Article Text

Abstract
Background Cerebral venous sinus thrombosis (CVT) is an uncommon cause of stroke that is usually treated medically with intravenous heparin therapy followed by long-term anticoagulation therapy. A series of patients with CVT who underwent rheolytic thrombectomy with the AngioJet as a first-line adjunctive treatment in addition to standard anticoagulation therapy is presented.
Methods Prospectively maintained endovascular databases at two institutions were retrospectively reviewed. The available clinical and imaging data were compiled at each institution and combined for analysis.
Results Over 18 months, 13 patients (seven women and six men; age range 17–73 years, median age 45 years) with CVT were treated with rheolytic thrombectomy. Immediate (partial or complete) recanalization of the thrombosed intracranial sinuses was achieved in all patients. At a median radiographic follow-up of 7 months there was continued patency of all recanalized sinuses. Clinical follow-up was available on nine patients: modified Rankin score of 0 in four patients, 1 in three patients and 6 in two patients.
Conclusion This series demonstrates the feasibility of performing mechanical thrombectomy as a first-line treatment for acute CVT. This technique facilitates the prompt restoration of intracranial venous outflow, which may result in rapid neurological and symptomatic improvement.
- Venous sinus thrombosis
- rheolytic thrombectomy
- angiography
- aneurysm
- arteriovenous malformation
- artery
- spinal cord
- thrombectomy
- navigation
- complication
- thrombolysis
- angioplasty
- vascular malformation
- orbit
- pediatrics
- subarachnoid
- cervical
- lesion
- tumor
Statistics from Altmetric.com
- Venous sinus thrombosis
- rheolytic thrombectomy
- angiography
- aneurysm
- arteriovenous malformation
- artery
- spinal cord
- thrombectomy
- navigation
- complication
- thrombolysis
- angioplasty
- vascular malformation
- orbit
- pediatrics
- subarachnoid
- cervical
- lesion
- tumor
Cerebral venous sinus thrombosis (CVT) is an uncommon but potentially devastating cause of stroke. Once clot forms within the venous sinus it can propagate quickly, obstructing venous outflow. The resulting venous congestion can lead to incapacitating headache, hemorrhagic infarction and potentially neurological decline or even death. The mainstay of treatment for CVT has been systemic anticoagulation, which can lead to recanalization and symptomatic improvement within days to months.
In some cases, progressive neurological decline may occur in patients with CVT despite intravenous heparin therapy. In these patients, direct intrasinus infusion of thrombolytic agents may be an effective treatment. This approach may require several days to work and may increase the risk of hemorrhagic complications, especially in patients with pre-existing hemorrhagic venous infarction. Several case reports and small case series have recently reported the usefulness of the AngioJet Rheolytic Thrombectomy System (Possis Medical, Minneapolis, Minnesota, USA), a peripheral vascular and coronary thrombectomy device, to achieve revascularization of the venous sinuses in patients refractory to standard medical therapy and in those with a rapidly deteriorating neurological status. We report our experience using the AngioJet system as first-line therapy for the treatment of CVT.
Materials and methods
We retrospectively reviewed prospectively maintained endovascular databases at our two institutions. Between January 2009 and July 2010, 13 consecutive patients with CVT (seven women, six men; median age 45 years, age range 17–73) were treated with the Angiojet mechanical thrombectomy system. Patients who were treated with anticoagulation without endovascular neurosurgery consultation were not included. Informed consent for the procedures was obtained from each patient (or family member). Available imaging studies and clinical data were reviewed for all patients. Data were compiled for each institution and combined for analysis. At each institution, approval was obtained from the Institutional Review Board for retrospective chart review and data sharing.
At presentation, six patients had non-disabling symptoms (headache with or without double vision) and seven patients presented with significant neurological decline. The average clinical follow-up was 5 months (range 2 weeks to 9 months) and was available in seven patients. Radiographic follow-up was based on CT venography and magnetic resonance venography.
Technical considerations
All patients were treated under general anesthesia. 5 Fr and 8 Fr sheaths were placed in the femoral artery and vein, respectively. Intravenous heparin (100 units/kg) was administered with the goal of an activated clotting time of 250–300 s. Bilateral carotid angiograms were performed with attention to the venous phase to delineate the extent of the venous sinus thrombosis. A 5 Fr diagnostic catheter was introduced over a 0.035 inch exchange Glidewire (Terumo Medical Corp, Somerset, New Jersey, USA) through the common femoral vein, cannulating one of the internal jugular veins. The Glidewire was guided into the jugular bulb and into the sigmoid sinus. The diagnostic catheter was then exchanged for a coaxial system consisting of a 6 Fr KSAW Shuttle sheath (Cook, Indianapolis, Indiana, USA), Neuron 070 delivery catheter (Penumbra, Alameda, California, USA) and Neuron 5 Fr Berenstein select catheter (Penumbra). The Shuttle sheath was manipulated over the Neuron delivery and select catheters and the Glidewire into the intracranial venous sinus system. The distal position of the KSAW sheath in the venous sinuses is very important for successful deployment of the AngioJet system. Depending on the venous vascular anatomy, the KSAW Shuttle sheath could travel as far distally as the mid-transverse sinus. The Neuron catheters were then removed and a microcatheter was introduced over a 0.014 inch micro-guidewire to further traverse the occluded sinus segments. The microcatheter was exchanged over a 0.014 inch extra-support exchange length microwire. Finally, a 4 Fr or 5 Fr AngioJet catheter was introduced over the microwire. With the distal position of the KSAW Shuttle sheath providing good support, the AngioJet catheter can be delivered as far as the anterior third of the superior sagittal sinus, as well as across the midline and into the contralateral transverse and sigmoid sinuses. Occasionally the KSAW Sheath could not be maneuvered past the jugular bulb because of tortuous anatomy, making delivery of the AngioJet system more difficult. The 6 Fr AngioJet catheter was used in cases with massive clot burden, but its use required an exchange length 0.035 inch Glidewire as a platform.
The AngioJet device was activated to initiate rheolytic thrombectomy and slowly withdrawn through the clot. A powerful heparinized saline (4 units/ml) jet streamed through the distal orifice of the catheter, creating a low-pressure zone around the catheter tip via the Bernoulli effect. This vacuum effect drew the thrombus to the catheter inflow zone where it was fragmented and evacuated from the body through the catheter.
After treatment, patients were typically transitioned from intravenous heparin to coumadin or low molecular weight heparin for 3–6 months.
Results
Most patients had a risk factor for developing a hypercoagulable state (three patients smoked and one each had an infection of the CNS, ulcerative colitis, Factor V Leiden and protein S deficiency, HIV infection or Sjogren syndrome). One patient was postpartum and one was receiving hormone replacement therapy.
The superior sagittal sinus was involved in nine of the 13 cases. Thrombus extended down into the internal jugular vein in five cases. Sinus thrombosis was unilateral in seven cases and bilateral in six cases. Immediate partial and complete recanalization of the thrombosed intracranial sinuses was achieved in seven and six patients, respectively. In one patient (8%) the sinus re-occluded on the day after the procedure. At a median radiographic follow-up of 7 months there was continued patency of all recanalized sinuses.
The Glascow Coma Scale on admission was 3T, 10T in three patients, 14 in two patients and 15 in seven patients. The predominant symptoms on presentation included coma (n=1), significant weakness (n=3), confusion (n=3) and double vision (n=2). Patients were neurologically unchanged immediately after mechanical thombectomy but made variable improvements during the hospitalization; two of the three patients with weakness improved, as did two of the three patients with confusion. In the two patients with double vision, this was unchanged postoperatively but had resolved at the latest clinical follow-up. After undergoing thrombectomy, all six patients who presented with severe headache experienced complete and immediate resolution of their headache.
Clinical follow-up was available on nine patients; the modified Rankin score was 0 in four patients, 1 in three patients and 6 in two patients. Of the seven patients who presented with a neurological deficit, five showed clinical improvement at the latest follow-up. Two patients died in the perioperative period, one as a result of re-occlusion of her thrombosed sinuses and another patient who had presented with a GCS of 3T died from multiple organ failure caused by sepsis. The only operative complication was an asymptomatic perforation of a cerebellar vein from microwire manipulation.
Illustrative case
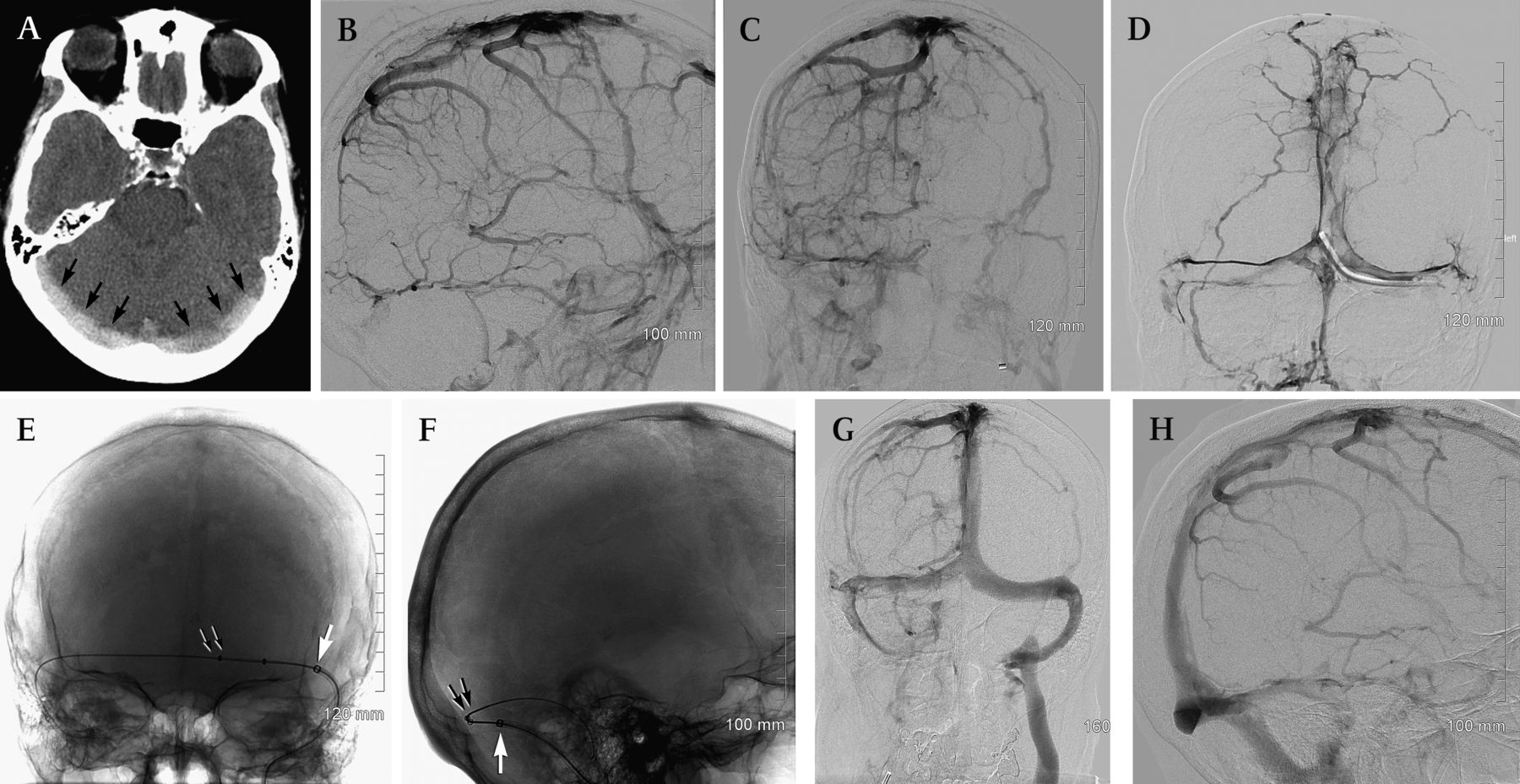
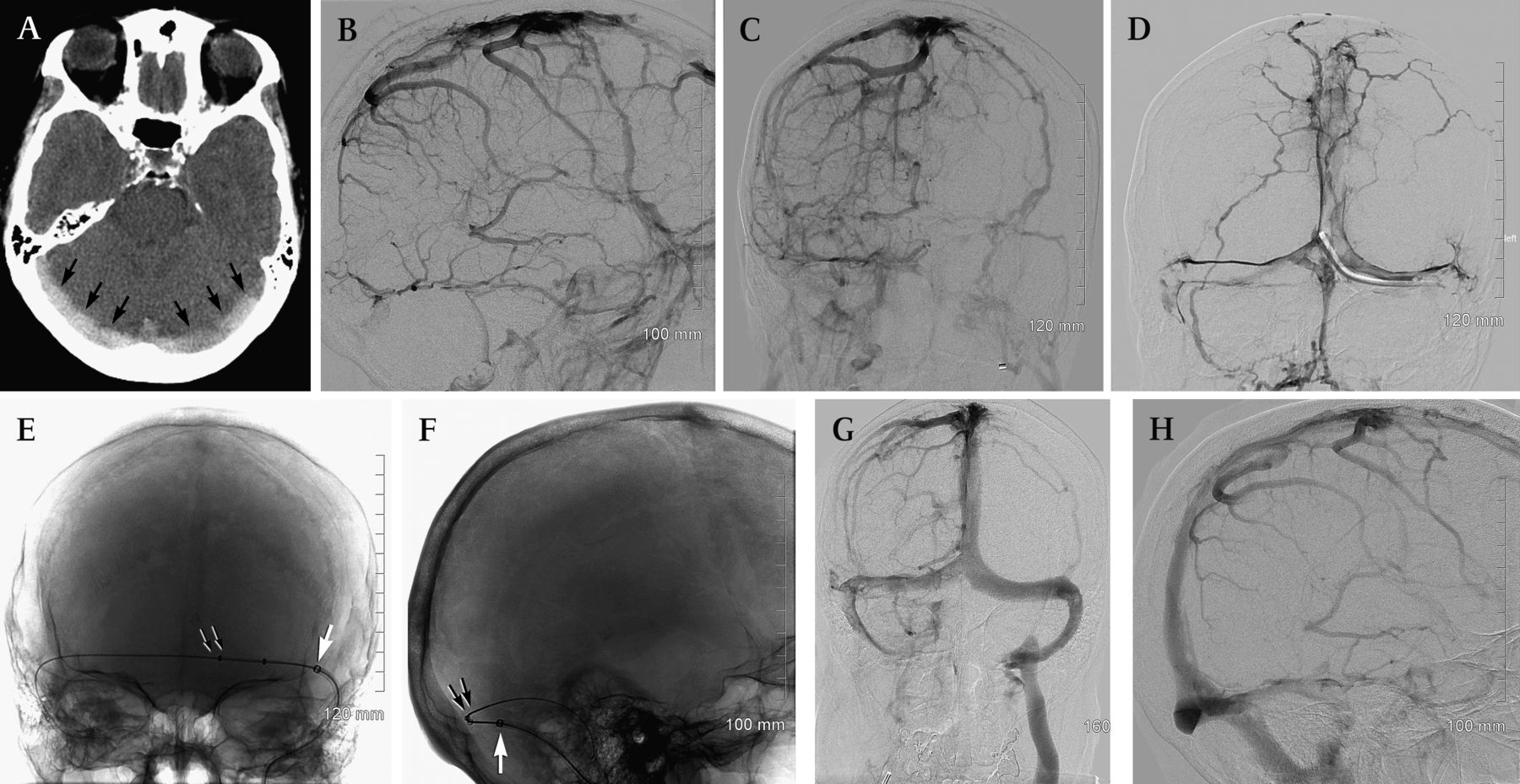
A woman in her mid 50s with a history of treatment for Sjorgen syndrome developed sudden onset of a severe occipital headache (figure 1). An axial CT scan of the head without contrast showed acute thrombus within the venous sinuses (figure 1A). Cerebral angiography showed complete occlusion of the posterior half of the superior sagittal sinus, both torcular sinuses, both straight sinuses and both internal jugular veins (figure 1B,C). A torcular venogram showed complete venous sinus thrombosis without distal run-off (figure 1D). The 6 Fr KSAW shuttle catheter was positioned at the junction of the left torcular and straight sinuses (figure 1E,F). The 6 Fr AngioJet catheter was then delivered over a 300 cm stiff Glide exchange wire. An angiogram obtained after use of the AngioJet showed complete recanalization of the venous sinuses (figure 1G,H). The patient had immediate and complete relief from her headache in the recovery room. She was transitioned from intravenous heparin to coumadin for 6 months. Magnetic resonance venography performed after 6 months confirmed continued patency of all sinuses and the patient remained symptom-free.
{kind=link}
A woman in her mid 50s with a history of Sjorgen syndrome presented with sudden onset of a severe occipital headache. Axial CT scan of the head without contrast (A) shows acute thrombus within the venous sinuses (arrows). Cerebral angiogram, right internal carotid artery injection, venous phase, lateral (B) and posteroanterior views (C) show complete occlusion of the posterior half of the superior sagittal sinus, both transverse sinuses, both sigmoid sinuses and both internal jugular veins. Torcular venogram (D) shows venous sinus thrombosis without distal run-off. Posteroanterior (E) and lateral (F) native views of the skull show the 6 Fr KSAW shuttle catheter at the junction of the left transverse and sigmoid sinuses (white arrow). The 6 Fr AngioJet catheter (double arrows) was delivered over a 300 cm stiff Glide exchange wire. Right internal carotid artery angiograms, venous phase, after AngioJet mechanical thrombectomy, posteroanterior (G) and lateral (H) projections show complete recanalization of the superior sagittal sinus, both transverse sinuses, both sigmoid sinuses and the left internal jugular vein. Used with permission from Norton Neuroscience Institute.
Discussion
Systemic anticoagulation
In 1991 Einhaupl and colleagues published their seminal paper detailing a small randomized controlled trial which compared administration of placebo with intravenous heparin for the treatment of CVT.1 The results were so strikingly in favor of anticoagulation therapy that the trial was stopped early. The authors concluded that intravenous heparin was an effective treatment for CVT, even in the setting of intracranial hemorrhage. However, the extent of recanalization of CVT treated with systemic anticoagulation has not been defined. Several small case series have shown only partial recanalization.2 ,3 In a prospective observational study of 12 consecutive patients with CVT treated with at least 6 months of anticoagulation therapy, six patients had incomplete recanalization and three patients achieved full sinus recanalization.4
The International Study on Cerebral Vein and Dural Sinus Thrombosis, a multicenter prospective observational study of 624 patients published in 2004,5 shed some light on the natural history of CVT treated with systemic anticoagulation. Most patients (83%) were treated with anticoagulation therapy. At a median follow-up of 16 months, 79% had recovered completely or had minor residual symptoms, 7.5% had mild impairment and 13.5% had died or were disabled. Multivariate predictors of death or dependence were male gender, age older than late 30s, coma, decreased mental status, involvement of the deep venous system, hemorrhage on admission CT scan, infection and cancer.
Chemical thrombolysis
With the role of intravenous heparin clearly established, direct infusion of tissue plasminogen activator (t-PA) into a thrombosed venous sinus was the natural next step in the treatment of CVT, mimicking the clinical experience with intra-arterial t-PA infusion for acute stroke. Frey et al reported at least partial recanalization in 9 of 12 patients treated with intrasinus t-PA infusion combined with intravenous heparin.6 Two of the three patients who failed recanalization, however, experienced significant worsening of their intracranial hemorrhage. The authors concluded that direct t-PA infusion is unsafe in patients who become symptomatic with obvious hemorrhage. Soleau et al similarly treated 10 patients with continuous chemical thrombolysis over 1–5 days.7 Although sinus patency was restored in 90% of the patients, the incidence of hemorrhagic complications was 30%.
Mechanical thrombectomy
Again paralleling our current treatment for acute arterial occlusive disease, the next logical step in the treatment of CVT is mechanical thrombectomy. This method is especially appealing because dural-covered venous sinuses are much more durable than intracranial arteries. Many mechanical thrombectomy devices have been used to treat venous sinus thrombosis with limited effectiveness.7 Recently, off-label use of the AngioJet thrombectomy device has shown promise in a handful of cases.8–13 The device is approved by the Food and Drug Administration for the treatment of coronary arteries as small as 2 mm in diameter as well as for saphenous vein grafts. It has also been used effectively to perform peripheral venous thrombectomy and pulmonary embolectomy.14–29
AngioJet relies on the Bernoulli effect created by streaming a high-pressure saline jet through the device. In fluid dynamics, Bernoulli's principle states that, for non-viscous fluid flow, an increase in the speed of the fluid is coupled with a decrease in pressure or a decrease in the potential energy of the fluid.30 In effect, a vacuum is created and captures the thrombus within the catheter where it is pulverized and removed from the body. In this manner, vascular patency can be restored within minutes.
Eight cases have been reported in which the transfemoral AngioJet was used for mechanical thrombolysis of CVT. Early reports combined the use of AngioJet mechanical thrombectomy with direct infusion of a thrombolytic agent.8–13 Chahlavi and colleagues reported their experience with craniotomy and direct puncture of the torcula for delivery of the AngioJet catheter and cited difficulty obtaining transfemoral access.31 Until now, Kirsch et al had published the largest series—four patients with CVT treated with the AngioJet device.32 Their patients were fully anticoagulated but no chemical thrombolytic agents were used. In all four patients, blood flow within the venous sinuses was restored. There were no procedural complications. Three patients had an excellent clinical outcome. One patient died despite sinus recanalization.
In these previous reports the AngioJet device was used as a last resort exclusively for patients who failed to improve or whose condition deteriorated while on intravenous heparin. We used the AngioJet device in 13 patients, but with two important differences. First, we had the benefit of recent improvements in AngioJet catheter technology. Its lower profile, more flexible catheters and hydrophilic coating now allow much easier and safer access to the venous sinuses. Second, we used the AngioJet device as first-line treatment in combination with intravenous heparin.
There are several reasons to consider AngioJet sinus thrombectomy as first-line treatment. First, it appears to be relatively safe. No symptomatic procedure-related complications associated with the use of AngioJet in the treatment of CVT (10 previously reported cases as well as our series of 13 patients) have been reported. Second, the technique is associated with a high rate of technical success. Finally, the technique offers the opportunity to achieve prompt resolution of venous occlusion and neurological sequelae compared with other treatments. In contrast, a bail-out strategy of mechanical thrombectomy in patients who fail anticoagulation may be too little too late in some cases.
We hypothesize that the immediate restoration of physiologic venous outflow is beneficial. Mechanical evacuation of thrombus and restoration of flow quickly reduce the total volume of venous thrombus burden and prevent stasis and further propagation of thrombus. These advantages augment the efficacy of systemic anticoagulation therapy with heparin. Once blood flow is restored, venous hypertension and vascular congestion are relieved. The more quickly this relief is achieved, the shorter is the length of time that normal brain tissue is exposed to the deleterious effects of abnormal vascular pressure, which can affect cerebral perfusion. Furthermore, the symptoms of venous sinus occlusion, which may consist of severe headache, focal neurological deficits or both, may be resolved more quickly than treatment with anticoagulation therapy alone. Potentially, this advantage could result in shorter hospitalizations and a shorter duration of disability.
A more conservative approach could stratify patients according to risk. Patients at high risk for a poor outcome (male gender, advanced age, presence of infection or cancer, intracranial hemorrhage, coma or mental status change) would undergo AngioJet thrombolysis. The remaining patients would be treated with anticoagulation therapy alone. Mechanical thrombectomy would then be reserved for patients who deteriorate despite adequate anticoagulation therapy. The obvious drawback of this strategy is the significant delay it would create in definitive treatment if heparin fails.
Despite these encouraging results, it is important to acknowledge that the application of the Angiojet system for the treatment of CVT represents an off-label use. There are anatomic limitations to the use of the Angiojet system. For example, cerebral veins such as the veins of Trollard and Labbe may be affected by clot extension but would not be amenable to thrombectomy because of a higher risk of hemorrhage. These veins, however, may have a higher chance of recanalization if the venous sinus clot burden is reduced through thrombectomy, allowing increased circulation of the anticoagulated blood in the intracranial venous system. Although no clinically significant complications were encountered in our series, there are potential risks of which the operator should be aware. Perforation of veins or venous sinuses with subdural hemorrhage is always a possibility. Hemolysis of the thrombus can increase the probability of acute renal dysfunction related to obstructive nephropathy. Pulmonary embolism can occur during or after the procedure. These emboli are related to the disruption of the thrombus, which causes the clots to flow distally from the dural sinuses into the pulmonary vasculature. Theoretically, arterial ischemic stroke can occur if the patient has an undetected patent foramen ovale and thrombus is diverted intra-arterially during and after the procedure.
Conclusion
The mainstay of treatment for venous sinus thrombosis has been systemic anticoagulation therapy. More invasive endovascular approaches have been used only in a handful of cases as a last resort. The current series provides preliminary evidence in support of the efficacy and safety of mechanical rheolytic thrombectomy as a first-line treatment for acute CVT. In our series, this strategy promptly restored intracranial venous outflow with rapid symptomatic and neurological improvement in some patients. It would take a randomized multicenter controlled trial to prove superiority of mechanical thrombectomy over systemic anticoagulation for the treatment of CVT, but patient accrual may be a problem because of the rarity of the disease.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by St Joseph's Hospital and Western IRB.
Provenance and peer review Not commissioned; externally peer reviewed.