Article Text

Abstract
Background Elevated mean platelet volume (MPV), indicating higher platelet activity, could be a predictor of prognosis in patients with acute ischemic stroke receiving medical therapy.
Objective To investigate the relationship between MPV and functional outcome in patients with acute anterior circulation stroke 3 months after undergoing mechanical thrombectomy (MT).
Methods A total of 153 consecutive patients with acute stroke following MT, in two separate stroke centers, were enrolled between May 2013 and March 2016. MPV was measured on admission. Subjects were divided into two groups according to average MPV level. Univariate and multivariate analyses were performed. MPV was also incorporated into the Houston IA Therapy (HIAT) score, which was developed as a scoring system to predict poor prognosis, and the prediction capability was compared with the HIAT score alone.
Results The average MPV was 10.4 fL. Patients with high MPV had a significantly lower rate of functional independence (28.9% vs 57.1%, p=0.000). After multivariable analysis, elevated MPV remained an independent predictor of unfavorable outcome (OR=3.93, 95% CI 1.73 to 8.94, p=0.001). When the MPV cut-off value was set at 10.4 fL using the receiver operating characteristic (ROC) analysis, MPV ≥10.4 fL predicted unfavorable outcome with 62.1% sensitivity and 66.7% specificity, respectively. Addition of MPV to the HIAT score did not improve predictive power compared with the HIAT score system alone by a comparison of the areas under the two ROC curves (0.70 vs 0.62, p=0.174).
Conclusions Elevated MPV is an independent predictor of poor outcome in patients with acute anterior circulation stroke undergoing MT at 3 months.
- Intervention
- Atherosclerosis
Statistics from Altmetric.com
Introduction
Enhancement of platelet activation is a crucial step in initiating a cascade of processes that may contribute to atherosclerosis, and also involved in the pathological process of ischemic stroke.1 ,2 Mean platelet volume (MPV), which is considered as an indicator of platelet function and activation, because larger platelets contain more dense granules and produce more prothrombotic factors than smaller ones,3 is usually obtained from routine blood tests in patients with acute stroke on admission. There is an inverse correlation between MPV and platelet count under physiological and some pathological conditions so that the circulating mass of platelets remains constant.4 ,5 Some studies have demonstrated that a higher MPV is an independent predictor of recurrence of stroke and cardiovascular events.6 ,7 Moreover, an elevated MPV value is related to a worse clinical outcome from acute ischemic stroke and myocardial infarction, even if patients with acute myocardial infarction are treated with percutaneous coronary intervention.8–10
In recent years, several prospective randomized studies have consistently shown that mechanical thrombectomy (MT) is better than IV thrombolysis alone in patients with large vessel occlusion in anterior circulation.11–15 MT has been recommended by the 2015 American Heart Association/American Stroke Association guideline for patients with proximal artery occlusion in anterior circulation owing to a higher rate of recanalization and better functional outcome.16 However, 29–67.4% of the patients still had an unfavorable prognosis despite receiving MT.11–15 A growing number of risk factors for poor clinical outcome have been identified, including older age, elevated baseline glucose, more severe neurological deficit, larger core infarction, and increased blood leukocytes.17–22
To our knowledge, the predictive value of MPV for prognosis in patients with acute occlusion of anterior circulation following MT has not been reported. The primary purpose of this study was to investigate the association of baseline MPV value with clinical outcome after MT. Furthermore, MPV was incorporated into the Houston IA Therapy (HIAT) score,23 which was developed as a simple tool to predict poor outcome and to determine whether the prediction capability was enhanced compared with the HIAT score alone.
Methods
Between May 2013 and March 2016, data of all consecutive patients with acute stroke receiving MT were prospectively collected and retrospectively analyzed at two stroke centers (Jinling Hospital, Nanjing Medical University and Zhongshan Hospital Xiamen University). Detailed information was recorded for all patients, including demographic characteristics, vascular risk factors, laboratory and imaging data, procedural details, and clinical functional outcome. Inclusion criteria for this study were age ≥18 years; a baseline National Institutes of Health Stroke Scale (NIHSS) score ≥6; large artery occlusion in the anterior circulation established by CT angiography, MR angiography or DSA; treatment started within 6 hours from the time of symptom onset or last known healthy; a modified Rankin scale (mRS) score before stroke ≤1; and hypodensity on cranial CT less than one-third of the middle cerebral artery territory. Exclusion criteria included tumor, hematologic disease, and autoimmune disease. Informed consent was obtained in all cases. The ethical committees of both hospitals approved the study.
Venous blood samples were drawn into standardized tubes containing an anticoagulant (EDTA) at admission and stored at room temperature. The value of MPV was determined using an autoanalyzer (Sysmex XE-2100 or XT-2000i, Kobe, japan) within 1 hour after sample collection.
Neurological deficits were evaluated by the NIHSS score at baseline and 24 hours after MT. CT or MRI was performed at 24 hours after intervention or whenever neurological deterioration occurred. Current smoking was defined as smoking at least 1 cigarette/day. Hemorrhagic transformations were classified as hemorrhagic infarction (type 1 and type 2) or parenchymal hematoma (type 1 and type 2) based on European Cooperative Acute Stroke Study-II criteria.24 Symptomatic intracerebral hemorrhage was defined as hemorrhage transformation within 36 hours after MT that was associated with a worsening neurologic deficit shown by an NIHSS score of ≥4 points. Stroke subtype was classified according to the Trial of Org 10 172 in Acute Stroke Treatment criteria.25 Recanalization results were assessed using the Modified Treatment in Cerebral Infarction (mTICI) Scale.26 A post-treatment mTICI score of 2b or 3 was considered as successful recanalization. Total time of operation was defined as time from groin puncture to mTICI 2b or 3 or completion of the procedure. Follow-up data were obtained by outpatient or telephone interviews. Clinical outcome was dichotomized into favorable functional outcome (mRS 0–2) or unfavorable functional outcome (mRS 3–6) at 3 months.
All MT procedures were performed using the groin puncture under local anesthesia. An 8 F or 6 F guiding catheter was placed in the internal carotid or common carotid artery through a short 8 F sheath. The microcatheter (Rebar-27/18, ev3) containing a microwire (Silverspeed-14, ev3) was navigated distal to the site of occlusion. Then, the stent retriever (Solitaire AB, ev3) was deployed and placed in the distal thrombus borders. After a delay of about 5 min, the microcatheter and the stent retriever were recovered under constant manual aspiration into the guiding catheter. This sequence was repeated until successful recanalization was established or a maximum of four attempts was reached.
The HIAT score was a simple scoring system to predict poor outcome for patients with acute ischemic stroke undergoing IA therapy using age, NIHSS score, and admission glucose level. Each variable scored 1 point as follows: age >75 years; NIHSS score >18; admission glucose >150 mg/dL.23 The HIAT score ranged from 0 to 3. We added the MPV value to the HIAT score and renamed it as the HIAT–MPV score; MPV was averagely dichotomized in our cohort. One extra point was assigned if MPV was higher than the average level. Thus, the HIAT–MPV score ranged from 0 to 4.
Statistical analysis
Participants were stratified into two groups according to the mean MPV level measured on admission. Continuous variables were presented as mean (SD) or median (IQR). Differences in continuous variables between groups were compared by Student t-test or Mann–Whitney test. Categorical variables were expressed as proportions and analyzed with the χ2 test or Fisher exact test. Associations between functional outcome and MPV and clinical parameters were first tested by univariate analysis. All possible variables with p<0.1 in univariate analysis were then entered into a forward logistic regression model. A receiver operating characteristic (ROC) curve was used to determine the sensitivity and specificity for the MPV at the cut-off level to predict clinical outcome. We compared the HIAT–MPV score with the HIAT score by area under the ROC curve (AUC). A p value of <0.05 was considered statistically significant and all statistical analyses were performed with SPSS V.16.
Results
A total of 156 patients who received MT fulfilled the inclusion criteria during the study period. Two patients were excluded because of lung cancer and one owing to systemic lupus erythematosus. As a result, 153 subjects were enrolled in the study. The mean level of MPV was 10.4 fL and mean age was 61.7±11.9 years. There were 105 (68.6%) men and 48 (31.4%) women. The patients were stratified into two groups according to the mean MPV value <10.4 fL (n=77) and ≥10.4 fL (n=76). Baseline clinical characteristics and clinical outcome according to MPV are presented in table 1. Patients with high MPV values were found to have a significantly lower proportion of current smoking (p=0.003), lower platelet count (p=0.005), and lower lymphocyte count (p=0.019) than those with low MPV, but a higher MPV/platelet count ratio (p=0.000).
Baseline characteristics and clinical outcome according to MPV
Successful recanalization was achieved in 80 (52.3%) patients, and 66 (43.1%) patients had good outcome (mRS 0–2). The univariate analysis suggested that elevated MPV was associated with a lower proportion of successful recanalization (43.4% vs 61.0%, p=0.029), but there was no statistical difference after controlling for confounders (OR=0.56, 95% CI 0.27 to 1.19, p=0.134). Patients with high MPV had significantly lower chance of functional independence (28.9% vs 57.1%, p=0.000). As shown in table 1.
The univariate analysis showed that age (p=0.000), MPV ≥10.4 fL (p=0.000), baseline NHISS scores (p=0.000), coronary artery disease (p=0.036), baseline systolic blood pressure (p=0.012), cardioembolism (p=0.018), platelet count (p=0.010), symptomatic intracerebral hemorrhage (p=0.024), and higher MPV/platelet count ratio (p=0.006) were significantly related to poor functional outcome in the cohort. On the contrary, successful recanalization was an indicator of good outcome (p=0.000; see online supplementary table S1). After multivariable regression analysis, there remained an independent relationship between higher MPV value and unfavorable outcome (OR=3.93, 95% CI 1.73 to 8.94, p=0.001). Figure 1 shows the distribution of mRS in the two groups. Moreover, older age (OR=1.05, 95% CI 1.01 to 1.09, p=0.012) and increased baseline NIHSS scores (OR=1.19, 95% CI 1.09 to 1.31, p=0.000) were also independent risk factors of poor outcome. Successful recanalization was inversely correlated with unfavorable clinical outcome (OR=0.21, 95% CI 0.09 to 0.48, p=0.000). The results are shown in table 2.
Risk factors for poor outcome using multiple logistic regression

Modified Rankin Scale (mRS) at 3 months among mean platelet volume (MPV) ≥10.4 fL and MPV <10.4 fL.
supplementary table
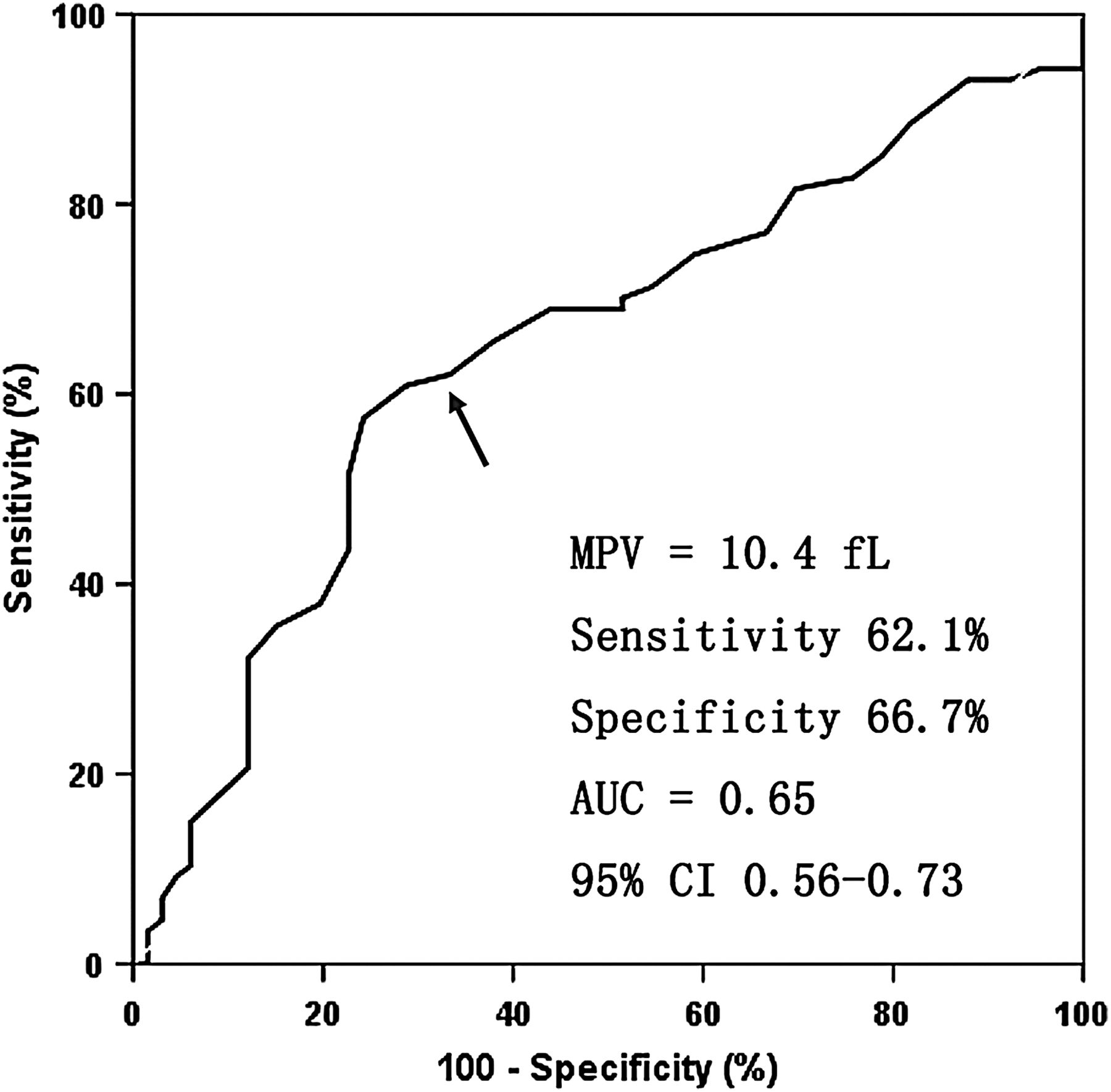
ROC curve analysis was employed to evaluate the ability of MPV level to predict poor clinical outcome. When the MPV cut-off value was set at 10.4 fL by using the ROC analysis, an MPV ≥10.4 fL had a sensitivity of 62.1% (95% CI 51.0% to 72.1%) and specificity of 66.7% (95% CI 53.9% to 77.5%). The area under the ROC curve with MPV used to detect worse outcome was 0.65 (95% CI 0.56 to 0.73) (figure 2).

{kind=link}
{kind=link}
The receiver operating characteristic (ROC) curve analysis of admission mean platelet volume (MPV) for predicting poor outcome. The area under the ROC curve (AUC)=0.65 (95% CI 0.56 to 0.73).
In the present cohort, the AUC for the HIAT–MPV score was 0.70 compared with an AUC of 0.62 for the HIAT score. There was no difference between the HIAT score and HIAT–MPV score in predicting poor outcome (Z=1.36, p=0.174).
Discussion
In this study, we demonstrated an independent association between elevated MPV value at admission and worse clinical outcome in patients with acute anterior circulation stroke and occlusion of a large vessel treated with MT. MPV ≥10.4 fL has a nearly fourfold risk of a worse clinical outcome at 3 months when we controlled for confounding factors. There is mounting evidence that a higher baseline level of MPV is a strong predictor of subsequent death or myocardial infarction in patients with coronary artery disease undergoing percutaneous coronary intervention.9 ,10 ,27–29 However, to the best of our knowledge, this study is the first to establish an association between MPV and the prognosis in patients with acute ischemic stroke following MT.
The correlation of an increased MPV level with worse clinical outcome after MT may be explained as follows. First, an elevated MPV level has been considered to be a marker of greater platelet size and activity. Larger platelets contain a higher platelet granule content, produce more thromboxane B2, express a higher level of P-selectin, fibrinogen and glycoprotein IIb/IIIa receptors, and secrete larger amounts of serotonin and β-thromboglobulin.30–33 Therefore, patients with a higher MPV level may have enhanced thrombogenic potential. Second, an increased MPV value might reflect an increase in reticulated platelets or immature platelets, which is an indicator of turnover. High platelet turnover has been reported to be correlated with platelet aggregation and poor response to antiplatelet therapy.34 ,35 Third, acute ischemic stroke results in the activation of platelets, upregulation of inflammatory factors, and infiltration of neutrophils at the site of ischemia.36 Platelet–neutrophil–endothelial cell interactions lead to thromboinflammatory injury that aggravates ischemic cerebral damage by microvasculature occlusion.36 ,37 Thromboinflammatory injury may be further aggravated in patients with higher MPV because larger platelets are more reactive than smaller ones.
In our study, we found that an elevated MPV level was an independent predictor of unfavorable outcome. Nevertheless, the relationship between elevated MPV and successful recanalization was significant only by univariate analysis but not in the multivariate analysis. There may be two possible explanations. First, the trend toward a lower rate of successful recanalization in patients with higher MPV group, although not statistically significant, might have been clinically relevant. Second, we speculate that endothelial cell damage following MT may be more likely to turn into re-thrombosis in patients with a higher MPV because of increased thrombogenic potential and antiplatelet agent resistance. If our results and hypothesis could be validated by further research, patients with elevated MPV after intervention could benefit from active treatment with re-thrombosis.
In addition, our study showed that older age and higher baseline NIHSS score were significantly correlated with poor clinical outcome in postintervention patients. Our findings are in agreement with the results in several studies of endovascular treatment with thrombolysis or MT.17 ,21 ,38 Older age is frequently related to poor outcome after endovascular treatment, probably owing to several factors including pre-stroke cognitive or physical impairments, reduced neuronal plasticity, a higher rate of postoperative complications and comorbidities.18 ,21 Our analysis also showed that successful revascularization was an independent predictor of good outcome, being consistent with previous studies.21 ,38 This study demonstrated a lower proportion of current smoking in patients with a higher MPV by univariate analysis. This finding is not totally consistent with other studies.9 ,27 ,39 We assume that it may be associated with smoking cessation of some patients when they identify coronary artery disease or traditional vascular risk factors.
Unfortunately, the results of our study demonstrated that the addition of the MPV value to the HIAT score did not improve predictive power as compared with the HIAT score alone, as showing by comparing the different AUCs. Addition of MPV to a scoring system based on β coefficients is worthy of further study with a larger sample.
This study has some limitations. First, it has the inherent limitations of an observational study and selection bias. Second, our sample population was relatively small, therefore, further studies with larger numbers of patients are needed. Third, we did not analyze the effect of drugs, such as antiplatelet or lipid-lowering drugs, on the MPV value before a stroke. Fourth, our study protocol did not take into account C-reactive protein and the left ventricular ejection fraction.
Taken together, this study is the first to demonstrate that elevated MPV is an independent predictor of worse outcome in patients with acute anterior stroke following MT. As an economic and easily measured hematological marker, baseline MPV may be a useful indicator for risk stratification of patients with acute anterior circulation stroke treated with MT.
References
Footnotes
FP and WZ contributed equally and are co-first authors.
Contributors FP: study design, acquired and analyzed the data, and manuscript drafting. WZ, FL: study design. JW: data collection and statistical analysis. ZL, XC: data collection. LX: revised the draft paper. WS: study design and critical revision of manuscript. XL: study design and revision of draft paper.
Funding This work was supported by the National Natural Science Foundation of China. Grant numbers (81501193 and 81530038).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics committees of the Jinling Hospital, Nanjing Medical University and Zhongshan Hospital Xiamen University.
Provenance and peer review Not commissioned; externally peer reviewed.