Article Text

Abstract
Background Femoral access is the traditional approach for endovascular carotid artery stenting. Radial access is increasingly used as an alternative approach due to its known anatomical advantages in patients with unfavorable aortic arch morphology via the femoral approach and its excellent access site safety profile. Our objective was to analyze procedural success using radial access for carotid artery stenting as reported in the literature.
Methods Three online databases were systematically searched following PRISMA guidelines for studies (n ≥20) using radial artery access for carotid artery stenting (1999–2018). Random-effects meta-analysis was used to pool the procedural success (successful stent placement with no requirement for crossover to femoral access), mortality, and complication rates associated with radial access.
Results Seven eligible studies reported procedural success outcomes with a pooled meta-analysis rate of 90.8% (657/723; 95% CI 86.7% to 94.2%; I2=53.1%). Asymptomatic radial artery occlusion occurred in 5.9% (95% CI 4.1% to 8.0%; I2=0%) and forearm hematoma in 1.4% (95% CI 0.4% to 2.9%; I2=0%). Risk of minor stroke/transient ischemic attack was 1.9% (95% CI 0.6% to 3.8%; I2=42.3%) and major stroke was 1.0% (95% CI 0.4% to 1.8%; I2=0%). There were three deaths across the seven studies (0.6%; 95% CI 0.2% to 1.3%; I2=0%). The meta-analysis was limited by statistically significant heterogeneity for the primary outcome of procedural success.
Conclusion Radial access for carotid artery stenting has a high procedural success rate with low rates of mortality, access site complications, and cerebrovascular complications. The potential benefits of this approach in patients with unfavorable aortic arch access should be explored in a prospective randomized trial.
- stent
- cervical
- intervention
- stenosis
- stroke
Statistics from Altmetric.com
Introduction
Endovascular carotid artery stenting is traditionally performed via femoral artery access. Alternative arterial approaches have been used in an effort to reduce access site complications as well as prolonged catheterization times in patients with difficult anatomical morphology such as bovine or type III aortic arches.1 2 Transbrachial access has been investigated, but is considered less favorable due to high rates of access site and ischemic complications resulting from its role as the primary supply to the upper limb.3
Transradial artery access is an increasingly popular alternative for carotid stenting due to positive results from its use in interventional cardiology where it has become the standard of care, progressively replacing femoral artery access.4 This trend has been driven by several factors including the known reduced incidence of access site complications,4 reduced risk of major bleeding,5 reduced ICU and hospital length of stay,4 5 and reduced costs to national health systems.6 In addition to these practical and safety-based indications, radial artery access is more comfortable and better tolerated by patients due to the distance of the artery from adjacent nerves as well as the ability to mobilize earlier post-procedure.7–9
Several moderate-sized studies have reported on procedural success rates using radial access in endovascular carotid artery stenting,10–13 including three studies with comparator femoral access control groups.2 14 15 No systematic review or meta-analysis has been published to provide a global view of the success rates.
Materials and methods
Our primary objective was to analyze the procedural success rate with radial artery access for endovascular carotid artery stenting. The secondary objectives were to examine crossover rates to femoral artery access, complication rates, and length of hospital stay when using the radial approach. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed,16 and the protocol was submitted to PROSPERO.
Study types
Eligible studies were randomized controlled trials, prospective cohort studies, prospective registries, retrospective cohort studies, and case–control studies published between 1999 and 2018. Case series, case reports, letters to the editor, commentaries, and conference abstracts were excluded. A minimum sample size of 20 patients was required to minimize inclusion of underpowered studies for the primary outcome, given the approximately 4–6% crossover rate to femoral access in the coronary intervention literature.5 17
Eligibility criteria (PICO criteria)
Eligible studies required participants with stenosis of the distal common carotid artery and/or proximal internal carotid artery treated by endovascular carotid artery stenting using radial artery access. Two-arm studies in which radial access was used in at least one arm were also eligible. Studies using transbrachial access were excluded.
Outcomes
The primary outcome was procedural success of stent deployment using radial artery access for carotid artery stenting without requirement for crossover to femoral artery access. The secondary outcomes were the crossover rate to femoral artery access, anatomical variations of the aortic arch (type I aortic arch, type II/III aortic arch, bovine arch), side of treatment (right vs left), procedural times, major access site complications (symptomatic radial artery occlusion, pseudoaneurysm), minor access site complications (asymptomatic radial artery occlusion, forearm hematoma), periprocedural (within 30 days) minor cerebrovascular events (transient ischemic attack (TIA) and stroke with increase in NIH Stroke Scale (NIHSS) score by <4 points) and major cerebrovascular events (increase in NIHSS score by ≥4 points), myocardial infarction within 30 days, mortality rate, and length of hospital stay. For studies containing two arms, complication rates were reported using intention-to-treat analyses.
Search strategy
Three online databases (MedLine via PubMed, Embase via Ovid, and Cochrane Library) were systematically searched by two independent reviewers (TJ, KB) using filters for English language articles, publication between 1999 and 2018, and the following search strategy: MeSH stents AND carotid AND radial. In addition, the reference list of a published non-systematic review article was cross-referenced.18
Selection of studies
Our review followed PRISMA guidelines. Duplicate records were removed. Titles and abstracts of the remaining records that met the inclusion criteria were independently identified in an unblended standardized manner by two reviewers (TJ, KB). Full-text articles identified records were then assessed in detail to ensure they met the inclusion criteria. Disagreements between reviewers were resolved by consensus; otherwise resolution was by a senior reviewer (TK).
Data collection
A standardized online data extraction sheet was created using AirTable (www.airtable.com), and the data were extracted from the eligible studies by one review author (TJ). The extracted data were checked by the second reviewer (KB).
Data synthesis and statistical testing
StatsDirect Version 3.1.22 (Cambridge, UK) statistical and meta-analysis software was used for all quantitative analyses. Proportions were calculated for binary variables and mean values for continuous variables. Proportions were pooled using random effects meta-analysis (DerSimonian and Laird model).
Heterogeneity testing and risk of bias assessment
Heterogeneity testing was performed using Cochran Q statistics to calculate I2 percentages; I2 ≥50% would indicate statistically significant heterogeneity. Bias risk assessment was undertaken by funnel plot analysis with SE on the y axis and proportion on the x axis, and calculation of Egger and Harbord–Egger statistics (α=0.05).
Results
Search results
A total of 170 records were identified through the three online databases (PubMed n=84, Embase n=82, and Cochrane Library n=4); 35 duplicates were excluded (see online supplementary material: PRISMA flow diagram). A prior review article was cross-referenced but no additional records were identified.18 After exclusion of 127 records through assessment of titles and abstracts, eight records were selected for full-text assessment by both reviewers. One article19 was excluded because it described preliminary results for the same patient sample reported in an included study.14
Supplemental material
Included studies
Seven studies were included in the final review and quantitative meta-analysis, all published between 2007 and 2018, describing 723 patients who underwent carotid artery stenting via radial artery access.2 10–15 Four studies were retrospective11 13–15 and three studies were prospective.2 10 12 The three most recent studies were two-arm studies (one prospective randomized controlled trial and two retrospective case–control studies) comparing radial with femoral access for carotid artery stenting.2 14 15 However, OR meta-analysis for the two-arm studies was ultimately not conducted due to the presence of only three studies of this design, which in our opinion would result in an underpowered meta-analysis.
Baseline demographics
Mean age was 69.4±1.1 years with 508 male patients (70.3%). There were more right-sided lesions (57.4%) than left-sided lesions (42.6%). Aortic arch morphology data grouped as type I (114/279; 40.8%) versus type II/III combined could be extracted from four of the seven studies,2 13–15 and bovine arch status (35/492; 7.1%) was reported in five studies.10–13 15 Pre-procedural stenosis was reported for five studies (µ 87.0±1.4%).2 10 12 14 15 Patient demographics, lesion characteristics, and equipment used in the seven studies are detailed in table 1.
Patient demographics and lesion characteristics for seven eligible studies assessing radial access for carotid artery stenting
Outcomes
The results of the meta-analysis, heterogeneity testing, and bias risk assessments are presented in table 2. Procedural success was achieved in 657 of 723 patients with a random-effects meta-analysis proportion of 90.8% (95% CI 86.7% to 94.2%; I2=53.1%). Mean procedural time was 40.5±7.0 min (95% CI 21.0 to 60.0). Three deaths were reported with a pooled meta-analysis proportion of 0.6% (95% CI 0.2% to 1.3%; I2=0%). No myocardial infarctions were identified within 30 days of the procedure. Major cerebrovascular events within 30 days of the procedure occurred in five of 723 patients (1.0%; 95% CI 0.4% to 1.8%; I2=0%) and minor cerebrovascular events in 16 of 723 patients (1.9%; 95% CI 0.6% to 3.8%; I2=42.3%).
Random effects meta-analysis of the primary and secondary outcomes, heterogeneity testing, and bias risk assessment
Two major access site complications occurred within a single study (with the largest sample size of 382 patients; one symptomatic radial artery occlusion in a patient with Buerger’s disease; one pseudoaneurysm in a patient who underwent crossover to transfemoral access),2 with none occurring in the other six studies (0.4%; 95% CI 0.1% to 0.9%; I2=0%). For minor access site complications, asymptomatic radial artery occlusion was identified in 32 of 540 reported patients from four studies (5.9%; 95% CI 4.1% to 8.0%; I2=0%),2 11 13 15 and forearm hematoma in three of 441 patients from six studies (1.4%; 95% CI 0.4% to 2.9%; I2=0%).2 10 12–15
Subgroup analyses
Subgroup analysis for the primary outcome stratified by aortic arch morphology was not conducted due to variable reporting of this outcome within arch subtypes. Four of the seven studies provided data on procedural success/crossover rates for type I versus type II/III arches2 13–15 and only three studies for bovine arch morphology.10 12 15
Heterogeneity and bias risk assessment
Meta-analysis for the primary outcome of procedural success was associated with statistically significant heterogeneity (I2=53.1%). No statistically significant heterogeneity was identified for the secondary outcomes (I2 <50%). No statistically significant bias risk was identified for the primary and secondary outcomes (p>0.05) (see table 2).
Discussion
Procedural success
Compared with coronary interventions, transradial carotid artery stenting has the additional technical challenge of selection of the common carotid arteries, which often requires use of reverse angle catheters.20 Adoption of the radial approach has therefore been limited in part by concerns over the feasibility of advancing a stable guiding system. These concerns may be overstated; two recent studies have reported high procedural success rates for transradial cerebral angiography with advancement of hydrophilic-coated reverse angle catheters into the internal carotid arteries.20 21 In addition, there are multiple reports describing successful transradial placement of guide catheters for mechanical thrombectomy and aneurysm coiling procedures.22–24
Based on the current literature, our meta-analysis suggests that radial access for carotid artery stenting has a high procedural success rate (90.8%). However, this rate is certainly lower than that reported in large transfemoral studies. Tokuda et al, in a retrospective analysis of a Japanese national registry containing 8458 eligible patients, reported a technical success rate of 99.5%.25 Shen et al reported transfemoral success rates of 96.2% for patients with type III aortic arch and 100% for type I/II arches.26 Burzotta et al reported significantly prolonged procedural times in patients with type III and bovine arch morphologies via a femoral approach.1 Conversely, Gao et al purposely included only patients with type III and bovine arch morphologies and reported a transradial success rate of 100% and a transfemoral success rate of 90.0% (see table 3).15
Patient demographics, lesion characteristics, and outcomes for two-arm studies with radial and femoral arterial access arms
These results suggest that the technical success and advantages of radial access for carotid stenting are highest in patients with unfavorable aortic arch morphology when using femoral access (ie, type III and bovine arches). Thus, the radial artery approach may be best viewed as complementing rather than competing with the femoral artery approach.
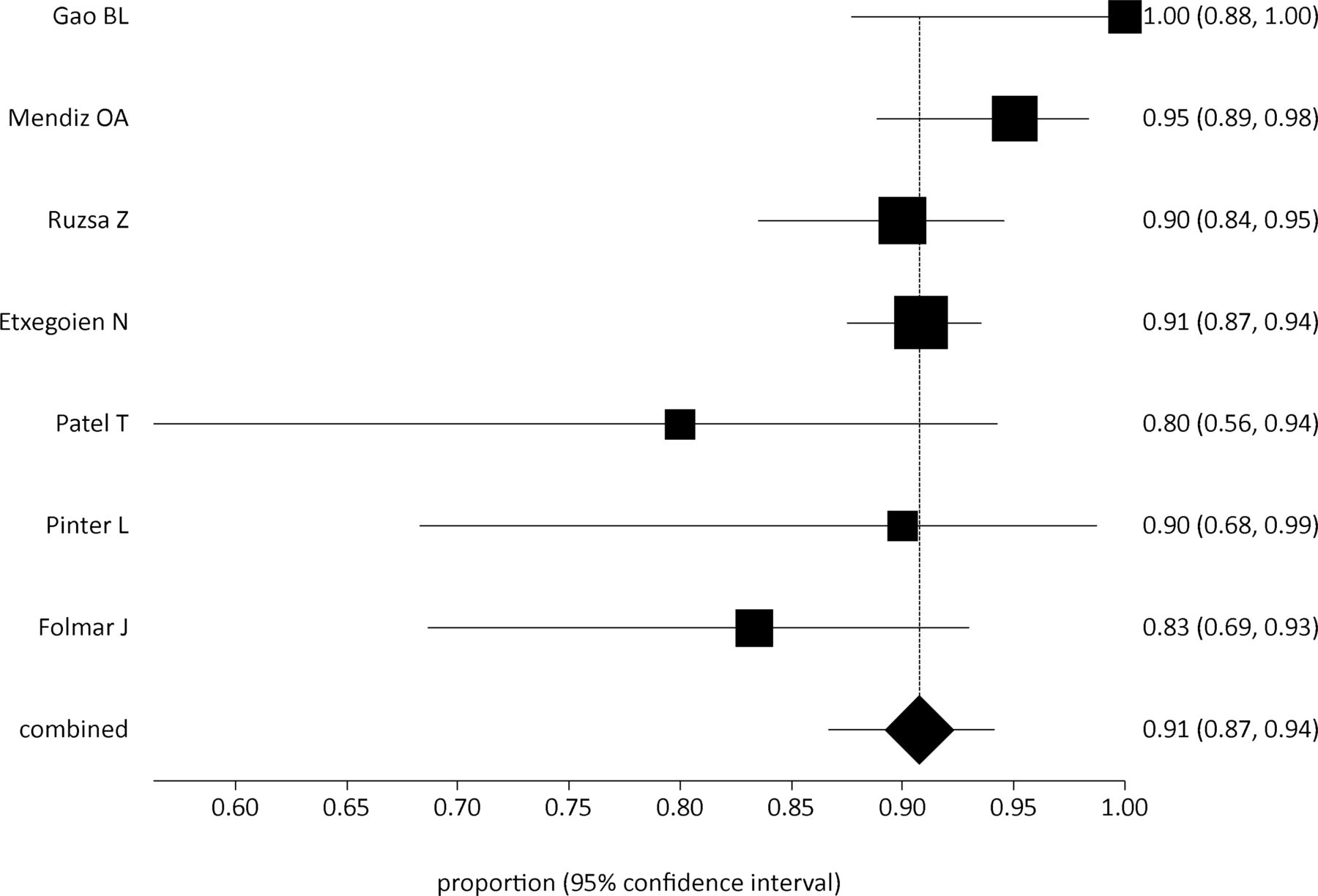
Our meta-analysis of the procedural success rate was associated with statistically significant heterogeneity (I2=53.1%). Assessment of the forest plot for procedural success (see figure 1) demonstrates three outlier studies for this outcome.10 12 15 Gao et al reported a 100% procedural success rate but purposely included only patients with type III and bovine arch morphologies, contributing to selection bias; in addition, their sample size was relatively small (n=28).15 Patel et al used an atypical contralateral radial approach (ie, left radial artery to access the right common carotid artery and vice versa), again with a small sample size (n=20), and reported a lower success rate of 80.0%.12
{kind=link}
Forest plot analysis of procedural success rates for transradial carotid artery stenting using DerSimonian and Laird random effects meta-analysis.
Folmar et al reported a procedural success rate of 83.3%, falling to 54% in patients with non-bovine (conventional) origin of the left common carotid artery.10 The study cited difficulty in maintaining stable guide system access in these patients as a contributing factor to failure. This may reflect a combination of inexperience with the procedure (first major publication) and the inherent limitations of radial access in this anatomical subgroup.
Thus, each of the three studies that contributed most to the heterogeneity for this outcome had underlying methodological and anatomical biases that added to the variance, although in opposing directions (100%, 80%, and 83.3%).10 12 15 The opposing impact of these studies on the mean result, although all contributing to variance (and thus I2 values), would have had a partially equilibrating impact on the pooled proportion in our meta-analysis (90.8%).
The mean procedural time of 40.5±7.0 min was pooled across five studies,2 10–13 and was lower than that reported in a previous transfemoral carotid stenting study (54±18 min).27
Contributors to procedural failure
Eight of 66 procedural failures were due to failed radial artery access, radial artery spasm, radial artery loop, or subclavian artery stenosis. Of these, seven were clustered in a single study2 which was the only prospective randomized controlled trial. This rate of failed radial access may be falsely low due to the non-randomized design of the other studies.
The remaining 58 procedural failures (22 right (37.9%), 36 left (62.1%)) resulted from inability to cannulate the relevant common carotid artery with the guide catheter/sheath (see table 2). Thirty-two of 36 left carotid lesion cases reported bovine origin status, of which 29/32 (90.6%) had non-bovine (conventional) origin. Two studies reported that, for right-sided lesions, the major contributor to failure was extreme angulation between the origins of the right subclavian artery and common carotid artery.11 14 For left-sided lesions, non-bovine status was considered the most important contributor to failure.2 10 11
Periprocedural complications
Three deaths were reported in our pooled analysis of 723 patients, with a low meta-analysis rate of 0.6% (95% CI 0.2% to 1.3%). This pooled rate is comparable with the mortality rate associated with transfemoral carotid artery stenting (0.7%).25 Two of these patients were from the same study (Rusza et al), a prospective randomized controlled trial with 130 patients in each arm2; one patient died from a major stroke occurring 20 days after successful transradial carotid artery stenting while the other patient underwent crossover to femoral access (for whom the cause of death was not reported but was not a result of stroke, major bleeding, or myocardial infarction).2 The third patient died after a major periprocedural stroke.11
The rates of periprocedural major stroke (1.0%; 95% CI 0.4% to 1.8%) and minor stroke (1.9%; 95% CI 0.6% to 3.8%) were also comparable to the literature on the transfemoral approach (1.5% and 1.3%, respectively).28 Interestingly, 13 of the 16 reported minor stroke/TIA events were from a single study (also the largest study with 382 patients), of which 10 events represented intra-procedural TIAs with the new symptoms resolving within 12 hours.11
Asymptomatic radial artery occlusion (ARAO) rates were reported in four2 11 13 15 of the seven studies (diagnostic criteria reported in table 1). The pooled rates of major (0.4%; 95% CI 0.1% to 0.9%) and minor (5.9% for ARAO; 1.4% for forearm hematoma) access site complications are low, and are consistent with that found in the coronary literature when using 6F sheaths29 (6F guiding sheaths used in six of the seven studies). The low rates of ARAO may also reflect the routine use of intra-arterial heparin during access and patent hemostasis during closure.2 11 15 29
Technical aspects
All seven included studies used a distal protection device. Six of the seven included studies2 10–14 initially placed a 4–6F 10 cm radial sheath in the right radial artery with intra-arterial injection of heparin and antispasmodics, performed angiography using a 5F Simmons catheter, and then exchanged the short sheath and catheter for a 90 cm 6F guiding sheath over an exchange length guidewire (see table 1). Difficulty advancing the guide was managed using a coaxial technique with a diagnostic catheter over the exchange wire and/or use of a buddy wire.11–14 The seventh study15 telescoped a 6F coronary guiding catheter over a Simmons-1 catheter into the common carotid artery using a coaxial technique without an exchange procedure. Recent literature on transradial neurointerventions report exchange of the short radial sheath for a 6F guiding sheath over a wire into the subclavian artery, with advancement of the guide into the carotid arteries using a telescoping technique over a 125 cm Simmons catheter.22–24 In addition, puncture at the level of the anatomical snuffbox is increasingly popular, allowing for arterial access with the forearm pronated and preservation of the artery at the level of the radial styloid.30
Limitations
Statistically significant heterogeneity (I2=53.1%) was present for the primary outcome of procedural success and its inverse of conversion to femoral access, but not for the other secondary outcomes (see section on Procedural Success). Major limitations of this meta-analysis were the small number of studies included (n=7), the wide range of sample sizes (20–382 patients), and the presence of studies influenced by selection and methodological biases (including aortic arch morphology and contralateral approach). As discussed in the Results section, the number of studies reporting procedural success rates stratified by aortic arch morphology subtype was insufficient for meaningful meta-analysis. Although this study would have been strengthened by OR meta-analysis of outcomes from two-arm studies, unfortunately there were insufficient eligible studies to allow for a meaningful analysis (n=3).
Complication rates were mainly reported using intention-to-treat analyses which reduces bias risk but may overestimate the true rate of complications. In addition, criteria for differentiation of major versus minor stroke was not clearly defined in two studies.2 11 Initial experience of the operators with the transradial approach for carotid stenting was reported in two studies13 15 with reported high experience rates in the others. Even though experience was not formally quantified in any of the studies, the presence of a learning curve was described in all studies.
Conclusion
Radial artery access for carotid artery stenting has a high rate of procedural success (90.8%) with low rates of death, periprocedural stroke, and access site complications. Transradial access may have anatomical advantages in patients with type III and bovine arch morphology, and future randomized studies should use inclusion criteria based on arch configuration.
Acknowledgments
None
References
Footnotes
Contributors TJ was the primary author of the study protocol, was one of the two reviewers, performed data extraction and collation, assisted with data analysis, and drafted and revised the manuscript. She is the guarantor. KB was one of the two reviewers, performed data quality checking, undertook the data analysis, and edited the manuscript. HK advised upon and edited the study protocol, assisted with data analysis, and edited the manuscript. EO advised upon and edited the study protocol, assisted with data analysis, and edited the manuscript. TK supervised the project, acted as the senior reviewer in cases of non-consensus, advised upon and assisted with editing of the protocol, advised upon the methodology, and edited and helped revise the manuscript. All authors assisted in the design of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.