Article Text

Abstract
Solitaire FR stent-based mechanical thrombectomy provides clinical benefit in selected patients with acute ischaemic stroke due to large vessel occlusion. A dreaded device complication that is associated with poor technical and clinical outcome is stent detachment. Retrieval of the detached stent can be technically challenging and has been attempted with variable success. The key benefit of this strategy is the lack of need to administer fibrinolytic/antiplatelet agents that can potentially be catastrophic in the setting of acute stroke. Therefore, retrieval may be preferred to other strategies (balloon angioplasty, lytic/glycoprotein 2b/3a inhibitors administration) to address detached stent. We report two patients in whom the detached stent was retrieved using alternative techniques—‘deploy and engage’ and ‘loop and snare’—as snare retrieval failed.
- Device
- Intervention
- Stent
- Stroke
Statistics from Altmetric.com
Background
Solitaire FR stent-based mechanical thrombectomy has emerged as an important strategy to recanalise large vessel occlusions. A dreaded device complication that is associated with poor technical and clinical outcome is stent detachment. The reported incidence of device-related complication ranges from <1% to 13%.1–5 Retrieval of detached stent has been attempted with variable results.1 ,2 ,6 Alternative strategies including balloon angioplasty and intra-arterial administration of antiplatelet and fibrinolytic agents have been described to establish reperfusion.6 However, use of lytic/dual antiplatelet agents can potentially be catastrophic in the setting of acute stroke. Retrieval of the stent therefore remains the desired strategy in these patients. We report two patients in whom the detached stent was retrieved using novel strategies and discuss the key technical aspects underpinning stent retrieval.
Case presentation
Case 1
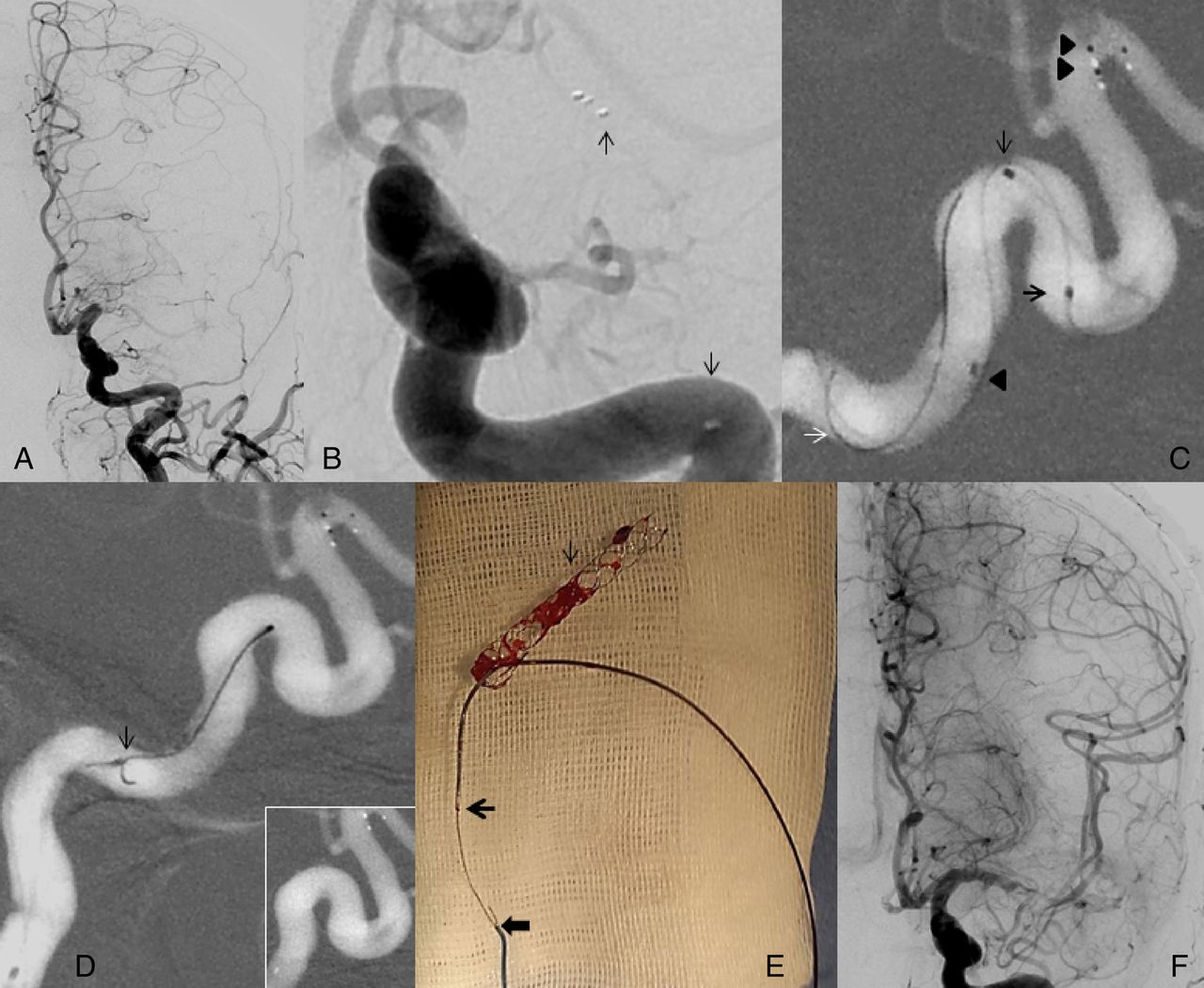
A 71-year-old man presented within 2 hours with global aphasia and right-sided weakness (NIH Stroke Scale (NIHSS) score 22). Multimodal CT imaging revealed a NCCT ASPECTS of 10, occlusion of the left internal carotid artery (ICA) from the origin and distal left M1 middle cerebral artery (MCA) and A2 anterior cerebral artery (ACA). Intravenous thrombolysis was deferred due to recent stroke. Thrombolysis In Cerebral Infarction (TICI) 3 reperfusion was established in the MCA territory after a single pass with a Solitaire 4×40 mm stent (Irvine, California, USA). Following this, during the second pass for the A2 ACA thrombus, stent detachment occurred. The proximal radio-opaque marker of the detached stent was noted abutting the wall at the proximal genu of the cavernous ICA. There was no flow in the ACA territory. Snare retrieval with an Amplatz goose neck microsnare (4 mm) (Plymouth, Minnesota, USA) failed. Stent-based retrieval was therefore performed with a Solitaire 4×40 mm stent (figure 1). TICI 3 reperfusion was established in the ACA territory and the modified Rankin Scale (mRS) score at 3 months was 1.

(A) Left A1 anterior cerebral artery (ACA) and M1 middle cerebral artery (MCA) occlusion (black arrows). (B) Left A1 ACA occlusion (black arrow), Thrombolysis In Cerebral Infarction (TICI) 3 reperfusion in left MCA territory. (C) Native image showing deployed stent in left A2–A3 ACA. (D) Distal (white arrow) and proximal (black arrow) markers of the detached stent. (E) Distal end of the detached stent (large white arrow), distal end of the second stent (black arrow), proximal end of the detached stent (white arrow) and distal marker of the microcatheter (large black arrow). (F) Post-stentectomy digital subtraction angiogram showing TICI 3 reperfusion.
‘Deploy and engage’ technique
The ‘deployment’ step involves partial deployment (distal radio-opaque markers have expanded and are apposed to the wall of the ICA) of an appropriately sized Solitaire device proximal to or within the detached stent. The ‘engagement’ step involves advancing the ‘microcatheter/partly deployed stent complex’ in an attempt to engage the proximal part of the detached stent. The proximal stent is then resheathed to capture the proximal legs/struts of the detached stent. Following this, the microcatheter, device and detached stent are retrieved (figure 2).

Line art demonstrating the ‘deploy and engage’ technique. (A) ‘Deployment’ step involves partial deployment (distal radio-opaque markers have expanded and are apposed to the wall of the internal carotid artery) of an appropriately sized Solitaire device proximal to or within the detached stent. (B) ‘Engagement’ step involves advancing the ‘microcatheter/partly deployed stent complex’ in an attempt to engage the proximal part of the detached stent. (C) ‘Capture’ stent: the proximal stent is then resheathed to capture the proximal legs/struts of the detached stent.
Case 2
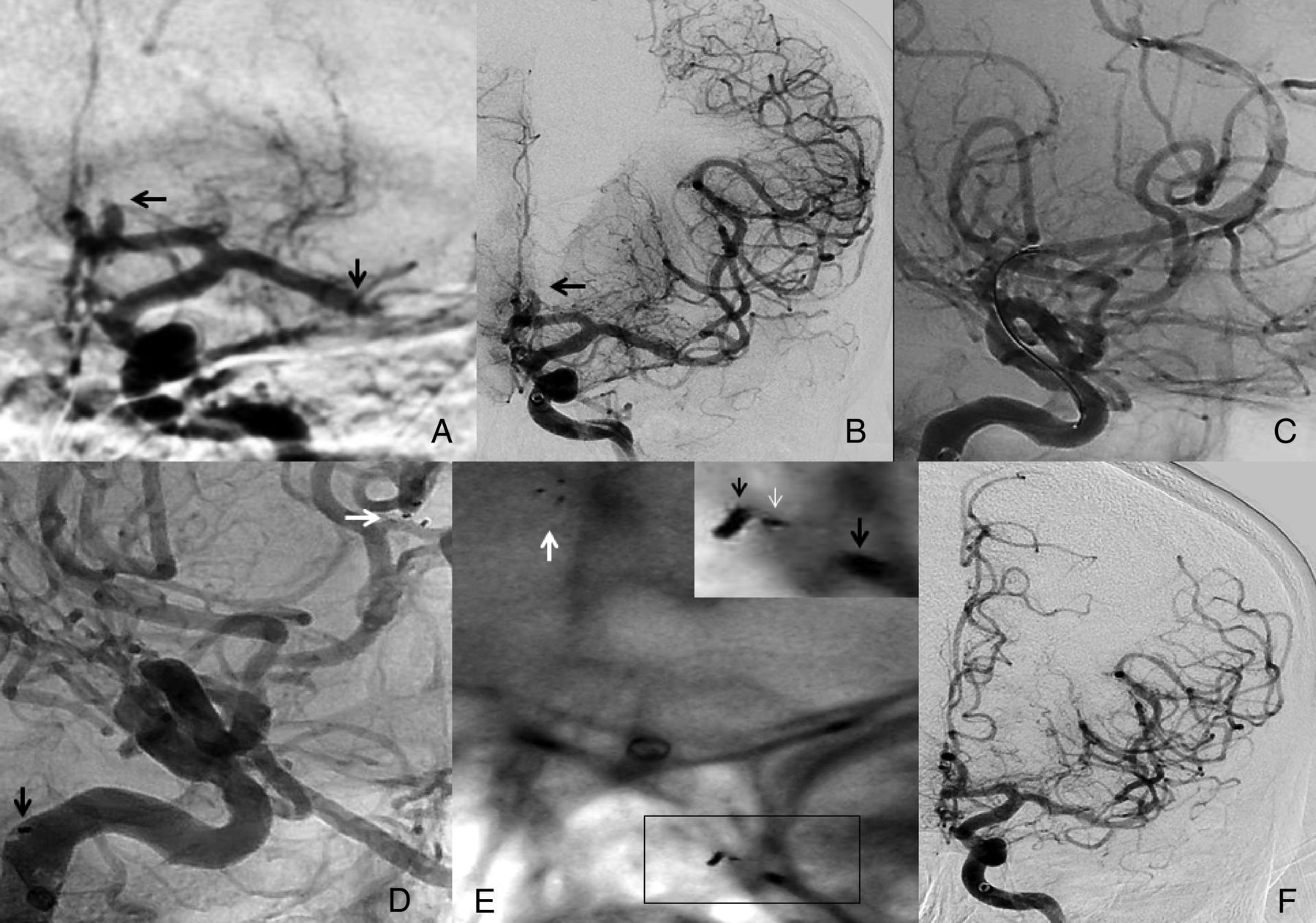
A 50-year-old woman presented at 3.5 hours with global aphasia and right-sided weakness (NIHSS score 21). Multimodal imaging revealed left M1 MCA occlusion and a small core. Intravenous thrombolysis was deferred due to recent myocardial infarction. Stent detachment occurred during the third pass with a Solitaire 4×40 mm stent. Both snare and stent-based retrieval failed. A ‘loop and snare’ technique was employed and the stent was retrieved successfully. TICI 2a reperfusion was established (figure 3).
(A) Occluded proximal left M1 middle cerebral artery (MCA). (B) Detached stent—distal and proximal markers (black arrow); left M1 MCA is occluded. (C) Distal end of the detached stent (black double arrowheads); proximal marker of the detached stent (black single arrow head); proximal (bold black arrow) and distal marker (black arrow) of the microcatheter; microwire (white arrow). (D) Snaring of the microwire (black arrow) (inset: road map showing distal and proximal markers of the removed stent). (E) Detached stent (black arrow); microcatheter distal end (bold black arrow); snare (solid black arrow). (F) Thrombolysis In Cerebral Infarction (TICI) 2A reperfusion.
‘Loop and snare’ technique
A small-calibre microcatheter (Echelon 10, Irvine, California, USA) with a curved tip (steam-shaped) is advanced through the detached stent. The microwire is navigated through the struts and back into the parent artery to form a loop. The microcatheter is then navigated over the microwire into the parent artery. A 4 mm snare is advanced into the parent artery and the microwire is snared. Following this, the microcatheter and snare are pulled back together with an attempt to retrieve the stent (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
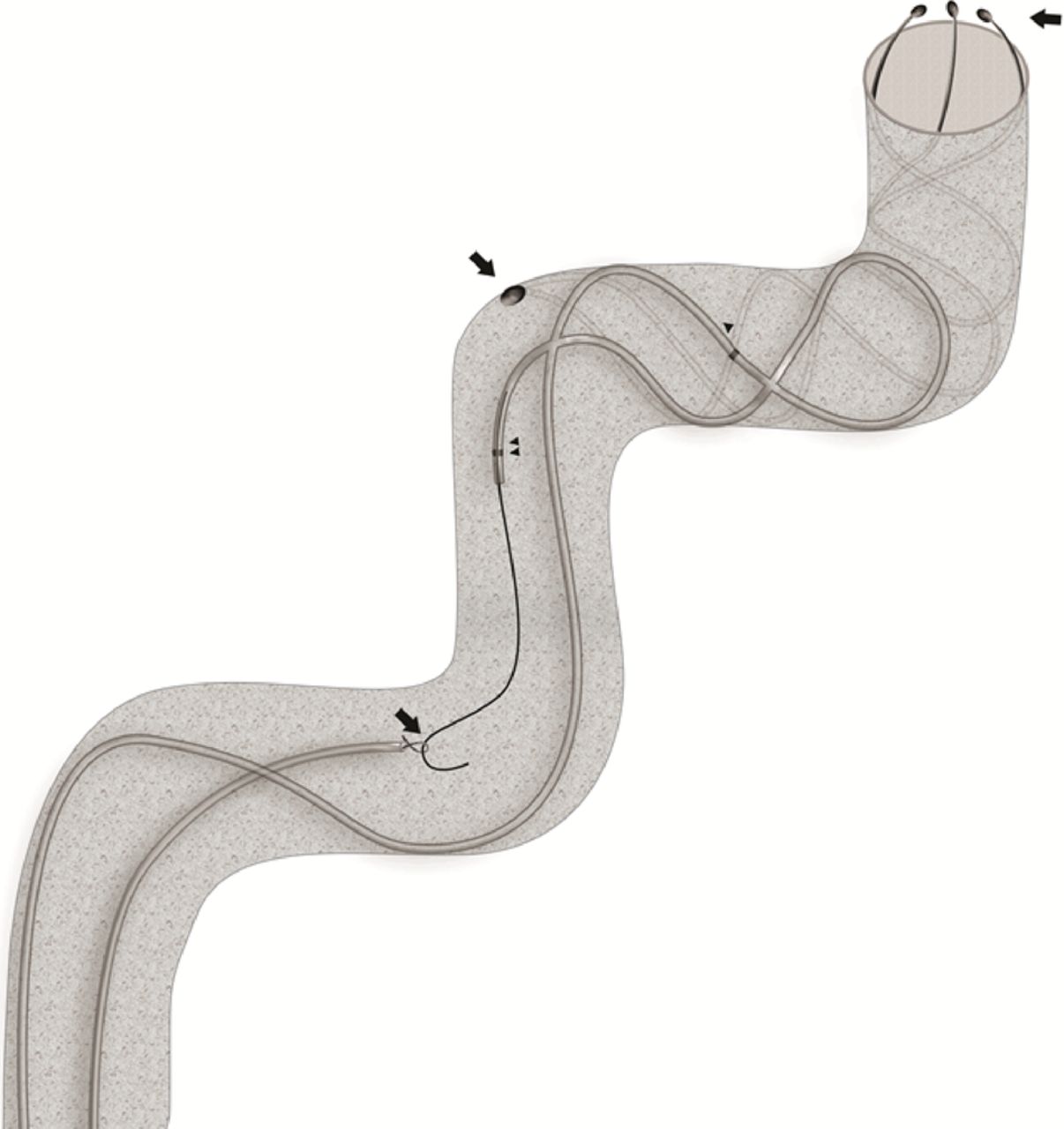
Line art demonstrating the ‘loop and snare’ technique. Bold arrows proximal to distal indicate the microwire through the loop of the snare; proximal marker of the detached stent; distal markers of the detached stent. Single black arrowhead indicates proximal marker of the microcatheter; double black arrowheads indicate distal marker of the microcatheter.
Discussion
Stent detachment is not uncommon during mechanical thrombectomy, and an in vitro study revealed that detachment commonly occurred at the site of the proximal marker band and not the detachment zone. The proximal marker band houses the ball and socket joint and it appears to be the weak site that tends to detach with the tensile forces.7 Stent detachment can occur prior to the third pass and the predisposing patient factors include large calcified plaque, a hard or lengthy thrombus and tortuous anatomy. Furthermore, the application of undue forward force during proximal stent deployment around curves can cause bending at the proximal marker band resulting in detachment at the ball and socket joint. Interestingly, resheathing appeared to offer some protection from detachment while retrieving around bends and not in straight anatomy.7 ,8
Stent retrieval precludes administration of dual antiplatelets and appears to be an important strategy to establish flow. Castano et al 8 reported on successful snare retrieval in most type ‘A’ detachments (proximal to radio-opaque marker). However, this technique failed in type ‘B’ detachment (distal to radio-opaque marker).8 Failed retrieval is likely when the proximal marker is positioned at an unfavourable angle abutting the wall of the artery or is not visualized. Alternative strategies to retrieve detached stents are therefore necessary.
A review of the literature revealed no description of techniques other than snare retrieval to retrieve detached Solitaire stents in acute ischemic stroke. In our report, alternative techniques were employed as snare retrieval failed. In theory, stent-based retrieval appears to be suitable for both types of detachment as engaging the struts in the proximal end of the detached stent is not technically challenging. However, the key limitation is that capture by resheathing may not provide a strong hold onto the detached stent during retrieval and detachment of the second stent. A resheathable stent without a distal wire is ideal for this technique. Chapot et al 9 have described stent-based retrieval of misplaced or thrombosed stents used in adjunctive coiling. When stent-based retrieval fails, the rescue strategy that can be employed is the loop and snare technique. The key benefit is dual control: the microwire can be manipulated and the loop of the snare appropriately positioned to enable snaring with relative ease. Looping the catheter through the struts of the stent can be potentially challenging; a small caliber curved tip catheter can be used to overcome this limitation. The technique can be employed to remove displaced stents during stent-assisted coiling.
Key messages
Stent detachment is a dreaded device complication that is mostly associated with a poor outcome.
Stent retrieval precludes administration of fibrinolytic/dual antiplatelet agents that can potentially be catastrophic in patients with acute ischemic stroke.
The ‘deploy and engage’ and ‘loop and snare’ techniques for Solitaire stentectomy may be acceptable alternative strategies to retrieve stents in the event of stent detachment.
Footnotes
Republished with permission from BMJ Case Reports Published 12 August 2016; doi:10.1136/bcr-2016-012547
Contributors RP, VG: planning, conduct and reporting of the work. GG: conduct and reporting of the work. AM: reporting of the work.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Dataset available from the Dryad repository.