Article Text

Abstract
The pipeline embolization device (PED) is a revolutionary tool for the endovascular treatment of intracranial aneurysms by flow diversion. Treatment using the PED often requires considerable manipulation and customization by the neurointerventionalist at the time of deployment. Proper use of the PED involves a novel set of techniques and associated jargon, which must be learned by all neurointerventionalists, fellows and residents for safe treatment of patients with this device. In this report, the PED removal techniques referred to as ‘corking’ and ’pseudo-corking’ are described. Corking is used for the removal of a partially deployed in situ PED when the pusher wire is intact whereas ‘pseudo-corking’ is used if the pusher wire is fractured or disconnected. Knowledge of both techniques is necessary for withdrawing the PED in situations of malposition or failed expansion.
Statistics from Altmetric.com
Introduction
The pipeline embolization device (PED; Covidien Vascular Therapies, Mansfield, Massachusetts, USA) is a low porosity, stent-like device that achieves aneurysm obliteration via flow diversion and eventual parent vessel remodeling.1–5 Deployment of this device is unlike that of other currently available intracranial stents. PED placement is often technically challenging, and it requires specific maneuvers to assure proper expansion of the device and also to customize the density of the struts across the aneurysm neck. Safe and effective enactment of these specialized techniques requires teaching not only the manual skills but also a fluency in the associated new terminology used to describe them.
In certain circumstances, PED deployment is non-ideal and despite exhaustion of salvage techniques, removal of the device is desirable. Such is the case if mechanical or technical failure prevents the distal, mid or proximal portions of the device to fully open. Similarly, malposition of the device may prompt the neurointerventionalist to remove the device and start fresh. In this report, the authors describe removal of a partially deployed PED using techniques called ‘corking’ and ‘pseudo-corking’.
Technique description and case examples
To date, over 50 PEDs have been deployed at the institution of the senior author (ALC). Five of these have required in situ removal of the device (table 1). Two PEDs were removed for failed mechanical deployment of the distal PED (table 1, cases Nos 1 and 2) and one device was removed for failed mechanical deployment of the mid-portion of the device (table 1, case No 3). One PED (table 1, case No 4) was removed after the distal device dislodged into the aneurysm sac and the anchor point for a planned telescoping construct was lost (successful deployment was subsequently achieved on the second attempt). This case is illustrated in detail in figure 1 and in videos 1–3 (videos 1–3 are available online only). One PED (table 1, case No 5) was removed after the distal portion of the device deployed proximal to the aneurysm neck. All of the devices were removed safely and without incident.
Four cases of corked PEDs and one case of pseudo-corking
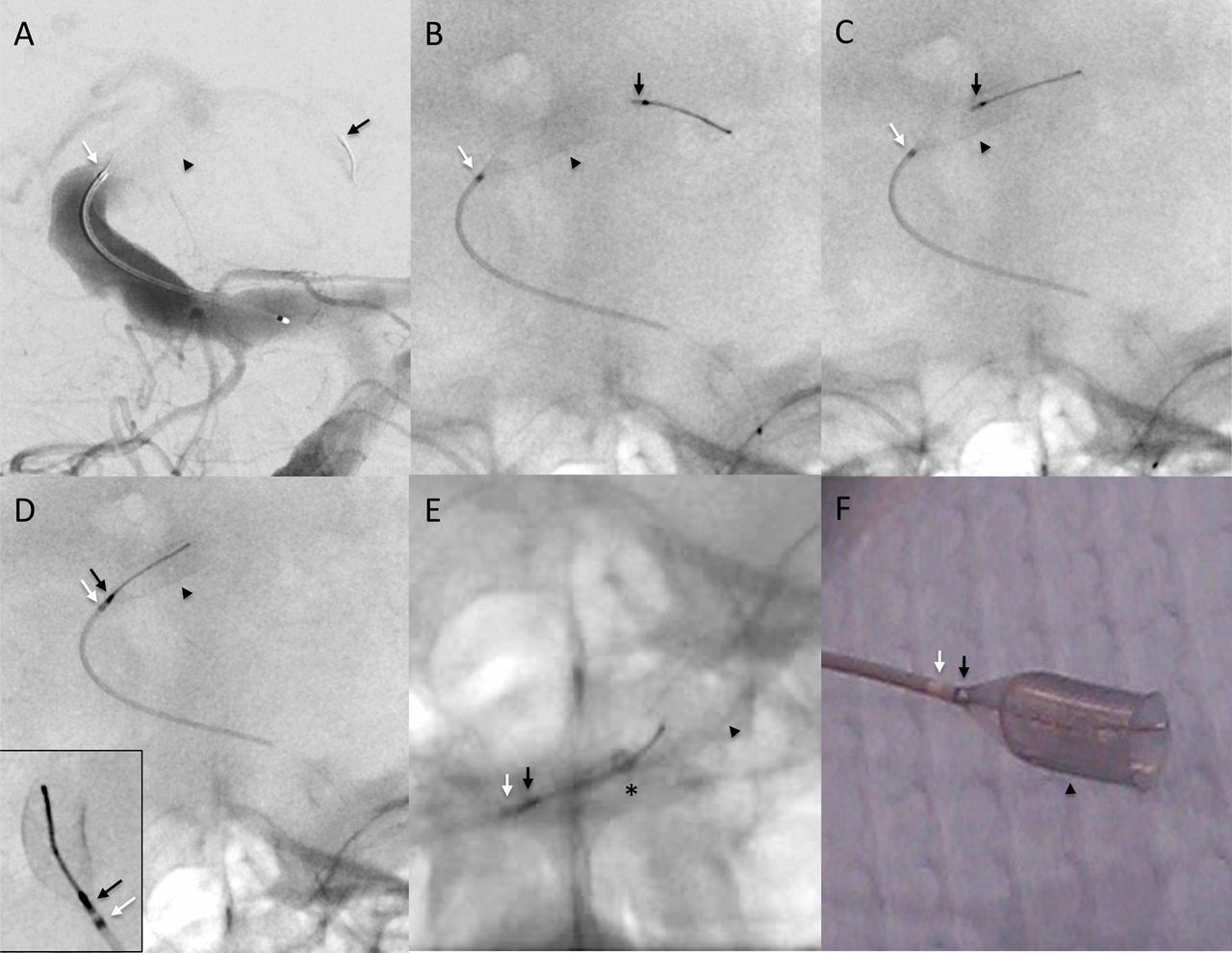
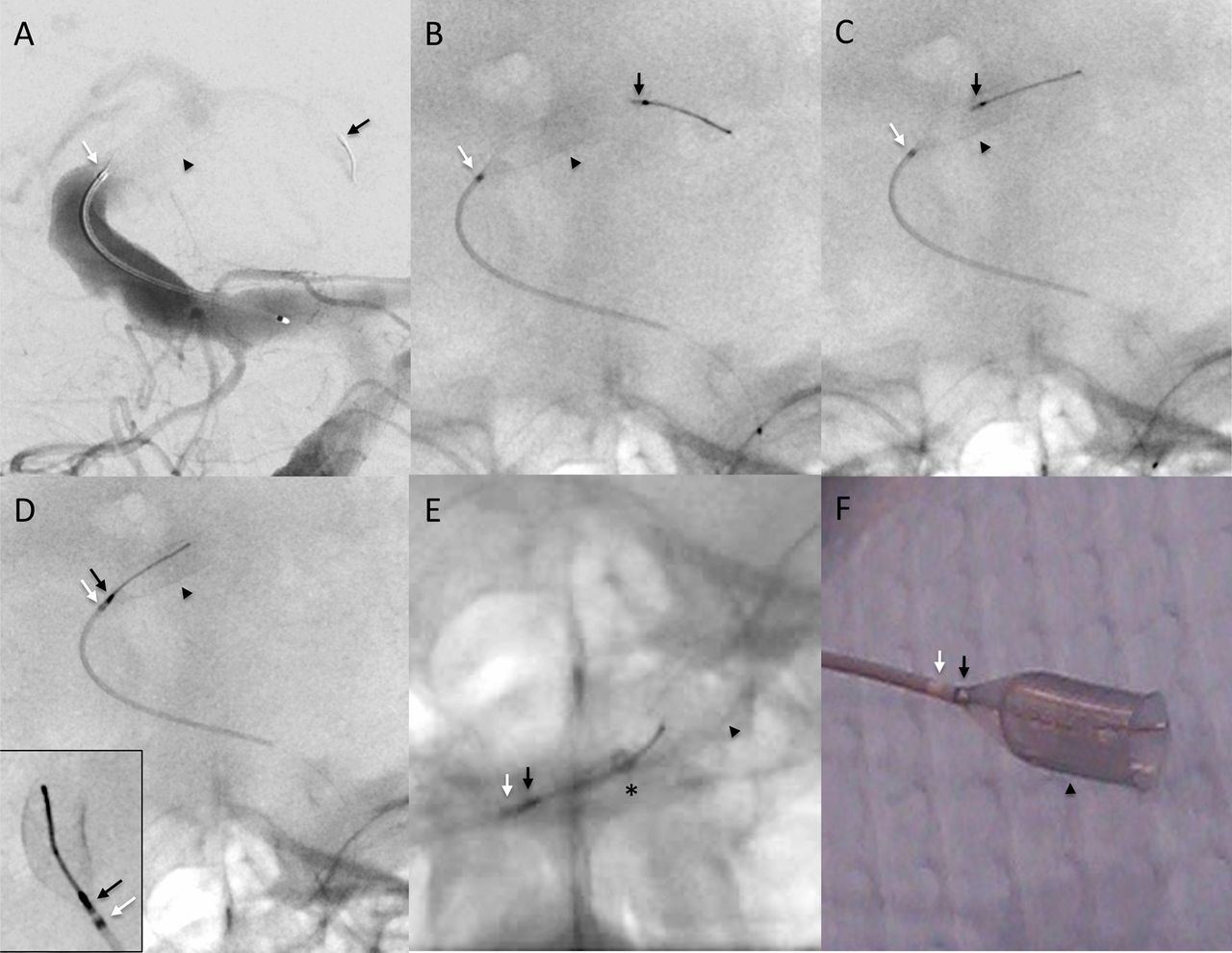
Corking and removal of a 5 mm × 35 mm pipeline embolization device (PED) from a basilar aneurysm. (A) Right vertebral artery digital subtraction angiograph run (anteroposterior plane). The distal PED (arrowhead) is fully expanded in the basilar artery aneurysm. The protective/capture coil and distal bumper (black arrow) is positioned in the left posterior cerebral artery. The white arrow represents the distal marker of the Marksman 0.027 inch microcatheter. (B, C) Fluoroscopy demonstrating that the corking process is initiated by withdrawing the protective/capture coil into the lumen of the PED. (D) Corking is complete when the protective/capture coil reaches the distal marker of the microcatheter (inset=magnified lateral view). (E) The corked PED and Marksman microcatheter are partially withdrawn into the distal tip of the 5 Fr ReFlex 0.058 inch guide catheter. These devices were subsequently withdrawn through a 6 Fr Flexor Shuttle Select Guiding Sheath (Cook Medical, Bloomington, Indiana, USA) positioned in the right subclavian artery (not shown, see video 3, available online only). (F) Photograph of the corked PED and distal Marksman microcatheter.
In Nos cases 1–4 listed above, removal of the partially deployed PED was accomplished via a technique called ‘corking’. Corking refers to the act of withdrawing the PED pusher wire so that the protective/capture coil engages the PED as it exits the distal microcatheter (figure 1B, D) (see also videos 1A, B, available online only). This effectively pins the open PED against the distal microcatheter lumen with the PED protective/capture coil serving as the ‘cork’. Under fluoroscopy, corking is complete when the protective/capture coil is visualized adjacent to the distal marker on the microcatheter. Care must be taken when withdrawing the bumper/protective coil through the distal end of the PED to prevent the bumper/capture coil from getting caught on and everting the PED edge. An everted edge would be more prone to endothelial damage when the PED is removed.
After the PED is corked, the PED and microcatheter can be removed as a single unit (figure 1E and video 2, available online only). Of note, the PED can undergo considerable lengthening as it is withdrawn, particularly if most of the PED is already deployed prior to corking and if the device is being withdrawn around a sharp turn in the vessel. Once the PED is freed from its position, the corked PED and microcatheter can be removed easily as a unit through a 6 French (Fr) guide catheter, such as the Neuron 0.070 inch inner diameter (ID) catheter (Penumbra Inc, Alameda, California, USA). However, the guide catheter must also be removed if a 5 Fr system is used (video 3, available online only), such as the DAC 0.057 inch ID (Concentric Medical Inc, Mountain View, California, USA) or the ReFlex 0.058 inch ID catheter (Reverse Medical Corporation, Irvine, California, USA).
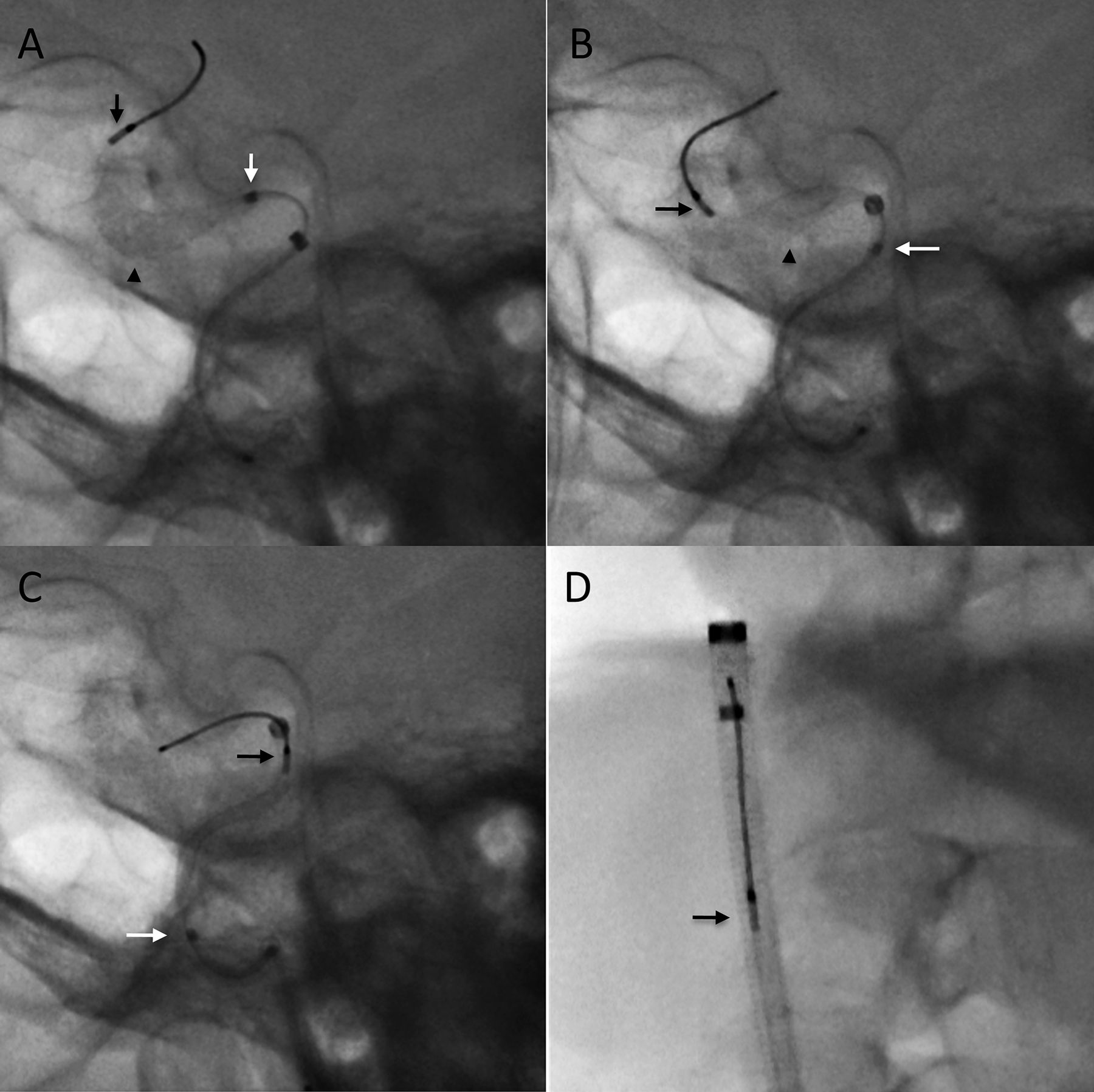
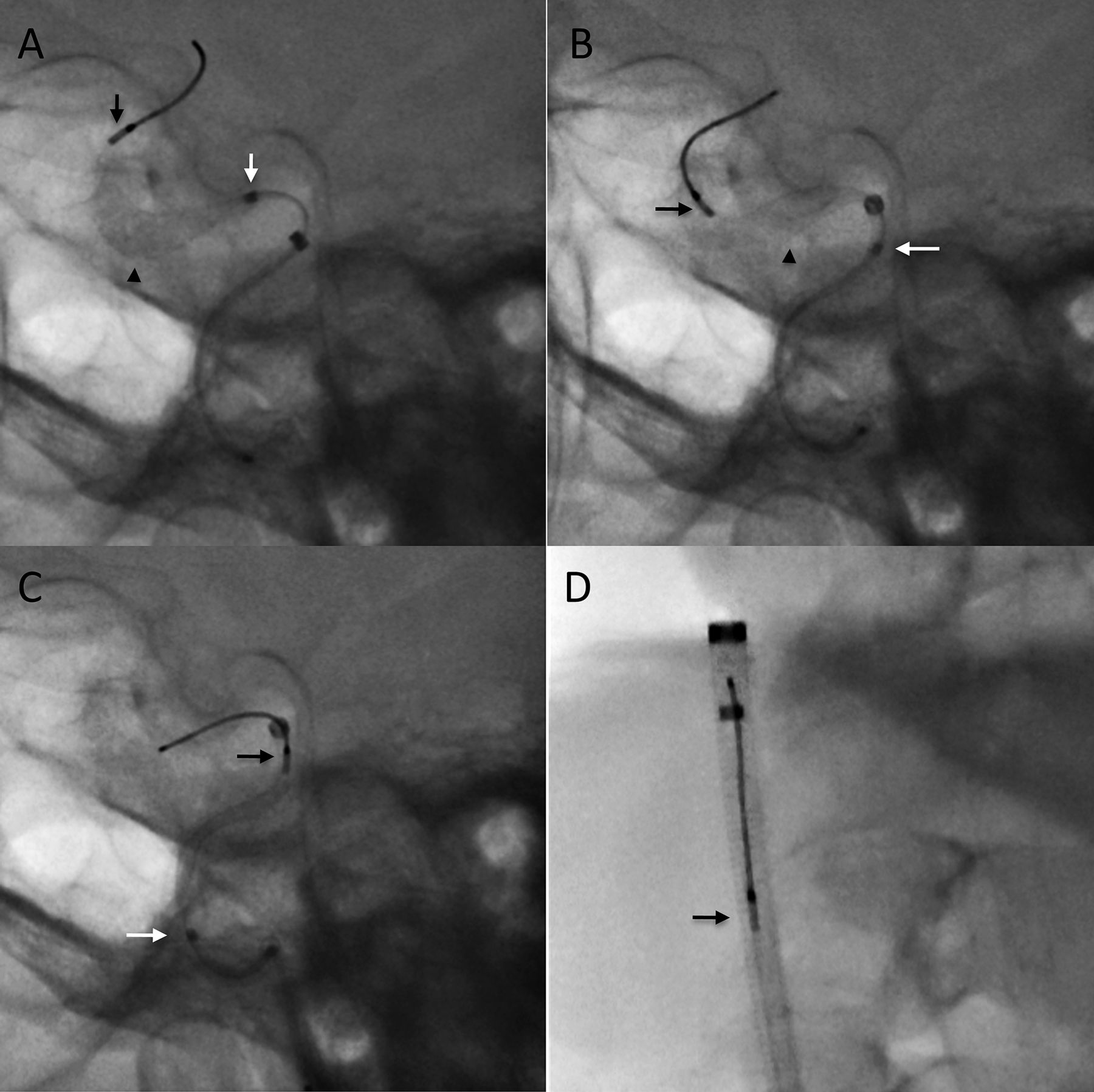
In case No 5 listed above, the PED was removed using a technique referred to here as ‘pseudo-corking’ (figure 2A, D). In this case, the PED pusher wire fractured at the point where it connects to the proximal bumper. This fracture caused complete disconnection of the distal wire segment, making removal of the partially deployed PED via classical corking impossible. In order to remove the PED, several steps were performed. First, the guide catheter was advanced over the Marksman until both of their tips were nearly aligned for maximal control of the Marksman. Second, the Marksman catheter was advanced forward so that it jammed into the proximal portion of the partially deployed PED (figure 2A). Third, the Marksman catheter was slowly withdrawn into the guide catheter (figure 2B, C). Of note, the PED can elongate considerably during this step. Finally, the guide catheter is withdrawn (figure 2D). In this case, the PED is held to the microcatheter by the friction forces between the inner lumen wall of the microcatheter and the undeployed PED and also between the microcatheter tip and the portion of the deployed PED captured during pseudo-corking. The extreme distal position of the guide catheter was key for removal of the device in this fashion because a ‘pseudo-corked’ PED is relatively unstable and prone to unintentional release.
{kind=link}
{kind=link}
Pseudo-corking and removal of a 4.5 mm × 20 mm pipeline embolization device (PED) from an internal carotid artery. (A) Fluoroscopy demonstrating the distal PED (arrowhead) deployed in the clinoidal/cavernous internal carotid artery. The black arrow represents the protective/capture coil and distal bumper and the white arrow represents the distal marker of the Marksman microcatheter. The PED pusher wire is fractured proximal to the proximal PED bumper. The 5 Fr ReFlex 0.058 inch guide catheter and subsequently the Marksman microcatheter were advanced to engage and jam the proximal portion of the deployed PED. (B, C) Relying on friction forces between the PED and the Marksman, the Marksman catheter was slowly withdrawn into the ReFlex guide catheter. (D) These devices were subsequently withdrawn into a 6 Fr Flexor Shuttle Select Guiding Sheath positioned in the proximal internal carotid artery.
Discussion
The introduction of flow diversion with the PED represents a paradigm shift in the approach to managing intracranial aneurysms. Although the PED is labeled a ‘device’, its handling and deployment is truly a combination of multiple novel ‘techniques’. A solid working knowledge of these techniques and the associated new vocabulary that describes them is critical for the modern neurointerventional surgeon using the PED.
The authors describe five cases of capture and retrieval of a partially deployed in situ PED using the corking and pseudo-corking techniques. In three of the cases, the device was removed because of failure of the PED to properly open. In one case the distal PED dislodged from the target vessel necessitating removal, and in an additional case a PED was removed because the distal PED deployed proximal to the aneurysm. In four of the cases, the corking technique was able to easily and safely facilitate removal of the involved PED. For the fifth case, however, the corking technique could not be used because the PED pusher wire fractured at the location of the proximal bumper. A pseudo-corking technique was therefore utilized. The corking technique has undoubtedly been used by other groups for salvage removal of a PED, both nationally and internationally, but this report represents the first such description in the literature. The pseudo-corking technique described in this report represents a novel technique that was developed to remove a partially deployed PED when it was impossible to cork the device secondary to a fractured pusher wire.
The corking technique works only for capture of a partially deployed PED because the protective/capture coil of the pusher wire needs to wedge the PED against the microcatheter. Likewise, the pseudo-corking technique can only be used for a partially deployed PED because once the PED is fully deployed and expanded, the device cannot be captured by advancing the microcatheter. Retrieval of a fully deployed intracranial stent using an adjunct device has been previously described but not for the PED. Chen and Goldstein-Smith reported two cases of Enterprise stent (Codman, Miami Lakes, Florida, USA) rescue using the Alligator retrieval device (ARD; Covidien, Mansfield, Massachusetts, USA).6 Vora et al reported retrieval of a Neuroform stent (Stryker, Kalamazoo, Michigan, USA) using the L5 Merci Retriever (Concentric Medical Inc).7 The retrieval of a fully deployed PED has not been reported but use of adjunct devices such as snares or the ARD would be reasonable options. Regardless of whether the PED is partially or fully deployed, removal of the device involves dragging the metal stent over vessel endothelium and there is a risk of vasospasm or vessel wall damage.
Special consideration should be given when using the corking technique in conjunction with a highly trackable guide catheter, such as a DAC or ReFlex catheter. These catheters are usually placed in distal positions such as the petrous or cavernous internal carotid artery. When the ‘corking’ technique is employed and the entire PED/microcatheter assembly is being extracted, the release of slack in the delivery microcatheter system can cause the trackable guide catheter to advance even further distal, threatening vasospasm, dissection or other damage to the internal carotid artery. Although a distal guide position is more desirable, the exact position should be scrutinized before introducing the forces necessary to withdraw an in situ PED. This is the case particularly if a significant portion of the PED is already deployed, thereby increasing the friction force of the ‘corking’ withdrawal.
Conclusion
Removal of a partially deployed PED may be necessary if technical or mechanical difficulties prevent the device from opening or if the distal device is dislodged from or malpositioned in the target vessel. The ‘corking’ technique is a simple and safe maneuver to capture and remove the PED in such a situation. The ‘pseudo-corking’ technique is also a feasible option if corking is not possible. It is important for interventionalists to be familiar with multiple options such as these for removal of a PED.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (MOV) - Manuscript file of format mov
- Download Supplementary Data (MOV) - Manuscript file of format mov
- Download Supplementary Data (MOV) - Manuscript file of format mov
- Download Supplementary Data (MOV) - Manuscript file of format mov
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the the Institutional Review Board of Johns Hopkins Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.