Article Text

Abstract
Crossing the neck of large complex intracranial aneurysms for the purposes of stent deployment can be challenging using standard over the wire techniques. We describe a novel yet simple technique for straightening out the loop formed within a large intracranial aneurysm, which is often required in order to cross the aneurysm neck into the distal branch. Both the microcatheter and microwire are initially introduced into the distal vasculature, followed by withdrawal of the microwire to a point parallel to the distal exiting branch. The microcatheter and microwire are then gently withdrawn and a series of maneuvers to gradually reduce the loop is performed, obviating the need for distal purchase in the form of a stent, balloon, or coil, which have previously been described to maintain distal purchase.
- Aneurysm
- Catheter
- guidewire
- Stent
- Technique
Statistics from Altmetric.com
Background
The options for the treatment of giant and large complex intracranial aneurysms have improved significantly since the addition of both stent-assisted coiling and flow diversion to the endovascular repertoire. These aneurysms are often large in size and have complex anatomical configurations of the proximal and distal branches entering and exiting the aneurysm. This can make crossing of the aneurysm neck for the purposes of stent deployment challenging using standard over the wire techniques. It is often necessary to form a loop within the aneurysm with the microwire and microcatheter in order to cross the aneurysm neck into the distal vasculature. A number of techniques have previously been described to then straighten the consequent loop within the aneurysm, with key goals being to avoid excess pressure on the aneurysm wall while maintaining distal purchase.1–3 We describe a novel yet simple technique called the ‘wire anchor loop traction’ (WALT) maneuver to achieve these goals.
Case presentation
A 67-year-old woman with a symptomatic unruptured giant right-sided paraophthalmic artery aneurysm presented for flow diversion stent treatment (figure 1, panel 1). The patient was loaded on aspirin and clopidogrel 1 week prior to the procedure.

{kind=link}
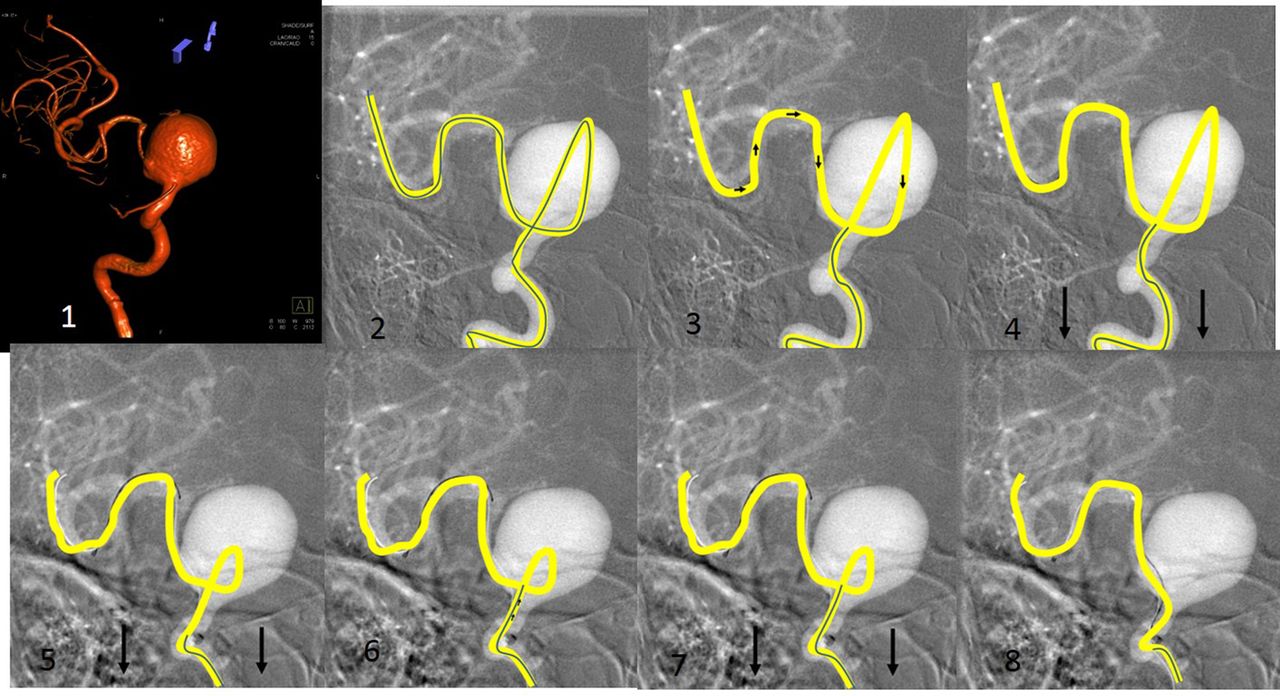
The wire anchor loop traction (WALT) maneuver. Panel 1: three-dimensional angiographic reconstruction of right-sided paraophthalmic aneurysm. Panels 2–8: roadmap depiction of WALT maneuver with the microcatheter illustrated by a solid yellow line and the microwire by a solid black line (see text for detailed description).
Technique
A 6 F Cook Shuttle guiding catheter (Cook, Bloomington, Indiana, USA) was introduced into the common carotid artery and a Navien 072 6 F guide catheter (Covidien, Mansfield, Massachusetts, USA) was positioned in the horizontal petrous carotid. A Marksman microcatheter (Covidien) over a 0.014 inch outer diameter Synchro-14 microwire (Stryker Neurovascular, Fremont, California, USA) was then introduced in a co-axial fashion. Initial attempts at cannulating the distal supraclinoid internal carotid artery using conventional microwire techniques were unsuccessful. The wire was advanced and a loop was formed within the aneurysm; the wire was then directed out of the distal internal carotid artery followed by the right-sided middle cerebral artery (MCA) M2 segment. The microcatheter was tracked over the microwire to follow the loop into the aneurysm and then out into the right MCA. Attempts at straightening the system and reducing the loop by gently pulling on the microcatheter failed.
The WALT maneuver was then performed in order to straighten out the looped microcatheter. As depicted in figure 1 panels 2–8, the following steps were taken:
The microwire and microcatheter are shown looped within the aneurysm with the distal end of the microcatheter and microwire in the M2 branch (panel 2).
The microwire was then withdrawn within the microcatheter to a point parallel with the distal exiting branch from the aneurysm. The position of the distal portion of the microcatheter was maintained throughout (panel 3).
Gentle traction was then placed on both the catheter and the microwire until the loop was made smaller (panels 4 and 5).
The microwire was advanced within the microcatheter to establish its previous relationship with being parallel to the exiting branch from the aneurysm (panel 6).
Gentle traction was repeated on both the microcatheter and the microwire, making the loop smaller (panel 7).
Steps 5–7 were repeated until the loop straightened (step 8).
Outcome and follow-up
The procedure continued uneventfully.
Discussion
Navigation of a microcatheter and microwire across the neck of large complex aneurysms is essential for stent placement and may require the formation of a loop within the aneurysm in order to cross the neck. Previously published techniques of straightening the loop generated by the microwire within the aneurysm share some mechanism of obtaining distal purchase to stabilize the catheter distally while pulling on the proximal catheter, either with a stent,2 balloon3 or free floating long coil.1 The WALT which we describe is simpler and more cost-effective—as well as possibly safer—obviating the need for navigating around the dome of the aneurysm with a stiffer balloon or stent.
We hypothesize the following explanation as to how the WALT maneuver works. Withdrawal of the microwire in the microcatheter approximately to a point created by a parallel line from the distal exiting branch allows two factors to work in synergy. First, the distal floppy microcatheter acts as a dragging and stabilizing mechanism, similar to the ‘sea anchor’ technique which utilizes a long coil for the same purpose. Second, the junction of the microcatheter and microwire result in a pivot along the microcatheter and acts as a guiding point for unlooping of the microcatheter.
We believe that the WALT offers a safe and cost-effective approach to navigating across challenging large and giant aneurysm necks.
Key messages
Navigation across large and giant aneurysms can be technically challenging.
A variety of techniques, including using stent assistance and coil deployment have been described.
The wire anchor loop technique (WALT) method is a cost effective and simple technique that we find useful in addressing this problem.
Footnotes
Republished with permission from BMJ Case Reports Published 23 January 2015; doi:10.1136/bcr-2014-011604
Contributors TRM conceived and designed the study; KE and RHS drafted the manuscript; TRM and FB critically reviewed and contributed to the manuscript.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.