Article Text

Abstract
Background More challenging animal models are needed to elucidate the efficacy of flow diverter (FD) designs and the mechanisms behind observed complications. The purpose of this study is to demonstrate the feasibility of implanting a FD in a sidewall aneurysm rat model.
Methods An end-to-side anastomosis was created in the abdominal aorta of 36 rats using a decellularized donor pouch. A FD was subsequently implanted.
Results After up to 3 months of follow-up, we observed that rats displayed normal growth and behavior. Mortality within the groups was low (2 rats, 5.6%). All aneurysms thrombosed after FD implantation and showed progressive soft tissue replacement of the thrombus during follow-up. The abdominal aortas remained patent.
Conclusions This model can be used to test the effects of FDs in future studies.
- Flow Diverter
- Aneurysm
- Technique
- Artery
Statistics from Altmetric.com
Introduction
Animal models offer the opportunity to assess the vascular response and histological characterization of aneurysm healing and can be used to study the efficacy and safety of flow diverters (FDs) in an in vivo situation. Rabbit1–3 and dog4–6 models have been used in endovascular stent testing since the mid-1990s and are currently the only animal models available to test FDs.7 Despite the valuable information that has been collected from these animal models, additional and more challenging animal models are needed to demonstrate the efficacy of various FD designs and the mechanisms behind complications seen clinically.7
Recently, a possible candidate for a new and challenging model has been introduced by Marbacher et al.8 In this model a thoracic aorta segment from a donor rat is decellularized and implanted in the abdominal aorta of a recipient rat. This model is exceptional among the available in vivo aneurysm models in that aneurysm growth and even rupture have been documented.9 Expansion of the rat sidewall aneurysm model for experiments with endovascular devices, such as FDs, has been suggested by Marbacher et al,8 but has not been demonstrated up to this point. The goal of this study is to investigate the feasibility of expanding the sidewall aneurysm rat model as a tool for testing FDs.
Materials and methods
Animals
All animal experiments were approved by the institutional animal care and use committee. We used 72 6–8-week-old Wistar WU rats (Charles River, Den Bosch, The Netherlands) for this experiment. A thoracic aorta segment was harvested from 36 rats and was subsequently decellularized by the method previously described.8 The decellularized aortic segment was used to create a microsurgical aneurysm in the abdominal aorta of 36 recipient rats. All 36 rats subsequently received a FD and were sacrificed after 1 week (n=12), 1 month (n=12), or 3 months (n=12).
Animals were housed in an animal room at 22±1°C with a 12-hour light/dark cycle. Animals had free access to a pellet diet and sterilized water and received humane care in conformity with institutional guidelines.
Graft harvest and decellularization
A thoracic aorta section between the first intercostal artery and the left subclavian artery was harvested according to the method described by Marbacher et al8 (figure 1). After harvesting, the tissue was immediately stored in an Eppendorf tube filled with phosphate buffered saline (PBS) and stored on ice until decellularization overnight.
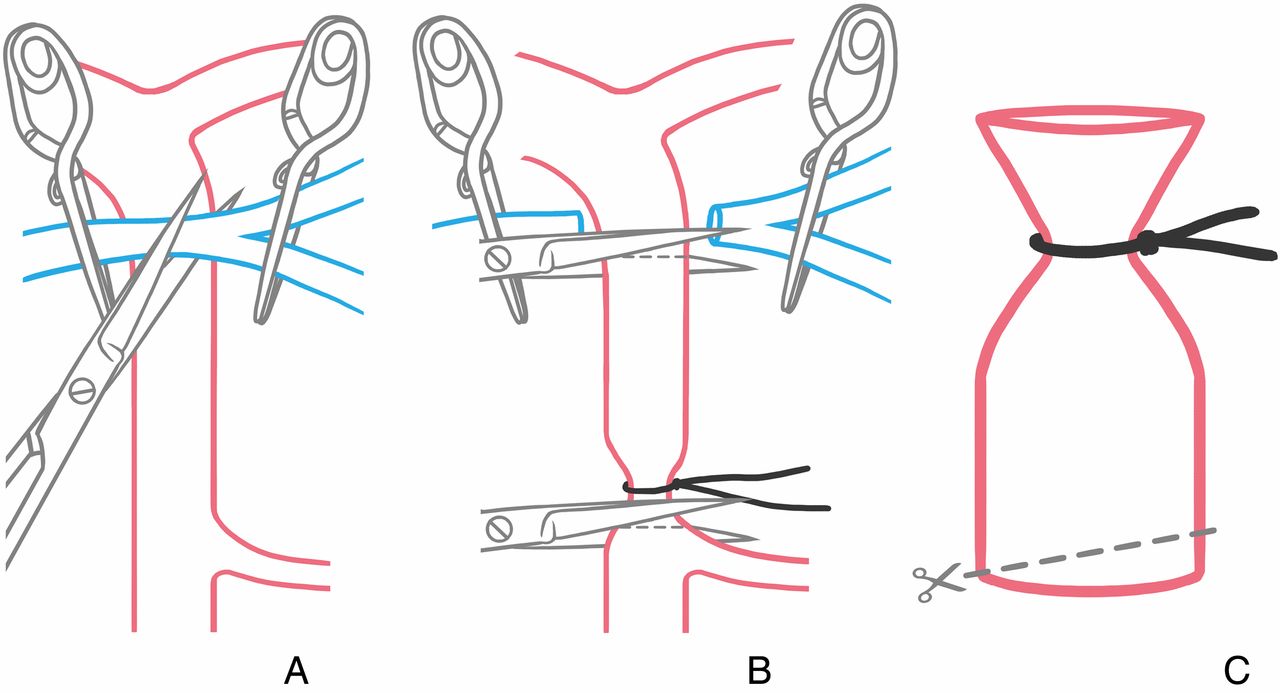
Clamping and cutting the prominent veins (A) to gain access to the thoracic aorta and harvest the section between the first intercostal artery and the left subclavian artery (B) resulting in an aortic donor pouch (C).
Decellularization of the aneurysm wall was achieved by incubation for 10 hours at 37°C in a 0.1% sodium dodecyl sulfate (SDS) in milli-Q water solution, identical to the protocol of Marbacher et al.8 After decellularization, the tissue was stored on ice in an Eppendorf tube filled with PBS until surgery later that day.
Surgical procedure
All surgeries in the recipient rats were performed under general inhalation anesthesia with isoflurane. For analgesia, subcutaneous carprofen (Rimadyl; Zoetis, Capelle aan de Ijssel, The Netherlands) injections were given for three consecutive days, starting at the day of surgery. All surgeries were performed under a surgical microscope (M500-N; Leica Camera AG, Wetzlar, Germany). Heart rate and blood oxygen levels were monitored with a pulse oximeter (PhysioSuite; Kent Scientific, Torrington, Connecticut, USA). Respiration was monitored visually. Temperature was controlled by placing the rat on a heating pad.
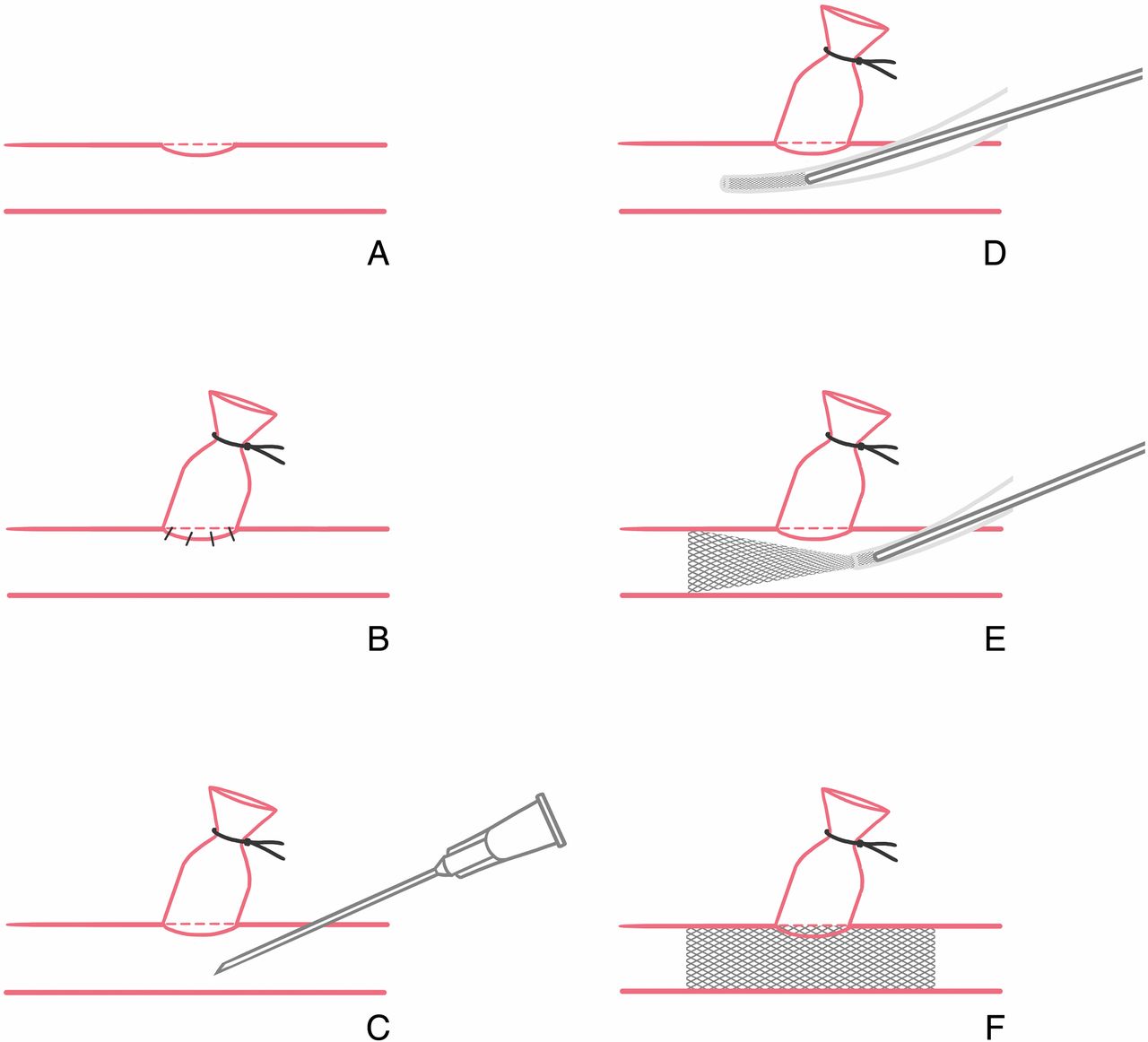
After achieving the appropriate plane of anesthesia, the abdominal aorta was exposed and the region between the aortic bifurcation and the renal arteries was dissected from the inferior vena cava and the surrounding connective tissues. The aorta above or below the iliolumbar arteries was considered optimal for end-to-side anastomosis creation. Surgical clips were used to temporarily ligate all side branches in order to prevent retrograde oozing, which can severely hamper visual inspection of the surgical site during anastomosis creation (figure 2A).

Surgical clips are used to ligate all side branches in the target area to prevent retrograde oozing during anastomosis creation (A). The aorta is clamped proximal and distal to the anastomosis site in order to create a small elliptical defect in the vessel wall (B).
Upon selection of the anastomosis site, the aorta was clamped proximal and distal to it and a small elliptical hole in the vessel was created (figure 2B). The lumen was subsequently rinsed with saline and heparin using a blunt needle. The decellularized pouch was cut in an oblique fashion and was placed at an angle of roughly 45–60° over the arteriotomy to allow for more jet flow inside the aneurysm, minimizing the risk for spontaneous thrombosis inside the aneurysm.10 Nylon 10-0 sutures (Serag-Wiessner, Naila, Germany) were used to attach the decellularized donor pouch to the aorta (figure 3B).

After creation of the aneurysm (A, B), a 27 Ga needle is used to puncture the aortic wall distal to the aneurysm (C). A 22 Ga Venflon is gently navigated through the aorta in a proximal direction. When the Venflon covers the ostium of the aneurysm, the pusher is introduced (D). The Venflon is carfully retracted (E) to unsheathe the flow diverter (F).
After creation of the end-to-side anastomosis, a thin film of topical tissue adhesive (Gluture; Abbott Laboratories, Maidenhead, UK) was used to ‘seal’ the connection between the aneurysm and aorta. This step was essential as the chance for bleeding was high due to the administered antiplatelet drugs. After application of the tissue adhesive, the distal clamp was removed to allow for backflow and to see if bleeding occurred. Subsequently, the proximal clamp could also be removed and the aneurysm should pulsate, with a marked volume increase during the peak arterial pulse wave.
Flow diverters
The FDs used in this experiment consisted of either 20 cobalt chrome wires and 4 platinum wires or 30 cobalt chrome wires and 6 platinum wires. Both implants were Surpass FDs that were custom-made for this experiment in rat aortas by Stryker Neurovascular (Fremont, California, USA).
We transferred the FDs from their 3.3 Fr custom-made catheters into a 20 Ga Venflon (Becton Dickinson Infusion Therapy, Helsingborg, Sweden). In order to push the FD out of the Venflon into the aorta, we adjusted the Venflon needle and removed the tip so that the end of the needle could push out the implant into the aorta.
Immediately after creation of the anastomosis we implanted the FD. The aorta was clamped again proximal and distal to the aneurysm. A 27 Ga needle was used to puncture the aorta wall distal to the aneurysm (figure 3C), which was used as a point of entry for the Venflon containing the FD. We gently navigated the Venflon through the aorta in a proximal direction, thereby covering the ostium of the aneurysm (figure 3D). When the Venflon bridged the aneurysm, the pusher was introduced into it and was held in place while retracting the Venflon in order to gently unsheath the FD (figure 3E).
We subsequently closed the entry point for the Venflon, again using 10-0 nylon sutures and a thin film of topical tissue adhesive to ‘seal’ the defect and prevent bleeding. The aortic clamps and surgical clips were all removed if no bleeding occurred and the surgery was completed (figure 3F).
Dual antiplatelet therapy
In order to prevent thrombosis inside the FD, dual antiplatelet therapy was given. A daily dose of 5 mg/kg clopidogrel was given, based on previous findings.11 In addition, we administered 1 mg/kg/day acetylsalicylic acid, which is an antithrombotic dose in humans and is known to inhibit 75% of platelet aggregation in Wistar rats.12 Both clopidogrel and acetylsalicylic acid were administered daily via oral gavage. Dual antiplatelet therapy was started at least 3 days before surgery and lasted for the remainder of the experiment.
Surgical outcome measures and tissue harvesting
Several surgical parameters were registered: time necessary to perform the operation (operation time); time needed to clamp the aorta to create the sidewall aneurysm (aortic clamping time); time needed to create the sidewall aneurysm (anastomosis time); time until bleeding stopped after sidewall aneurysm creation (hemostasis time); and time needed to clamp the aorta to place the FD (aortic clamping time FD). All rats were assessed on a daily basis while receiving antiplatelet therapy. Body weight, abnormal animal behavior and appearance, and postoperative complications were registered.
One week (n=12), 1 month (n=12), and 3 months (n=12) after surgery the rats were anesthetized again and underwent another laparotomy. After visual inspection, the aorta was clamped above and below the level of the FD and the aortic section including the FD and aneurysm was excised, flushed with saline and fixed overnight in 4% formalin. Tissues obtained were dehydrated through a graded ethanol series and embedded in methylmethacrylate. The tissues were then sectioned with a saw microtome (SP1600; Leica Microsystems, Eindhoven, The Netherlands) and underwent subsequent H&E staining.
Results
Full deployment of the FD implant could be seen in all cases by direct visual assessment under the surgical microscope during surgery. The mean±SD operation time was 126±23 min. Mean±SD aortic clamping times were less than 41 min (40.7±9.4 min) during anastomosis creation and less than 25 min (24.5±6.4 min) during FD implantation. The mean±SD hemostasis time was 10.4±3.8 min (table 1).
Surgical characteristics (n=36)
The mortality rate was 5.6% as two rats were lost due to unforeseen perioperative and postoperative complications. One rat died as a result of hemorrhage at the surgery site the night after surgery and the other rat died after 50 days of follow-up. Necropsy did not reveal any hemorrhagic or thromboembolic complications and the exact cause of death remains unknown.
No wound infections were encountered during follow-up and all rats displayed normal behavior after surgery during follow-up. Body weight showed a mean±SD increase of 13.1±8.0 g, 56.0±17.2 g, and 135.2±35.2 g in the 1 week, 1 month, and 3 months groups, respectively.
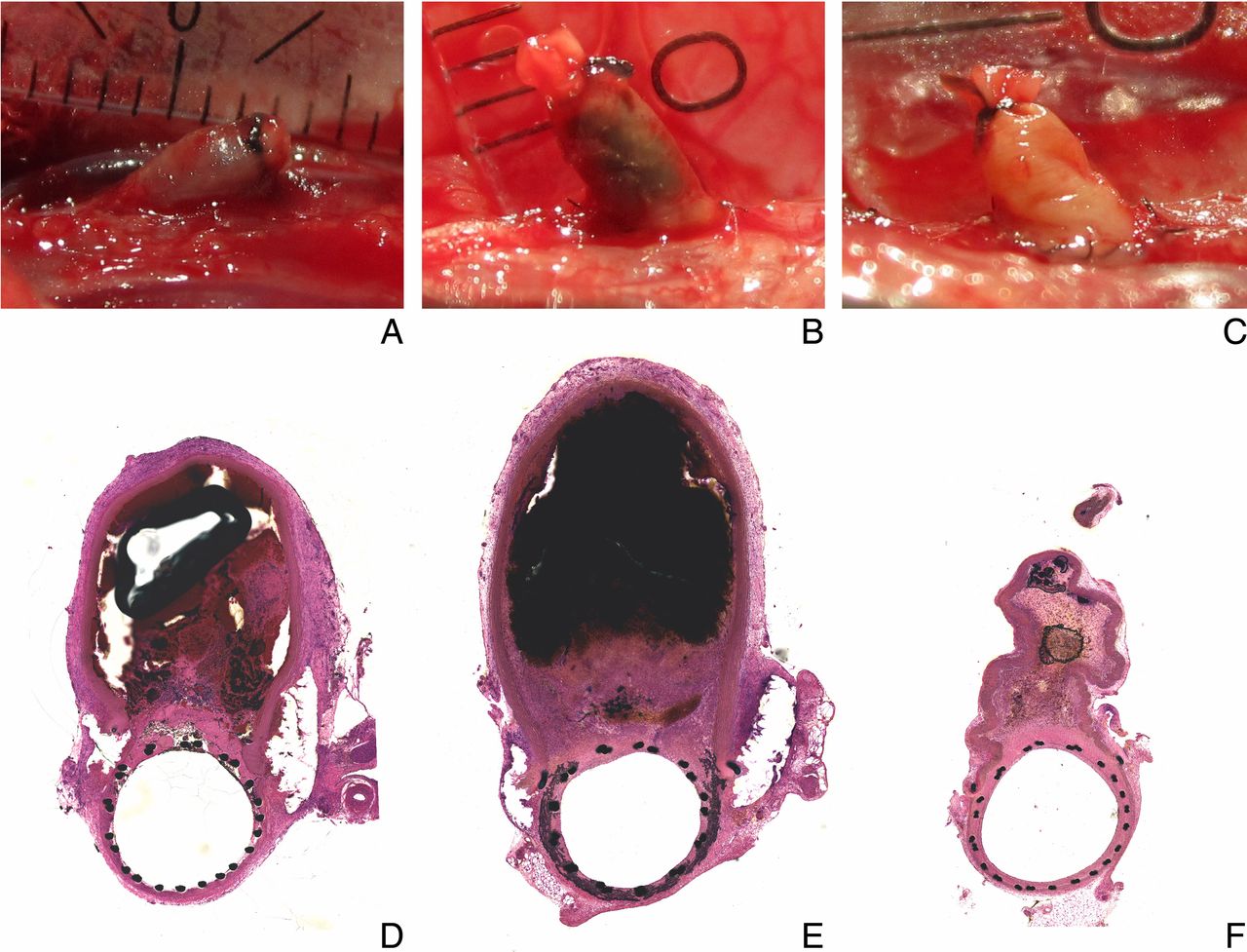
Macroscopic assessment at time of sacrifice revealed a clearly thrombosed aneurysm 1 week (figure 4A) and 1 month (figure 4B) after surgery. Three months after surgery the aneurysms seemed to be shrinking and were filled with soft tissue (figure 4C). Basic histology confirmed these macroscopic observations and showed thrombosed aneurysms after 1 week (figure 4D) and progressive fibromuscular tissue replacement of the thrombus starting from the aorta (1 month, figure 4E) and eventually filling up the entire aneurysm (3 months, figure 4F). The abdominal aorta was patent in all cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Macroscopic and microscopic (10×) overview of aneurysms at time of sacrifice showed initial thrombus formation at 1 week (A, D), gradual soft tissue ingrowth at 1 month (B, E), and complete soft tissue filling at 3 months (C, F). Abdominal aortas remained patent during follow-up (D–F).
Discussion
In this study we describe how a FD can be implanted in a surgical rat sidewall aneurysm model. Aneurysm creation in this animal model has been described in great detail,8 ,9 but this is the first study to demonstrate the feasibility of using this model to place FDs over the aneurysm.
The operated rats were sacrificed after a maximum of 3 months. During the study all rats displayed normal body weight increase and behavior after surgery. Mortality was very low (5.6%, n=2) and in only one case was it hemorrhagic in nature as bleeding at the surgery site occurred the night after laparotomy. No thromboembolic complications were seen.
The aortic clamping time was much longer than the clamping times reported by Marbacher et al.8 The implantation of the FD in part explains the increased aortic clamping time. Dual antiplatelet therapy also led to impaired hemostasis and demanded a more careful, and therefore more time-consuming, surgical approach. A vena cava or aorta rupture or puncture during surgery can be devastating in combination with the dual antiplatelet therapy. The relatively long aortic clamping times are possible in Wistar rats because of collateral vascularity capable of supplying the lower limbs during infrarenal aortic clamping.13
After 3 months we observed complete aneurysm occlusion, which is comparable to results reported for surgical sidewall aneurysms treated with FDs in rabbits and dogs.7 The rabbit elastase model and complex canine aneurysm models show markedly lower occlusion rates after FD implantation with 3 months of follow-up.7 The similarities and differences found in all of these models might lead to a better understanding of aneurysm healing after FD placement in a clinical setting.
What sets this surgical rat sidewall aneurysm model apart from other animal models is that the aneurysms are prone to growth and rupture when left untreated.9 The loss of endothelium and smooth muscle cells in the aneurysm pouch mimic the late stages of aneurysm pathology,14 and are in contrast with rabbit and dog models in which vessel wall cellularity is preserved.3 ,15 The low mortality rate (5.6%) is an additional advantage and is slightly lower than the mortality rate reported for the rabbit elastase model (8%).3
Another benefit of our model is the availability of rat strains with hypertension.16 This offers the opportunity to study implant efficacy under more strenuous, and clinically relevant, conditions in the future. Future studies might also benefit from the expanding knowledge regarding the rat genome. Thanks to the Rat Genome Database, data regarding genomic, genetic, phenotype, and strain for the laboratory rat is curated, validated, and made accessible through major databases such as NCBI.17
Although the microsurgical rat model is not a perfect representation of human aneurysms, it is ideal for testing new endovascular treatment options due to the reproducibility of the model. A possible disadvantage of our model is the overlap between the tissue reaction in response to microsurgery and the healing response of the aneurysm due to FD placement. The precise effect of this overlap on aneurysm healing is unclear at this moment. A way to further refine the animal model, and to circumvent the overlapping surgery-induced healing and FD-related aneurysm healing, is by creating the anastomosis first and by placing the FD at a later time point. Inclusion of angiography to assess aneurysm patency and volume increase before FD implantation would be an important addition in that case. This is technically feasible as we already successfully used the ventral tail artery as a point of entry for a microcatheter to inject contrast agent into the abdominal aorta in a pilot study (unpublished data). Further tests are warranted.
The aorta lacks the tortuosity of intracranial arteries, which makes this model less suitable to test FD wall apposition and the performance of new device delivery catheters. The use of large animal models such as canine models may be more appropriate in these cases.
Systemic arteries have a vasa vasorum, which is lacking in intracranial arteries in both humans and rats.18 ,19 Although the harvested thoracic aorta segment has no functional vasa vasorum due to the decellularization process, it is unknown if the presence of vasa vasorum in the abdominal aorta influences aneurysm healing after FD placement. Further study and comparison with the findings of the intracranial aneurysm rat model of Hashimoto et al20 might help to explain this discrepancy.
The addition of this model to study the mechanisms of FD complications could add value to the existing armamentarium of preclinical animal models. The decellularized aneurysm can be considered a ‘worst case scenario’ for the vessel wall condition, which might provide further insight into the development of next generation devices.
References
Footnotes
Contributors RA, MJG, WPJL, JdV: conception, design. RA, DS: data acquisition, data analysis. RA: drafting the manuscript. DS, MJG, WPJL, JdV: revising the manuscript. RA, DS, MJG, WPJL, JdV: final approval of the submitted manuscript.
Funding This work was supported by Stryker Neurovascular.
Competing interests MJG: research grants (money paid to institution): NIH, CereVasc LLC, Gentuity LLC, Philips Healthcare, Cook Medical, Neurogami, Codman Neurovascular, Microvention/Terumo, Stryker Neurovascular, Advanced Catheter Therapies, Medtronic Neurovascular, Wyss Institute, InNeuroCo, Bracco, Neuravi; fee-per-hour consulting: Codman Neurovascular, Stryker Neurovascular; travel support to Clot Consensus Group Meeting: Neuravi; stock: InNeuroCo; honorarium: Mt Sinai Department of Neurosurgery. JdV: research grants (money paid to institution): Stryker Neurovascular; fee-per-hour consulting: Stryker Neurovascular.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data available upon request.