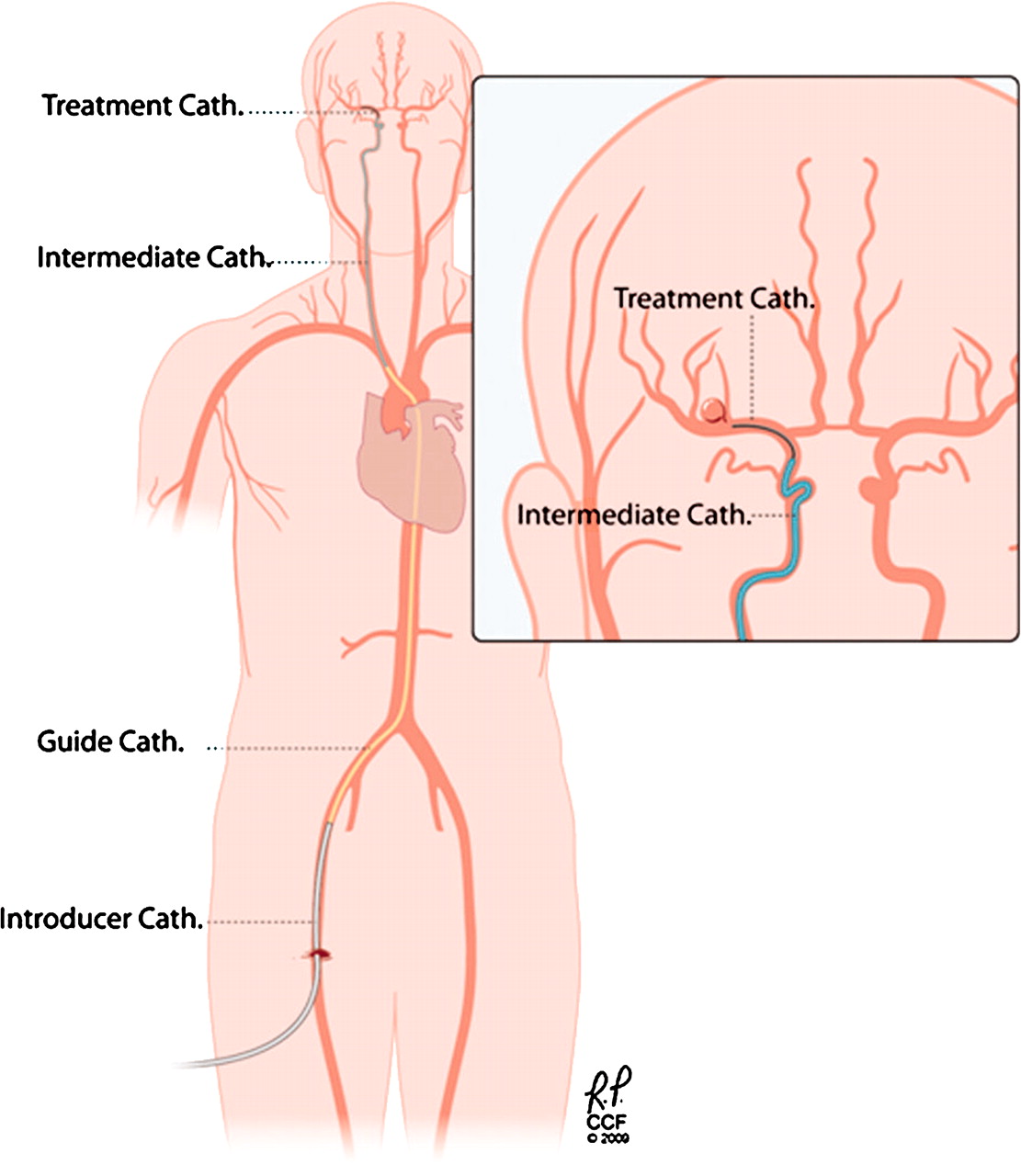
The 054 catheter was subsequently employed as an ‘intermediate catheter’, allowing deployment of an EPD distal to the clot and through the 054 catheter without needing to re-cross the lesion at the ICA origin (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram of the ‘intermediate catheter’ concept. In this case the Penumbra 054 served as an intermediate catheter, allowing rapid and safe placement of the embolic protection device.
The advantage to this approach to tandem lesions is that it allows an operator to employ both an EPD and distal clot access without ever losing control across the proximal occlusion site. In this case, the EPD trapped visually apparent debris. The occlusion of the A1 segment during stent deployment was felt to be related to failure of the EPD to completely eliminate distal emboli. However, stenting in the absence of an EPD may have resulted in even more emboli reaching the end organ. The placement of an EPD is not frequently used in carotid stenting in acute ischemic strokes as visualization of a target placement zone is limited. Moreover, it is difficult to steer the embolic protection device.6 However, using the Penumbra as an ‘intermediate catheter’ allowed for straightforward deployment of the EPD in a vessel segment angiographically clear of debris.
Proximal occlusion as an embolic protection regime has been described in carotid stenting in non-occluded carotids which avoids the hazards of traversing the occluded segment with the protection device.8 Flow reversal of the internal carotid has also been described,9 10 applied to carotid stenoses not occlusions. Some authors have employed dual balloon EPD techniques in high-risk carotid near-occlusions as well,11 which may improve efficacy in preventing distal embolic complications. The use of an EPD in carotid angioplasty and stenting of carotid stenoses may not, however, reduce embolic phenomena in carotid stenoses, which are predominantly microemboli.12 13 It is important to note that the type and size of emboli encountered in angioplasty of a carotid occlusion in the setting of an acute stroke may differ from that encountered in the angioplasty and stenting of carotid stenoses.
Patient selection remains the most challenging aspect of intervention in acute ischemic stroke. In this case, given that the patient's neurological examination was waxing and waning to such a large extent, it was felt that there was a significant territory that could be preserved.
Conclusion
Integration of an EPD may be a useful adjunct to the treatment of tandem occlusions in the setting of an acute ischemic stroke. By using the Penumbra 054 catheter or potentially a Distal Access Catheter (Concentric Medical, Mountain View, California, USA), it is possible to treat a distal lesion, place an EPD and stent a proximal lesion, all while maintaining access across the proximal occlusion site. Further study on the efficacy of such a technique and role is warranted.
Key messages
Optimum endovascular management for patients with ischemic stroke with tandem occlusions of the ICA bifurcation and intracranial thrombus has not been established. Techniques to first revascularize both distal and proximal occlusions have been described. A novel technique is described that crosses the proximal lesion only once, allowing access of the distal occlusion followed by carotid angioplasty and stenting with embolic protection.
Acknowledgments
The authors thank Christine Moore for her perseverance and editorial assistance.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Cleveland Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.