Article Text

Abstract
Background Cerebral venous sinus thrombosis (CVST) is an uncommon form of stroke with a variable presentation, ranging from headaches, to coma and death. Although the American Stroke Association has developed guidelines for the treatment of CVST, data are sparse on the outcome after treatment with anticoagulation, thrombolysis, and thrombectomy.
Methods In this retrospective review, we describe the 5-year UC Davis experience with spontaneous CVST.
Results Forty-one patients (mean age 37.5±23.1, range 0–96 years; 29 female) were identified with CVST. The majority of cases involved the transverse sinus (75.6%), sigmoid sinus (58.5%), and superior sagittal sinus (29.3%). The most common form of treatment was anticoagulation or antiplatelet therapy (n=35), while six patients were managed by observation alone. The overall 1-year modified Rankin score (mRS) was 1.4±1.5. Male patients and patients with a poor admission mRS had a worse outcome. Outcome was unaffected by hypercoagulable state, number of dural sinuses involved, the presence of intracranial hemorrhage, or seizures. Two patients who underwent anticoagulation therapy also required endovascular thrombectomy; both patients had a 1-year mRS of ≤2. Two patients underwent direct open surgical canalization of the superior sagittal sinus with varying outcomes (mRS 2 vs mRS 6).
Conclusions In our series, the majority (92.9%) of patients with spontaneous dural sinus thrombosis had a favorable clinical outcome as defined by a mRS ≤2. Further prospective studies are needed to study the impact of anticoagulation on the clinical course of the disease.
- Thrombectomy
- Thrombolysis
Statistics from Altmetric.com
Introduction
Cerebral venous sinus thrombosis (CVST) is a relatively uncommon disease.1 ,2 It is most often related to neoplasms, infection, puerperium, pregnancy, systemic diseases, dehydration, oral contraceptives (OCPs), or coagulopathies; however, in 30% of cases, no underlying etiology can be identified.3–5 Occlusion of one or more dural sinuses, particularly the superior sagittal sinus, can result in significant cerebral edema, elevated intracranial pressure, hydrocephalus, hemorrhage, infarction, and death.6 Clinical presentation can vary from headaches to coma and death.3 Diagnosis is often suspected on routine CT and confirmed with MRI, CT venography, MR venography, or catheter-based angiography.
Mild cases are often treated with systemic anticoagulation alone, whereas significant neurological decline in the case of venous sinus thrombosis is often treated with endovascular therapy.7 However, as this is a relatively rare disease, only five cohort studies have analyzed the prognostic factors for the short-term and long-term outcome of CVST.8 Therefore, a study of the influence of clinical variables (eg, use of anticoagulation) on outcome is still needed. Here, we analyze our 5-year institutional experience with CVST and modifiers of clinical outcome.
Material and methods
Diagnosis of cerebral venous sinus thrombosis
In this study, we evaluated all patients with the diagnosis of CVST between July 2009 and June 2014 at the UC Davis Medical Center. Patients with a diagnosis of spontaneous CVST were identified by searching the UC Davis database for the following International Classification of Diseases-9 codes: 325, 437.6, and 671.5.
All patients with the ICD-9 code for CVST were reviewed. Only patients with confirmed spontaneous sinus thrombosis on CT venography, MR venography or conventional angiography were included in this study. The UC Davis institutional review board approved this retrospective review.
Exclusion criteria
Patients were excluded from this study if sinus thrombosis was not verified by imaging, if it was secondary to trauma, or occurred from a direct compression by a mass lesion (ie, tumor). Patients with cortical vein thrombosis were also excluded from this study.
Management of spontaneous CVST
Specific treatments and the decision when and if to perform follow-up imaging were at the discretion of the treating physician. Functional outcomes were obtained at 6 and 12 months using the modified Rankin Scale (mRS).
Statistics
A multivariate ordinal logistic regression model was used to estimate associations between patient characteristics as well as treatments and 1-year outcomes (mRS). Parametric data are presented as mean values±SE.
Results
Patient demographics
Between July 2009 and June 2014, 41 patients (mean age 37.5±23.1, range 0–96 years) were identified with spontaneous CVST. Similar to previously published results, more women than men were affected group (29 female, 12 male). The most common presenting symptom was headache (63.4%), followed by hemiparesis (19.5%), and seizures (14.6%, figure 1A). Of the 41 patients, only one had an associated pulmonary embolism. Seven patients (17.1%) were diagnosed with papilledema; however, only two patients developed persistent pseudotumor (4.9%) that required a permanent ventriculoperitoneal shunt.
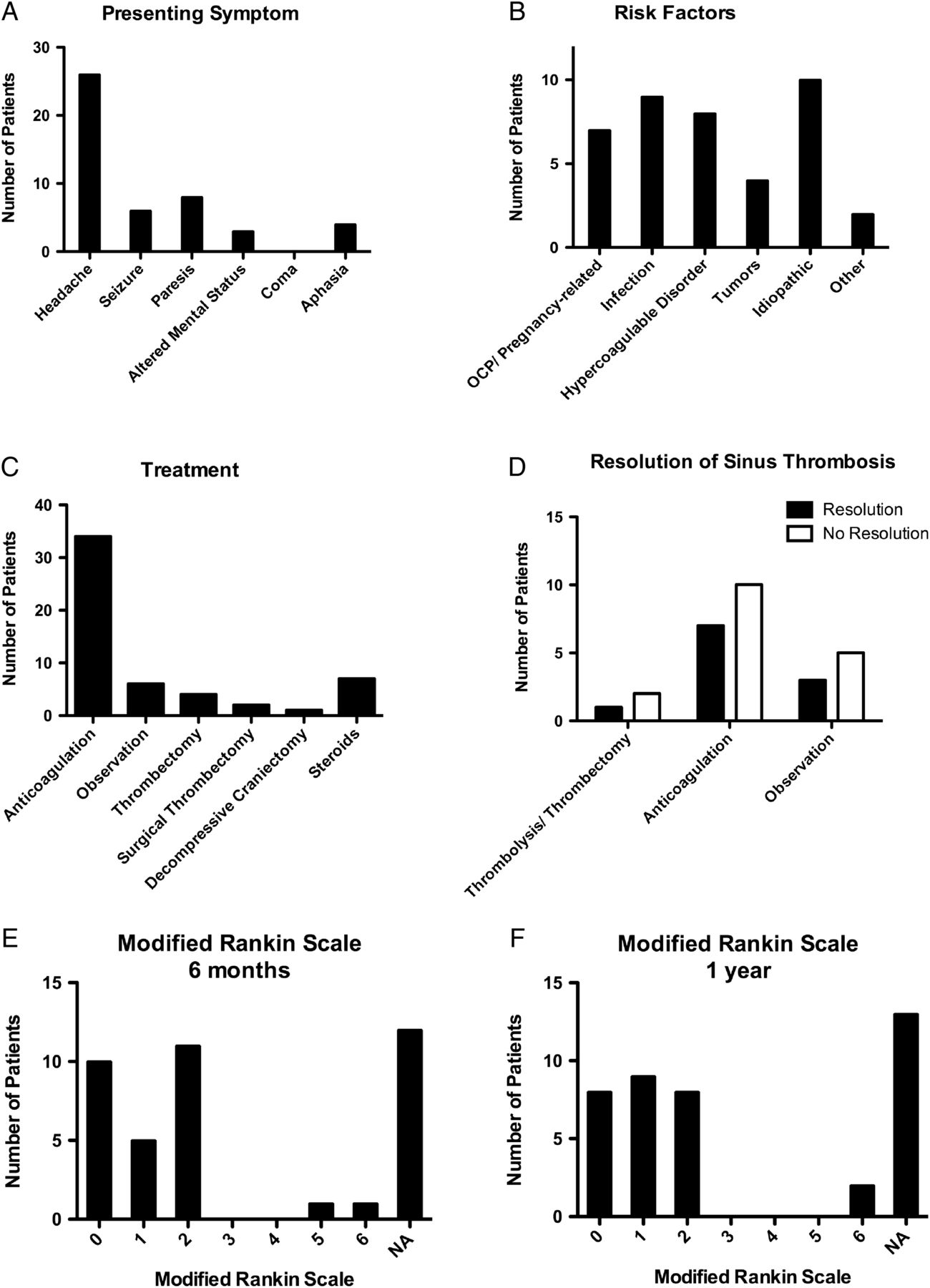
(A) The most common presenting symptoms were headache (63.4%), hemiparesis (19.5%), and seizures (14.6%). (B) A wide variety of suspected risk factors of spontaneous cerebral venous sinus thrombosis (CVST) are illustrated in this figure (oral contraceptives (OCPs)/pregnancy-related: 22.0%, infection: 17%, hypercoagulable disorder: 19.5%, tumors: 7.3%, idiopathic: 24.4%, and other: 12.2%). (C) Distribution of treatment modalities provided for CVST. (D) Observed outcomes (resolution vs no resolution) in 28 patients with CVST who received follow-up imaging after initial diagnosis and treatment (anticoagulation vs observation). (E) Modified Rankin Scores (mRS) at 6 months after CVST (mean mRS 1.3±1.4) and (F) 1 year after CVST (mean mRS 1.4±1.5). NA, not available as patients were lost to follow-up.
The most common risk factors for spontaneous CVST were OCPs or pregnancy-related etiology (22.0%), hypercoagulable state (19.5%), infection (17.1%), and systemic malignancy (9.8%, figure 1B). Ten patients (24.4%) had no known risk factors for CVST.
The majority of cases involved the transverse sinus (75.6%), followed by sigmoid sinus (58.5%), and the superior sagittal sinus (29.3%, figure 2). Only two cases involved the straight sinus (4.9%). Most cases had two or more sinuses affected (75.6%). There was no predominant laterality. The right hemisphere was involved in 20 cases (48.8%), the left hemisphere in 21 cases (51.2%), and 13 cases (31.7%) had a midline sinus involved.

Schematic diagram of cerebral venous sinus thrombosis locations and distribution.
Treatment and outcomes
The most common form of treatment was anticoagulation (34 patients, 82.9%; figures 1C and 3). Two of the patients undergoing anticoagulation also received antiplatelet therapy, and an additional patient received antiplatelet therapy alone. Antiplatelet therapy was chosen in these patients owing to concomitant cardiac disease. Six patients (14.6%) were merely observed. Eleven of the patients receiving anticoagulation had a lumbar puncture. Of note, three of these patients had normal opening pressures (<20 cm water). Two patients who underwent open surgical thrombectomy had a lumbar drain placed to monitor intrathecal pressures. Nineteen patients in the anticoagulation group underwent diagnostic cerebral angiography. Four of these patients also underwent thrombolysis. Two of these patients needed surgical thrombectomy, one of whom required a hemicraniectomy secondary to intracranial hypertension.

Retrospective summary of cerebral venous sinus thrombosis treatment.
Follow-up imaging was obtained in all patients with persistent symptoms after 30 days. In our cohort, 28/41 patients (68.3%) had follow-up imaging after the initial diagnosis (mean length of radiologic follow-up 11.0±10.2 months). Follow-up imaging was not obtained in the two patients who died. Without thrombolysis or thrombectomy, of those patients with follow-up imaging, 10 patients had image-confirmed spontaneous resolution of the sinus thrombosis (resolution at 9.1±5.7 months), while 15 patients continued to have occlusion (mean final imaging at 11.1±9.5 months, figure 1D). With either anticoagulation or antiplatelet therapy, 7/17 patients (41.2%) had complete resolution of their sinus thrombosis, while 10/17 patients (58.8%) had no resolution. Similarly, 3/8 patients (37.5%) who were managed by observation alone had a complete resolution of their sinus thrombosis, while 5/8 patients (62.5%) had no resolution. None of the 28 patients followed up for 1 year developed the clinical findings of a dural arteriovenous fistula.
In two patients, local thrombolysis was deemed necessary, as systemic heparin was insufficient. However, after interventional thrombolysis through femoral venous access, neither of the two patients had resolution of their sinus thrombosis (figure 4). Both of these patients had a 1 year mRS of ≤2. In each of these two cases mechanical thrombectomy was limited as the clot was too hard, and in one case there was immediate re-forming of the clot after the catheter was withdrawn. Two patients underwent direct open surgical canalization of the superior sagittal sinus and subsequent injections of tissue plasminogen activator and/or mechanical thrombectomy. In one patient, removal of the transfemoral clot failed, which required a direct surgical superior sinus thrombectomy.9 This patient had a mRS of 2 at 1 year. The second patient who required open surgical thrombectomy developed a blown pupil and elevated intracranial pressure after admission, resulting in an emergent hemicraniectomy and subsequent intraoperative superior sagittal sinus catheterization. Ultimately, this patient's care was withdrawn.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) A patient in the fourth decade of life with a history of lupus and hypothyroidism presented with a 1-month history of right-sided headache and 1-day history of new-onset convulsive seizures. Initial head CT demonstrated a 2.5×1.5 cm acute intraparenchymal right occipital lobe hematoma, probably secondary to acute venous thrombosis of the straight sinus. (B) MR venography (MRV) demonstrated thrombosis of the distal portion of the superior sagittal sinus, confluence of sinuses, bilateral transverse sinuses, straight sinus, and a portion of the vein of Galen. The patient underwent an unsuccessful attempt to catheterize intracranial dural sinuses in the interventional radiology suite with persistent extensive occlusive disease in the bilateral jugular veins and jugular bulbs as well as the sigmoid and transverse sinuses. The patient was then transitioned to chronic anticoagulation. (C) Three years later, MRV continued to demonstrate absent flow-related enhancement of the posterior aspect of the superior sagittal sinus. The bilateral transverse and sigmoid sinuses appeared to reconstitute through collaterals. At 1 year after intervention, the modified Rankin Score was 1. (D) A second patient in the fifth decade of life with a history of hypertension, asthma and receiving oral contraceptives presented with a 1-day history of worsening headache, confusion, and aphasia. Initial CT of the head demonstrated a large frontotemporal intraparenchymal hematoma (7.7×4.1×4.4 cm). (E) Initial MRV demonstrated dominant left transverse and sigmoid sinuses with significant thrombotic occlusion extending into the proximal jugular vein. Additionally, there was no flow related enhancement within the inferior anastomotic vein of Labbe, suggestive of occlusion. (F) The patient had a partial mechanical thrombectomy of the left jugular bulb without restoration of flow in the left transverse and sigmoid sinus. There was reconstitution of the left inferior petrosal sinus flow through collaterals after thrombectomy. Additionally, the right transverse and sigmoid sinus were thought to be large enough to drain the superior sagittal sinus. Treatment was started with anticoagulation. At 1 month, MRV demonstrated a stable intraparenchymal hematoma and increased flow-related enhancement in the left transverse and sigmoid sinus compatible with partial recanalization. At 1 year after intervention, the modified Rankin Score was 2. (G and H) A patient in the fourth decade of life presented with 3–4 day history of persistent headaches and emesis. Initial MRI of the brain demonstrated a venous infarct and hemorrhage within the right temporal lobe as well as near complete occlusion of the sagittal sinus and complete occlusion of the right transverse sinus, vein of Labbe, torcula and jugular vein. The patient rapidly decompensated after admission and developed a right fixed and dilated pupil. Repeat CT of the head demonstrated worsening edema around the temporal hematoma and increased midline shift. The patient was then taken emergently to the operating room for a right hemicraniectomy, superior sagittal sinus thrombectomy, and thrombolysis. Postoperatively, the ventricular drain lacked an adequate waveform and did not drain. A lumbar drain was then placed with an opening pressure that eventually rose to >55 mm Hg. (I) A subsequent left external ventricular drain was placed. Despite maximal sedation and paralytics, the intracranial pressure remained elevated. Care was subsequently withdrawn on hospital day 4, at the family's request.
Overall, 28 patients (68.3%) had a mRS of 1.3±1.4 (range 0–6) at 6 months and 25 patients (61.0%) a mRS of 1.4±1.5 (range 0–6; figure 1E, F) at 1 year. In one patient, care was withdrawn owing to a poor prognosis, while another patient with a history of cancer died at home without a definitive cause. Based upon a multivariate ordinal logistic regression analysis, women had a more favorable outcome at 1 year than men (mRS 1.00±0.18 vs 2.67±1.09, p<0.05). Additionally, patients with a worse admission mRS had a predictably worse 1-year score (p<0.05). Although not statistically significant, patients who presented with infection (infection: mRS 3.00±1.27 vs no infection 1.00±0.16, p=0.063), older age (p=0.066), or a deep venous sinus thrombosis (p=0.105) were more likely to have a worse outcome. There was no significant difference in outcome regardless of the presence of intracranial hemorrhage (p=0.96), hypercoagulable state (p=0.84), number of sinuses involved (0.54), seizures (0.62), or systemic malignancy (p=0.55). Our study had no patients who were in a coma upon initial admission. While the sample size was small, there was no significant difference in outcome between patients who received anticoagulation and those who did not (anticoagulation mRS 1.28±1.41 vs no anticoagulation mRS 1.56±1.88, p=0.09). Of note, 16 cases were lost to follow-up at 1 year. Two deaths occurred within 1 year of diagnosis.
Discussion
CVST is a relatively rare disease. The overall incidence of adult CVST is 1.32 per 100 000 person-years.10 Similar to previously reported studies, our data suggest a peak incidence in adults during their third decade.11 Our data also support published reports of an increased prevalence in women (3:1),11 ,12 even when excluding cases due to pregnancy and oral contraception. Some evidence suggests that women were younger than men, but in our study, even excluding newborns,11 men were generally younger than the women affected (median age: 19 years vs 41 years, respectively).
Several case reports have described the development of a dural arteriovenous fistula after sinus or cortical vein thrombosis.13 ,14 However, in our study, none of the 28 patients who were followed up for at least 6 months developed the symptoms of a dural arteriovenous fistula as a result of their dural sinus thrombosis. Additionally, there have been reports that sinus thrombosis preferentially affects the left transverse and sigmoid sinus, as it is more often hypoplastic;15 however, our study did not demonstrate a left-sided predominance.
Treatment options remain controversial, but the American Heart Association and American Stroke Association have suggested general guidelines for the treatment of CVST.8 ,16 Specifically, patients with sinus thrombosis should be tested for prothrombotic conditions (including protein C, protein S, or antithrombin deficiency), antiphospholipid antibody syndrome, prothrombin G20210A mutation, and factor V Leiden. Anticoagulation via IV heparin or subcutaneous low molecular weight heparin can be started as long as there are no major contraindications. If the patient exhibits neurological improvement or remains stable, the patient may continue to receive oral anticoagulation (target international normalized ratio of 2.0–3.0) for 3–12 months. Although there is a paucity of data on the overall benefit of anticoagulation with respect to death and disability, studies suggest that anticoagulation treatment is safe.11 ,17 However, multiple studies have led to inconclusive results for the clinical outcome with or without anticoagulation.15 ,18 There was a trend towards treatment with anticoagulation and improved outcomes in our cohort, but this was not statistically significant. Further prospective studies are needed, as physicians might have been biased and treated severe clinical presentations more aggressively with anticoagulation.
If a patient shows neurological deterioration or remains in a coma despite medical treatment, the next-line treatment is endovascular therapy (with or without mechanical thrombolysis). In urgent cases, superselective infusion of thrombolytic agents into the occluded sinus has been shown to be effective19–21 and may be considered in patients who are deteriorating.22–24 Endovascular mechanical thrombectomy may be effective in severe cases with tenacious thrombus or extensive clot burden.25–27 However, in our series, mechanical thrombectomy or thrombolysis through femoral venous access failed for both patients. Interestingly, both patients had good clinical outcomes. The indication and effectiveness of neurointerventional management of dural venous sinus thrombosis remains to be elucidated.
CVST is typically treated medically, but there may be a role for neurosurgical intervention. When endovascular mechanical thrombectomy is unsuccessful, surgical thrombectomy/thrombolysis via direct access to the superior sagittal sinus may also be considered as an adjunctive therapy.9 ,28 In one of our patients, transfemoral clot removal was unsuccessful, necessitating a direct burr hole approach. In the two patients treated surgically, one patient had a favorable outcome with this approach, and one patient continued to decline until care was withdrawn. If there is mass effect or intracranial hemorrhage, a decompressive craniectomy may also be performed. In our series, one patient underwent a decompressive craniotomy without improvement.
The International Study on Cerebral Vein and Dural Sinus Thrombosis found several predictors of poor outcome (mRS >3), including older age (>37 years), male sex, coma, seizure, deep CVST, brain hemorrhage, and concomitant diseases such as hematological pathologies, systemic malignancy, and central nervous system infection.29 Similarly, we found that women had more favorable outcomes than men. Furthermore, a poor admission mRS portended a worse outcome. Patients who had concomitant infections, deep CVST or older age were statistically close to a worse outcome. However, there was no significant difference in patients with seizures, intracranial hemorrhage, deep CVST, hypercoagulable disorders, or systemic malignancy. In this study, no patients were identified with coma on initial admission.
Interestingly, in a large meta-analysis by Feher et al,18 the presence or absence of anticoagulation treatment was not a predictor of poor outcome, which is consistent with our results. Additionally, clinical outcome was significantly more favorable in women with gender-specific risk factors than in men.15 In our patient population, women who had CVST with either concomitant OCP use or pregnancy had a favorable outcome (mRS 1.4±0.5). One patient (2.4%) had an additional thrombotic event (pulmonary embolism), similar to that of previously published reports (5.4%).18 While we did not identify any recurrence of CVST, the reported CVST recurrence rate is approximately 3.7%. In this study, two deaths were reported (4.9%), consistent with previously published mortality rates of 6.5–15% of cases.18 ,29
Conclusion
In this series, the majority (92.9%) of patients with spontaneous dural sinus thrombosis had a favorable clinical outcome as defined by a mRS ≤2. We identified female gender and favorable admission examination as predictors of a favorable outcome. While not statistically significant, concomitant infection, older age, and deep CVST were suggestive as predictors of an unfavorable outcome. Anticoagulation did not statistically influence outcome, but results may be biased owing to the retrospective nature of our study. The indication and efficacy of neurointerventional management through femoral venous access remains to be elucidated since three out of three patients in our series could not be recanalized with this approach, but all of these patients had good clinical outcomes. Interestingly, one of these patients required open surgical thrombectomy. Future prospective investigation is still needed to delineate the indications and effectiveness of various treatment modalities.
References
Footnotes
Contributors All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafted the work or revised it critically for important intellectual content; and gave final approval of the version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval UC Davis institutional review board approval: 653859-1.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All collected data and analysis (excluding any patient identifiers) will be available for review.