Article Text

Abstract
Background Aneurysmal subarachnoid hemorrhage is a potentially devastating condition, and among the first priorities of treatment is aneurysm occlusion to prevent re-hemorrhage. An emerging strategy to treat patients whose aneurysms are not ideal for surgical or endovascular treatment is subtotal coiling followed by flow diversion in the recovery phase or ‘plug and pipe’. However, data regarding the safety and efficacy of this strategy are lacking.
Methods A retrospective cohort study was performed to evaluate the efficacy and safety of ‘plug and pipe’. All patients with a ruptured intracranial aneurysm intentionally, subtotally treated by coiling in the acute stage followed by flow diversion after recovery, were included. The primary outcome was re-hemorrhage. Secondary outcomes included aneurysm occlusion and functional status. Complications were reviewed.
Results 22 patients were included. No patient suffered a re-hemorrhage, either in the interval between coiling and flow diversion or in follow-up. The median interval between aneurysm rupture and flow diversion was 3.5 months. Roy–Raymond (R-R) class I or II occlusion was achieved in 91% of target aneurysms at the last imaging follow-up (15/22(68%) R-R 1 and 5/22(23%) R-R 2). Complications occurred in 2 (9%) patients, 1 of which was neurological.
Conclusions Overall, these data suggest that subtotal coiling of ruptured intracranial aneurysms followed by planned flow diversion is both safe and effective. Patients who may most benefit from ‘plug and pipe’ are those with aneurysms that confer high operative risk and those whose severity of medical illness increases the risk of microsurgical clip ligation.
- aneurysm
- flow diverter
- hemorrhage
- subarachnoid
Statistics from Altmetric.com
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is a potentially devastating condition that confers high rates of morbidity and mortality. Improvements in microsurgical and endovascular techniques, coupled with dedicated neurocritical care, have contributed to the steady improvement in clinical outcomes after aSAH over the past three decades.1–3 However, treatment challenges remain. Microsurgical clip ligation of ruptured aneurysms is made more difficult than comparable, elective cases by the presence of subarachnoid blood products, which obscure visualization of relevant anatomy, vasospasm, brain edema, and systemic ill effects of aSAH, which increase the risk of prolonged anesthesia. Although coil embolization of ruptured aneurysms is relatively fast and less invasive, complete and durable endovascular occlusion is dependent on aneurysm and parent vessel anatomy. Often, ruptured intracranial aneurysms cannot be fully occluded with coiling alone.
Flow diversion with the pipeline embolization device (PED; Medtronic, Irvine, California, US) is currently approved by the Food and Drug Administration for the treatment of large, wide necked, internal carotid artery (ICA) aneurysms.4 In addition, robust literature now supports using the PED for off-label treatment of both smaller anterior circulation aneurysms and posterior circulation aneurysms.5–8 Placement of a PED requires dual antiplatelet therapy (DAPT) to mitigate the risk of thromboembolic complications. Accordingly, the PED is overwhelmingly used to electively treat unruptured intracranial aneurysms given apprehension over giving DAPT in the acute phase following aSAH. Indeed, the current literature is limited to case reports and small series of patients who harbor ruptured ‘blister’ aneurysms or vertebral artery dissecting pseudoaneurysms for which limited surgical and endovascular options exist.9–14 An emerging strategy for the treatment of ruptured intracranial aneurysms is near complete coiling in the acute setting, followed by flow diversion in a delayed fashion for definitive treatment of the diseased artery.15 While conceptually appealing, few data exist to support this approach.
Consequently, the efficacy and safety of upfront coiling followed by staged flow diversion were retrospectively evaluated in a series of patients with aSAH managed endovascularly at a high volume, cerebrovascular, academic referral center. We hypothesized that upfront coiling, followed by flow diversion, or ‘plug and pipe’, effectively occludes the target aneurysm without an increased risk of delayed re-rupture.
Methods
Study population
Patients were culled from a prospectively maintained database of all patients treated by the cerebrovascular and neuroendovascular surgery service at a large, high volume, academic, referral center for complex neurovascular disease. All patients endovascularly treated for aSAH were identified. Of those, all patients whose aneurysms were intentionally, subtotally treated by coiling in the acute stage with the intention to pursue flow diversion with the PED after recovery, were included. As such, three included patients were referred to our center following aSAH and coiling of the ruptured aneurysm with the intention of definitive management by flow diversion after recovery, which is a relatively common referral pattern at our center.16 17 Patients who initially underwent balloon assisted coiling were included, but patients with stent coiled aneurysms were excluded.
The study was approved by the local institutional review board with a waiver of informed consent given the retrospective analysis of de-identified clinical data.
Data collection
Relevant demographic, clinical, and radiographic data were extracted from the electronic medical record. Patient age, sex, pertinent social and family history, Hunt and Hess (H&H) grade, Fisher grade, and functional status at discharge from initial hospitalization were recorded. Parameters of aneurysm size, location, and morphology were documented, as were the presence of coexistent, unruptured aneurysms. Interval to flow diversion, device used (first generation PED or Pipeline Flex), number of devices deployed, segments and vessels covered, adjuvant coiling, and stent post-processing (either with a balloon microcatheter or microwire) were recorded. Clinical and radiographic follow-up was analyzed, including functional status and aneurysm occlusion, as graded on the Roy–Raymond Scale (R-R).18 19 All complications were reviewed and reported.
Outcome measures
Outcome measures were evaluated after the merging of data from the electronic medical record and the institutional picture archiving and communication system. The primary outcome was aneurysm re-rupture between initial coiling and flow diversion. Additional outcomes included aneurysm occlusion, functional status as graded by the modified Rankin Scale (mRS), and complications.
Procedural details
All patients underwent standard aneurysm coiling for the treatment of aSAH in the acute phase. The goal of initial treatment was maximal, safe coiling of the ruptured aneurysm without risk of parent or branch vessel occlusion. In all cases, the presumed rupture point (either dome or daughter lobule) was fully coiled. Following recovery from aSAH, patients were prepared for flow diversion. DAPT was initiated with aspirin (ASA) and a P2Y12 inhibitor, either clopidogrel or ticagrelor. Initial dosing of ASA was either 325 mg or 81 mg daily when paired with clopidogrel or ticagrelor, respectively. Dosing of both ASA and the selected P2Y12 inhibitor was adjusted to achieve a therapeutic effect prior to placement of the PED on the basis of light transmission aggregometry.20 All PEDs were placed using a standard endovascular technique.
Statistical analysis
Data were analyzed with the Statistical Package for Social Sciences V.23 (SPSS Inc, IBM Corporation, Chicago, Illinois, USA). Continuous variables were graphed to evaluate frequency distribution. Normally distributed data are presented as mean (SD), while data that were not normally distributed are presented as median (IQR). Comparisons of medians and frequencies were completed using Mann–Whitney U and Fisher Exact testing, respectively. P<0.05 was considered statistically significant.
Results
Population and aneurysm characteristics
Overall, 22 patients underwent acute phase coiling of an aneurysm after aSAH; 21 patients suffered SAH from a ruptured saccular aneurysm, while 1 was treated for an iatrogenic, medial wall, carotid cave ICA pseudoaneurysm caused during endoscopic, endonasal pituitary adenomectomy. The population was predominantly female (n=19, 86%). The median age of the study population was 57 years (IQR 49.3, 64.5; range 36–83). Only one patient (5%) had a familial history of aSAH, while seven patients (32%) were smokers. The distribution of H&H grades was as follows: grade 1 (n=3, 14%), grade 2 (n=2, 9%), grade 3 (n=11, 50%), grade 4 (n=4, 18%), grade 5 (n=1, 5%), and not applicable (n=1, 5%). The distribution of Fisher grades was as follows: grade 1 (n=1, 5%), grade 2 (n=3, 14%), grade 3 (n=0, 0%), grade 4 (n=16, 73%), unknown (n=1, 5%), and not applicable (n=1, 5%). Population demographics and characteristics are reported in table 1.
Population demographics and characteristics
Aneurysm characteristics and details of treatment are presented in table 2. The distribution of ruptured (target) saccular aneurysms that were coiled was as follows: posterior communicating artery origin (n=8, 36%), ophthalmic artery origin or clinoidal segment (n=7, 32%), superior hypophyseal artery origin (n=3, 14%), ICA terminus (n=2, 9%), and posterior inferior cerebellar artery origin (n=1, 5%). The median (IQR; range) maximal transverse dimension and absolute neck width were 8.8 mm (4.9, 13.3; 2.3–24.0) and 4.7 mm (3.6, 6.2; 1.8–8.3), respectively. The median (IQR; range) neck to dome ratio was 0.5 (0.3, 0.5; 0.3–1.6). All aneurysms were primary coiled at the time of their aSAH without any intraoperative rupture or thromboembolic complications.
Aneurysm and treatment characteristics
Initial coiling and vasospasm
All patients demonstrated continued aneurysm filling following initial coiling. R-R grade 3 residual filling was present in 20 (91%) patients, while R-R grade 2 residual filling was noted in 2 (9%) patients, both of whom harbored large ophthalmic artery origin ICA aneurysms. Of the 19 patients treated at our institution for the initial SAH (n=19), 9 (47%) developed radiographic vasospasm. All nine were treated with pharmacologically induced hypertension to achieve a sustained mean arterial pressure (MAP) >90 mm Hg per our institutional protocol. Additionally, all patients with vasospasm were treated with intraventricular nicardipine per our institutional protocol. Transient focal neurological deficits attributable to vasospasm occurred in two (22%) of the nine patients that developed vasospasm. Those patients underwent intra-arterial spasmolysis with verapamil injected into the ICA proximal to the affected vascular territory in addition to balloon angioplasty. One patient underwent angioplasty across the segment of the ICA that harbored the coiled aneurysm.
Flow diversion
The median (IQR; range) interval from coiling to flow diversion was 3.5 months (1.8, 5.3; 0.5–15). Adjuvant coiling was pursued in two (9%) patients at the time of PED placement. Patients who harbored multiple aneurysms numbered six (27%). A single additional aneurysm was discovered in five patients, while one patient harbored two aneurysms in addition to the ruptured aneurysm. All seven additional aneurysms were covered with a PED at the time of flow diversion.
Complications, as a result of flow diversion, occurred in two (9%) patients. One patient suffered monocular blindness as a consequence of ophthalmic artery occlusion. The second suffered an inferior epigastric artery avulsion and external iliac artery dissection that required an operative bypass by vascular surgery. No patients suffered re-hemorrhage in the interval between coiling and PED placement, or after PED placement.
Short and long term radiographic results
Radiographic outcome data are displayed in table 3. Short term radiographic follow-up was obtained in 21 (95%) patients. The median (IQR; range) duration between PED placement and first follow-up imaging was 6.0 months (6.0, 8.0; 2–12). Patients were imaged with DSA in the majority of cases (n=18, 86%), while the remaining three (14%) patients were imaged with time of flight, time resolved MR angiography. On initial follow-up imaging, 14 (67%) patients achieved R-R grade 1 (complete) occlusion of the target, or previously ruptured, aneurysm. R-R grade 2 (neck remnant) was achieved in three (14%) patients and grade 3 (filling of the aneurysm fundus) in four (19%) patients. Of the seven patients with incomplete occlusion on initial imaging (R-R grades 2 and 3), four (57%) underwent long term follow-up imaging. The median duration from PED placement to second follow-up was 8.0 months (IQR 8.3, 21.8; range 8–25). One patient demonstrated no change on repeat imaging (R-R grade 2, which remained grade 2). One patient achieved complete occlusion (R-R grade 3 to grade 1), while two patients improved from R-R grade 3 to grade 2. Of the seven bystander aneurysms, R-R grade 1 was achieved in six (86%), while one (14%) demonstrated continued filling of the fundus (grade 3) on initial follow-up imaging. The patient with R-R grade 3 filling on initial angiography went on to complete occlusion at the long term follow-up. In-stent stenosis was observed in one (5%) patient and was not flow limiting or symptomatic.
Radiographic follow-up and outcomes after flow diversion
Clinical outcomes
Clinical follow-up was completed for all patients. The median (IQR) time from PED placement to most recent clinical evaluation was 15.3 (9.8, 29.3) months. Fourteen (64%) patients underwent long term follow-up of >12 months. On the whole, functional status, as measured by mRS, improved between baseline assessments at the time of discharge following aSAH and the most recent follow-up. The distribution of mRS frequency at the time of discharge from initial hospitalization and most recent follow-up are shown in figure 1. No patient in the study population died.
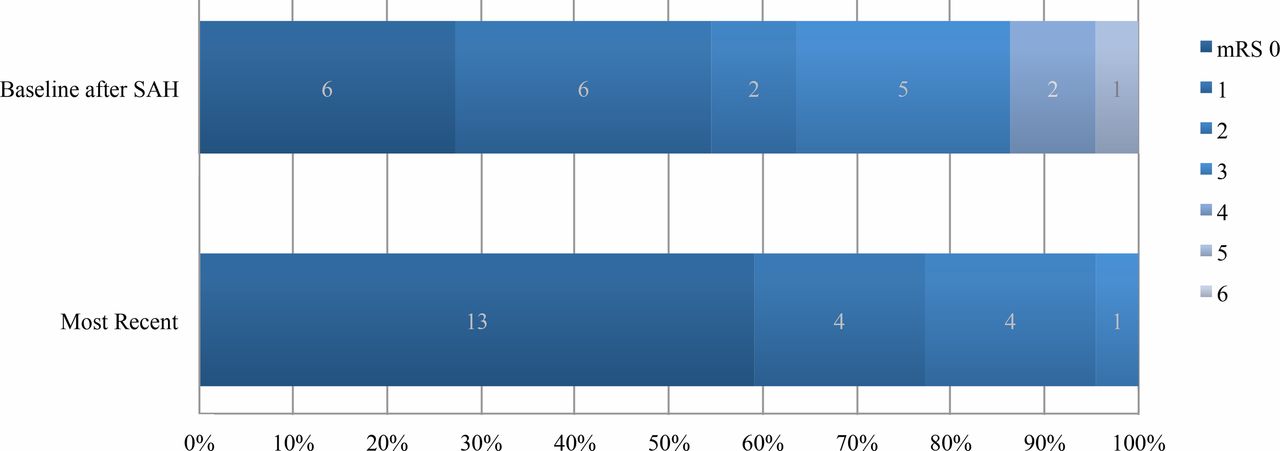
Frequency of modified Rankin Scale (mRS) scores at discharge following aneurysmal subarachnoid hemorrhage (aSAH) and at the last known follow-up. Functional status generally improved between baseline following aSAH and last known follow-up. No patient worsened in functional status over time. Only one patient not with a baseline mRS of 0 failed to improve at least 1 mRS grade. At baseline, 14 patients were discharged from hospital following aSAH with an mRS score of 0–2. At the last known follow-up, 21 patients achieved an mRS score of 0–2, leaving 1 patient with an mRS score of 3. No patient in the study group died.
Early versus late subgroup analysis
Subgroup analysis was completed to determine if changes in practice pattern occurred over time, as familiarity with the PED evolved. These data are presented in table 4. The population was divided into two cohorts: those treated between 2011 and 2014 and those treated between 2015 and 2017. The early and late cohorts were of equal number (n=11). The interval between initial coiling and flow diversion was equivalent between subgroups (median 3.0 months vs 4.0 months, P=0.748; Mann–Whitney U test). In addition, the rate of complete occlusion (R-R grade 1) was similar between groups (6 (55%) vs 8 (73%), P=0.66; Fisher Exact test). Likewise, the rate of R-R grade 1 or 2 on initial follow-up imaging was statistically equivalent between groups (7 (64%) vs 10 (91%), P=0.31; Fisher Exact test). The percentage of patients that underwent long term follow-up imaging was statistically smaller in the 2015 to 2017 cohort compared with the 2011 to 2014 cohort (2 (18%) vs 8 (73%), P=0.009; Fisher Exact test).
Evaluation of interval to flow diversion and occlusion between early and late cohorts
Discussion
Although not well studied, planned flow diversion following subtotal coil embolization may offer an effective treatment alternative for patients harboring ruptured aneurysms that are difficult to manage by traditional endovascular or microsurgical means. The principle concern regarding this strategy is that initial subtotal coiling is not immediately and completely protective against early and subacute aneurysm re-rupture. This is particularly concerning given that, in unselected cases, aneurysm re-hemorrhage following endovascular treatment is as high as 3.4% with the majority of subsequent ruptures occurring within the first week after treatment.21–23 Mortality from aneurysm re-rupture is as high at 75–100%.22–24 The only paper published to date advocating ‘plug and pipe’ as a strategy for the treatment of ruptured intracranial aneurysms included 31 patients, 1 of whom suffered a subsequent aSAH in the interval between coiling and flow diversion.15 No instances of delayed aSAH occurred in our population of 22 patients, either in the period between initial coiling and placement of the PED, or after flow diversion. These data suggest that an acceptable rate of aneurysm occlusion without excessive early complications or delayed re-hemorrhage may be achieved with judicious application of ‘plug and pipe’. Given these data, we advocate utilizing the ‘plug and pipe’ technique in selected cases for which traditional treatment modalities are judged impossible or of high risk.
Among several factors associated with early re-hemorrhage following endovascular coiling of ruptured intracranial aneurysms is extent of coiling. Multiple studies have shown that continued filling of the aneurysm fundus confers a higher risk of delayed re-rupture than aneurysms with a sessile neck remnant.22 23 25 In general, to achieve maximum safe coiling, density is the goal of initial treatment in our institution. In addition, our aim is to bring the coil mass as close to the neck as possible without risking prolapse of the coil into the parent vessel. To do so, balloon assistance for coiling is utilized liberally. If a suspicious daughter sac or obvious point of rupture is noted on pretreatment angiography, care is taken to occlude these regions of the aneurysm preferentially.
Patient selection is largely driven by a myriad factors. Expected patient compliance with medications and the proposed treatment course, as well as anatomic factors, are important aspects when considering whether to employ ‘plug and pipe’. Compliance with DAPT is the predominant modifiable factor to deliberate, as strict adherence to the prescribed regimen is imperative to limit thromboembolic complications. If unable to firmly adhere to DAPT, ‘plug and pipe’ should not be considered. Additionally, if a patient is not reliable for follow-up, a more immediately definitive treatment of the aneurysm, such as microsurgical clip ligation, is required. Contrarily, patients who are high risk for complications related to a craniotomy, such as older patients, those with a high H&H grade, who present in vasospasm, or patients with severe medical comorbidities, are favorable candidates for ‘plug and pipe’.
Vascular anatomy is a paramount consideration when deciding to pursue ‘plug and pipe’. Aneurysms that are surgically treacherous, but amenable to flow diversion, are ideal candidates for this strategy. The anatomic variants for which we advocate ‘plug and pipe’ are generally commensurate with those for which elective flow diversion is widely considered (a typical case is presented in figure 2). Generally, ‘plug and pipe’ is a viable option for carotid, vertebral, and some middle cerebral artery sidewall aneurysms. Roy et al previously showed that 66% of fetal posterior cerebral artery (fPCA) aneurysms treated with the PED continued to opacify (R-R grade 3) on long term follow-up imaging, while fewer than 10% were completely occluded (R-R grade 1).26 One patient in the current cohort was treated for a ruptured fPCA aneurysm, which on initial follow-up imaging after PED placement continued to fill, but was completely occluded at 12 months. Despite a good radiographic outcome in this case, we have nearly ceased treating fPCA aneurysms with flow diversion, either in the setting of ‘plug and pipe’ or electively, with select exceptions.
{kind=link}
{kind=link}
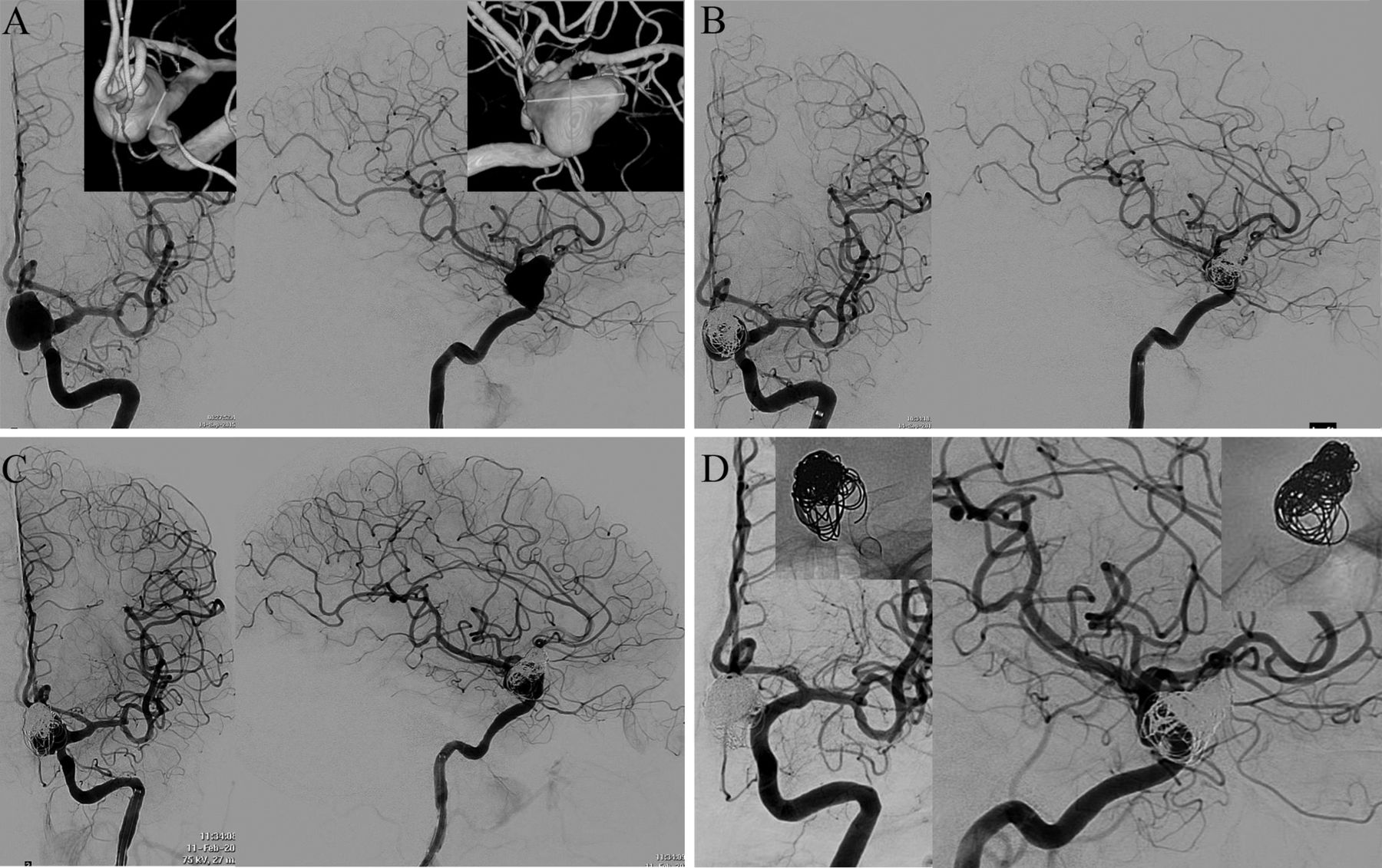
Case example of a patient selected for ‘plug and pipe’. The patient was elderly with multiple medical comorbidities at the time of initial presentation. Hunt and Hess and Fisher grades were both 4 on presentation. (A) Pre-coiling AP and lateral angiograms reveal a large, wide neck, right ophthalmic artery origin ICA aneurysm. Insets demonstrate three-dimensional reconstructions that show the neck (7.3 mm) and maximum transverse dimension (17.2 mm). The neck to dome ratio was 0.54. (B) Consistent with the ‘plug and pipe’ strategy, the aneurysm was subtotally coiled. (C) Follow-up angiography revealed coil compaction and significant recurrence of the aneurysm at 4 months, at which time flow diversion was completed with two PEDs. (D) Angiography 8 months following flow diversion showed complete occlusion of the aneurysm and reconstruction of the parent vessel. Insets reveal AP and lateral X-rays to visualize the coil mass and PED construct. AP, anterior-posterior; ICA, internal carotid artery; PED, pipeline embolization device.
Moreover, the PED is increasingly used for off-label indications, including smaller aneurysms and aneurysms in the distal or posterior circulations, with excellent results.27 A putative advantage of ‘plug and pipe’ is treatment of adjacent segment, bystander aneurysms within the flow diverter construct. Indeed, six patients in our cohort harbored bystander aneurysms that underwent treatment via flow diversion at the time of PED placement. In all cases, the presumed ruptured aneurysm was identified on the basis of size or morphology, and if this could not be determined with relative certainty, then the patient was treated by clip ligation. Altogether, seven bystander aneurysms were treated with 100% R-R grade 1 occlusion. This is an important advantage of the ‘plug and pipe’ technique as these aneurysms portend a rupture rate that is significantly higher than comparable aneurysms in patients without a history of SAH.28
This study is not without limitations, the most conspicuous of which is the retrospective design adds obvious bias to patient selection, which cannot be accounted for. While overall outcomes were good—acceptable rates of occlusion (15/22 (68%) R-R grade 1 and 5/22 (23%) R-R grade 2 at the most recent follow-up imaging) with no delayed re-hemorrhage and limited ischemic complications—these data may not be generalizable. Lastly, 68% complete occlusion is subpar relative to surgical clipping. For patients who are not suitable surgical candidates, ‘plug and pipe’ seemingly provides a safe and effective treatment path. When including patients who achieved R-R grade 2 occlusion, the overall rate of ‘successful’ treatment improves to a rate commensurate with traditional endovascular techniques. However, the aSAH risk from a small, sessile neck remnant following PED placement remains unknown. Accumulating data suggest that small neck remnants following flow diversion pose little risk of aneurysm recurrence or hemorrhage,29 30 but the PED has not been used for sufficient duration to make predictions about the long term behavior of aneurysms with R-R grade 2 residual filling.
Conclusions
Overall, these data suggest that subtotal coiling of ruptured, intracranial aneurysms followed by planned flow diversion is both safe and effective. No instances of delayed aneurysm re-rupture were encountered in our cohort. Overall R-R grade 1 or 2 occlusion was achieved in 91% of patients. This series represents only the second analysis of such a cohort published in the literature, and as such, these data should be corroborated by additional series to best determine which patient populations and aneurysm types are most amenable to ‘plug and pipe’. Patients who may most benefit from ‘plug and pipe’ are those with aneurysms that confer high operative risk and those with high H&H scores or medical comorbidities that significantly increase the risk of microsurgical clip ligation.
References
Footnotes
BMH and JMF contributed equally.
Contributors BMH and JAG: study design, data collection, data analysis, drafting of the manuscript, revision and final approval of the manuscript, and study supervision. JMF and TPM: study design, data collection, and revision and final approval of the manuscript. JED, FCT, and CMC: study design, revision and final approval of the manuscript, and study supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by the institutional review board of Emory University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Any data analyzed for this study are available upon request from the corresponding author.