Article Text

Abstract
Inadvertent deformation and displacement of a fully deployed closed-cell intracranial nitinol stent may occur with manipulation of other devices through or beyond them. Such displaced and deformed stents may obstruct the lumen, risking formation of thromboemboli, and/or fail to no function as a scaffold to assist with coil embolization. We review two such cases whereby an Alligator retrieval device (ARD) (ev3, Irvine, California, USA) was used to salvage a deployed misshapen intracranial stent.
- Intracranial stent
- alligator retrieval device
- outreach catheter
- enterprise stent
- stent retrieval
- aneurysm
- catheter
- complication
- stent
- technique
Statistics from Altmetric.com
- Intracranial stent
- alligator retrieval device
- outreach catheter
- enterprise stent
- stent retrieval
- aneurysm
- catheter
- complication
- stent
- technique
Introduction
Since FDA approval in May 2007 of the first closed-cell intracranial nitinol self-expanding stent, the Enterprise stent (Codman, Miami Lakes, Florida, USA) has rapidly become a commonly used adjunctive device for endovascular aneurysm occlusion. However, publications on clinically relevant technical properties of this stent have been limited. Inadvertent deformation and displacement of a fully deployed closed-cell intracranial stent may occur with manipulation of other devices through or beyond them. Such displaced and deformed stents may obstruct the lumen, risking formation of thromboemboli, and/or fail to no function as a scaffold to assist with coil embolization. We review two such cases whereby an Alligator retrieval device (ARD) (ev3, Irvine, California, USA) was used to salvage a misshapen stent.
Clinical presentation
Case 1
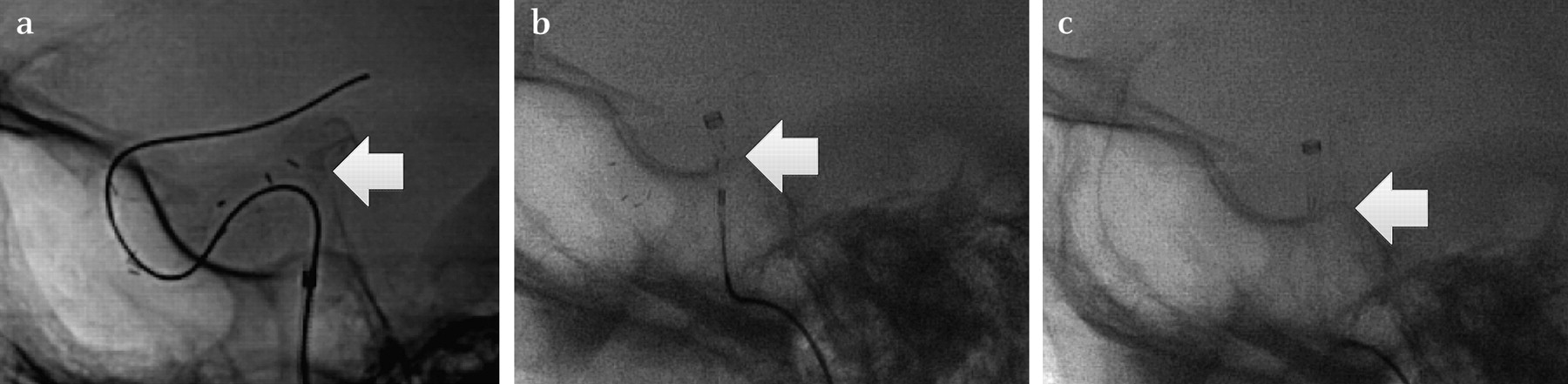
A 62-year-old woman underwent preventative aneurysm coil embolization using a 4.5 mm×22 mm Enterprise stent. The stent was inadvertently deployed proximal to the target lesion. Attempts to gain access to the aneurysm through this stent resulted in stent deformation, obstructing the vessel lumen. The proximal radio-opaque markers were splayed, suggesting a constricted, buckled stent (figure 1A). A microcatheter could not be advanced past the deformed stent.

(a) White arrow shows displaced proximal radio-opaque stent markers. (b) Proximal half of stent captured within distal access catheter with Alligator retrieval device seen by white arrow. (c) Distal radio-opaque stent markers within distal access catheter as seen by white arrow.
Case 2
A 61-year-old woman underwent coil embolization for a fusiform aneurysm dome remnant using a 4.5 mm×22 mm Enterprise stent, which was placed symmetrically across the aneurysm neck (figure 2A). Subsequent microcatheter selection of the aneurysm across the stent interstices led to stent deformation. The proximal radio-opaque markers were seen to constrict and migrate distally (figure 2B). The stent no longer functioned as an effective scaffold with attempts at coil embolization.

{kind=link}
{kind=link}
(a) Initial stent deployment symmetrically across aneurysm neck. (b) Stent buckling after selecting aneurysm dome with microcatheter. Proximal radio-opaque markers have moved as shown by white arrow. (c) After use of Alligator retrieval device, stent has reformed to its appropriate configuration as shown by the location of the proximal radio-opaque markers via the white arrow.
Intervention
Case 1
A Prowler Select Plus (PSP) (Codman, Miami Lakes, Florida, USA) microcatheter was advanced within a 5.2F Outreach (Concentric Medical, Mountain View, California, USA) catheter up and adjacent to the proximal edge of the stent. A 4 mm ARD was used to grasp the endoluminal portion of the stent. Using the ARD, we retrieved it directly into the 5.2F catheter (figure 1B and 1C). There was no resistance upon removal of the stent. Subsequent angiographic runs showed no vessel injury. Stent-assisted coil embolization was then completed.
Case 2
A PSP microcatheter was advanced to the proximal end of the stent. A 2 mm ARD was used to grasp the proximal edge of the stent and gently pull it until the radio-opaque markers were visualized to expand and fully appose the vessel wall (figure 2C). Coil embolization was then completed.
Conclusion
One challenge associated with using the currently available self-expanding intracranial stents is the limited radiographic visibility of the stent conformity to the vessel wall. Preliminary clinical experience with the Enterprise stent in 14 patients reported poor visibility after deployment as a notable limitation.1 Ebrahimi et al2 addressed the poor in vivo visibility and used a Flat-Panel CT (FPCT) to evaluate stent mechanics in a curved vessel in vitro model and found that when a closed-cell stent design like the Enterprise is bent, it has less flexibility to conform to a curved or irregular anatomy. The unsegmented stent design does not allow the stent to lengthen at the outer curve, or to shorten at the inner curve. This leads to flattening of the stent, and with increasing curves, the possibility of stent kinking or buckling. In vivo, these properties should raise concern for stent buckling if the aneurysm has a wide neck located on a tortuous segment.
In addition to the poor visibility and difficulty conforming to the lumen around curves, there have been reports of spontaneous stent migration. This finding is thought to be related to the closed-cell design, which allows for force transmitted onto one end to be transmitted to the entire device.3 A 14 mm length Enterprise stent was observed to spontaneously migrate proximally, as discovered on 5-month surveillance angiography. Stent migration during microcatheter selection of the aneurysm after full deployment was reported by Lubicz et al1 but fortunately it remained across the aneurysm neck to allow for successful coil embolization and no adverse clinical sequelae.
Therefore, because of its poor fluoroscopic visibility, lack of vessel conformity around curves and inherent susceptibility to migration, the radio-opaque markers must be carefully observed during manipulation of any device within or through the Enterprise stent. Because of this delicate property, some operators prefer to stage coil embolization at some interval after stent placement to allow for stent stabilization.
In the first case, having large inner lumen distal access catheters allowed for stent removal immediately at the exact lesion site without having to drag the device for any length along the artery lumen. Fortunately, the delicate properties that predispose the stent to deform also allow for ease of removal in that the stent folds on itself without overlapping and/or forming a knot. A Neuroform stent (Boston Scientific, Natick, Massachusetts, USA) tangled with a coil was reported to be ensnared with a Merci retrieval device (Concentric Medical, Mountain View, California, USA) but involved dragging the implants adjacent to the tip of the guide catheter out of the body, resulting in fracture of the retriever device and stent in the femoral artery.4
The ARD has been previously reported to retrieve intracranial aneurysm coils,5 cerebral thromboemboli6 and coronary stents,7 8 but never intracranial stents. It is made from a 0.016 inch stainless steel insertion wire with four precision grasping arms attached to its tip. The ‘jaws’ are deployed proximal to the target, the entire unit is advanced and the microcatheter is then advanced, forcing the jaws to close circumferentially, engaging the target.
In both instances, the constricted, endoluminal portion of the stent and the non-overlapping design allowed for relative ease of stent removal and repositioning. The ARD enables precise repositioning of the stent but visualization is limited to the configuration of the radio-opaque stent markers. The ARD has the strength to grasp the stent, and with the availability of distal access catheters, stent removal is a viable option if needed. As a bailout method, the ARD allowed for safe endovascular stent removal in the first case, and repositioning in the second case.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Rush University Medical Center Retrospective Stroke Registry ID 07110702.
Provenance and peer review Not commissioned; externally peer reviewed.