Article Text

Abstract
A patient with a ruptured left sylvian fissure arteriovenous malformation (AVM) treated with primary transvenous Onyx embolization, and angiographically cured, is reported. The patient presented with a large intraparenchymal subopercular hematoma and there was angiographic demonstration of a pseudoaneurysm and single draining vein. Trans-arterial approaches were unsuccessful because of the en-passage nature of feeding arteries and hence a transvenous approach was used to embolize the pseudoaneurysm with Onyx. Follow-up angiography at 1 month revealed durable angiographic cure of the AVM. Our case illustrates that in patients with ruptured AVM secondary to pseudoaneurysm and single draining vein, transvenous treatment can be utilized to achieve occlusion of the pseudoaneurysm resulting in AVM cure. To our knowledge, this is the first description of a transvenous approach for endovascular therapy of AVM.
- Vein
- Hemorrhage
- Angiography
- Intervention
- Technique
Statistics from Altmetric.com
Endovascular therapy of brain arteriovenous malformation (AVM) is most commonly used in reducing the size of an AVM prior to surgical resection, or is used in conjunction with radiosurgery, and in some cases may lead to primary AVM cure.1–3 Another application of endovascular AVM therapy is to minimize AVM bleeding risk by occluding and protecting vascular features commonly associated with AVM rupture, such as intranidal aneurysms and pseudoaneurysms. The latter approach is especially relevant in patients presenting with ruptured AVMs. Traditionally, a trans-arterial approach has been utilized to embolize the AVM nidus. However, in the presence of indirect feeders or extreme vessel tortuosity, an arterial approach may not always be possible.
We describe successful transvenous embolization and angiographic cure of a ruptured AVM following an unsuccessful attempt at trans-arterial cannulation, and we discuss the strategy behind this approach. To our knowledge, this is the first report of transvenous embolization for brain AVM for primary treatment.
Case report
History and examination
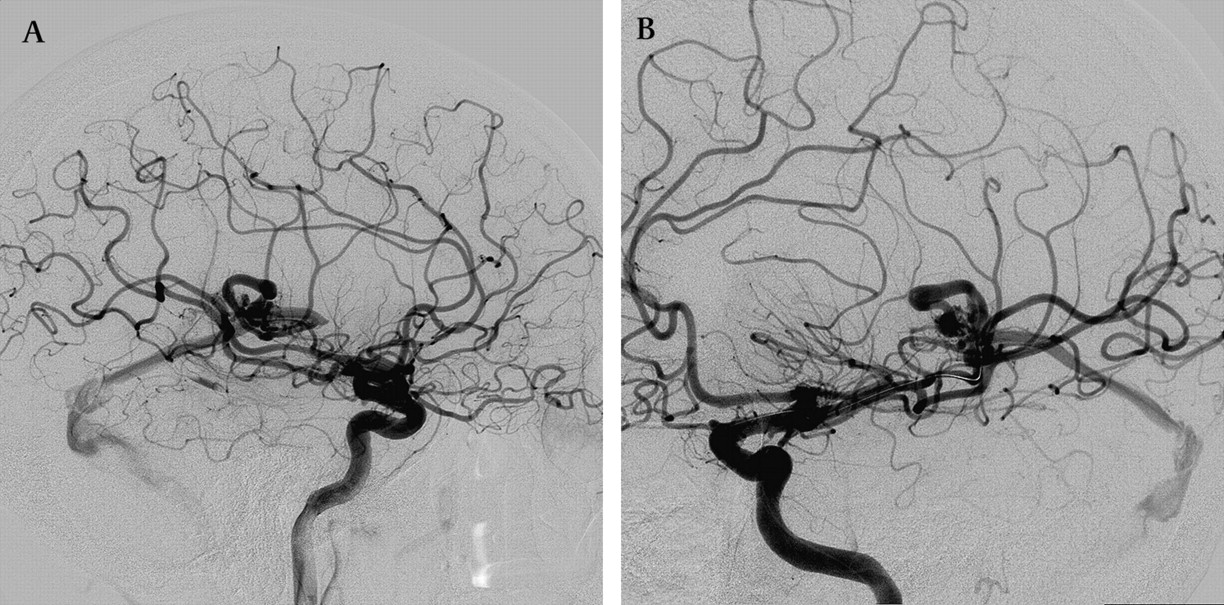
A patient in their 50s developed new onset of global aphasia and right hemiplegia. Unenhanced head CT showed a left infraopercular frontoparietal parenchymal hematoma measuring 6 cm×3 cm×3 cm (figure 1). Angiography confirmed a left sylvian fissure Spetzler Martin grade 2 AVM (1 point for size, 1 point for eloquent location), with moderately brisk flow characteristics. There was an indirect arterial supply via en-passage vessels and a small AVM nidus, measuring less than 1 cm in maximum diameter. A dilated saccular pouch immediately proximal to the draining vein represented a pseudoaneurysm or venous varix; the vein drained into a small Vein of Labbe which subsequently drained into the left transverse sinus (figure 2A,B).

Head CT demonstrating large left frontotemporal 6.6×3.2 cm hemorrhage.
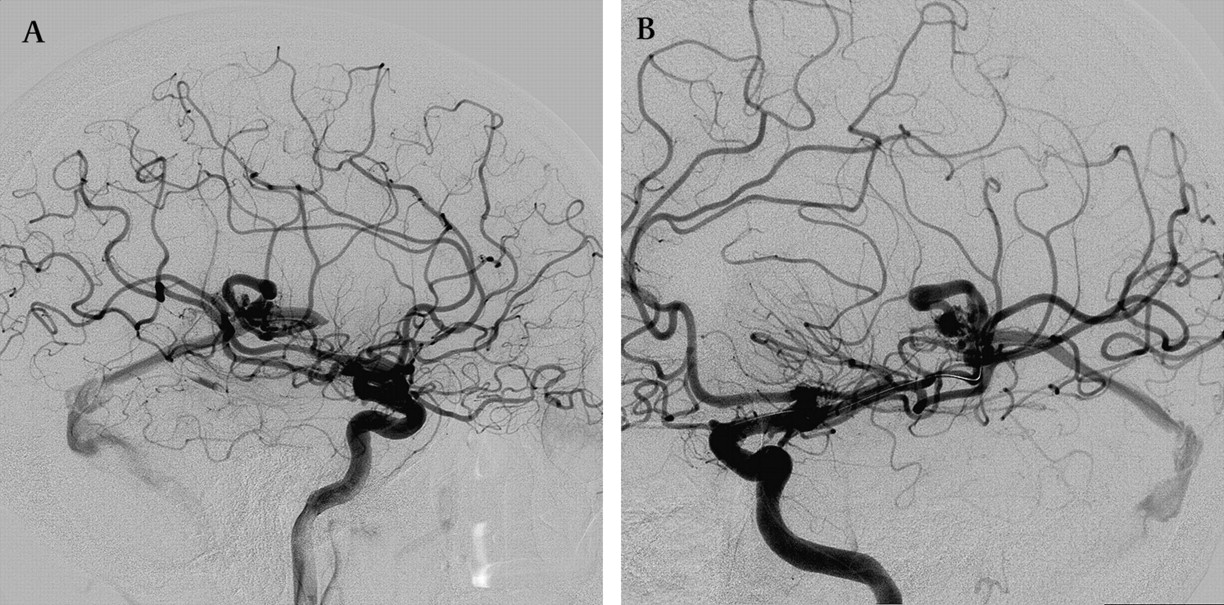
Angiography images (A) lateral and (B) oblique, show left frontal arteriovenous malformation supplied by indirect left middle cerebral artery feeder arteries and associated pseudoaneurysm.
Operation
A 6 French guide catheter was placed in the left internal carotid artery through which initial diagnostic angiography was performed. A microcatheter (Ultraflow; ev3, Irvine, California, USA) was placed in the superior division of the left middle cerebral artery with microguidewire guidance (Expedion 0.010; ev3). Superselective angiography demonstrated en-passage arterial supply to the AVM via multiple small feeding arteries. Multiple attempts to access the individual AVM feeding arteries were unsuccessful due to vessel tortuosity and their small caliber.
Following multiple unsuccessful efforts at cannulating arterial AVM feeding vessels, venous access was secured in order to access the saccular pouch in a retrograde manner. A 6 French sheath was placed in the left common femoral vein. The left jugular vein was accessed with a 6 French guide catheter. A microcatheter (Prowler 14; Cordis, Raynham, Massachusetts, USA) was negotiated in an antegrade approach with a 0.014 microguidewire (Synchro; Boston Scientific, Fremont, California, USA) through the arterial tree to the middle cerebral artery M1/M2 junction in order to provide road map guidance. Using microcatheter arterial road mapping, another microcatheter (Marathon; ev3) was advanced in a transvenous retrograde manner to the left Vein of Labbe, over 0.010 and 0.008 microguidewires (Expedion and Mirage; ev3) (figure 3A). Once access to the venous pouch was achieved, Onyx 34 was injected slowly to form a plug at the arterial junction of the pouch, resulting in stasis of flow confirmed by arterial injections. At this point, a second embolic injection of Onyx 18 was performed in order to complete retrograde nidal occlusion (figure 3B).

Via transvenous approach, the pseudoaneurysm is (A) accessed and (B) embolized with Onyx.
The completion control angiogram demonstrated occlusion of the draining vein and angiographic AVM cure (figure 4A,B). The procedure was complicated by branch occlusion of the previously cannulated left Rolandic feeder artery. This occlusion was demonstrated on the pre-embolization angiogram following initially attempted distal trans-arterial cannulation, and was treated unsuccessfully with 5000 units of intravenous heparin and 5 mg of intra-arterial verapamil following transvenous embolization (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Control angiogram (A) lateral and (B) oblique demonstrates angiographic cure of the arteriovenous malformation but occlusion of the attempted cannulated arterial branch.
Postoperative course
The postoperative course was complicated by generalized seizures on the day following the procedure, and treated with intravenous levetiracetam. Neurologic follow-up examination at 3 weeks revealed global dysphasia and persistent right-sided hemiplegia, which was largely unchanged from the patient's pre-procedure baseline status. Angiography follow-up at 3 weeks demonstrated persistent angiographic cure. Unfortunately, the patient died from other unrelated medical causes at 3 months.
Discussion
The risk of rebleeding after acute cerebral AVM rupture is broad, ranging from 2% to 18% in the first year.4–6 When an acutely ruptured AVM is diagnosed, angiography is often performed to identify risk factors for bleeding, such as feeder artery or intranidal aneurysms, pseudoaneurysms or venous outflow restriction.1 If identified, early treatment is recommended, particularly for pseudoaneurysms and intranidal aneurysms, to prevent re-hemorrhage.7
In our patient with a ruptured AVM, pseudoaneurysm and a single draining vein, our primary intention was to use an arterial approach to occlude the possible pseudoaneurysm to prevent re-rupture or, alternatively, to reduce trans-arterial flow to the AVM nidus. However, due to the principal consideration of small caliber en-passage feeder arteries and inability to navigate distally due to vessel tortuosity, we were not able to access the possible pseudoaneurysm safely, and hence pursued transvenous embolization as a last resort. We used an initial high concentration of embolic material (Onyx 34) to have as much in situ filling of the sac as possible and to prevent downstream migration. Once initial occlusion of the possible pseudoaneurysm was achieved, we augmented embolization with a second injection of Onyx 18, with the goal of achieving retrograde filling into the nidus. As a result, occlusion of the venous sac was achieved, with angiographic cure of the AVM.
Transvenous retrograde nidus sclerotherapy under controlled hypotension (TRENSH) has been proposed as a treatment to select AVMs to avoid ischemic complications when delivering embolic agents via a trans-arterial route.8 Transvenous embolization has been commonly used to treat dural arteriovenous fistulas, which is thought to be the most effective and durable treatment for this disease.9 Our patient's AVM exhibited similar hemodynamics as with a fistula, with a single draining vein. The vein was primarily draining the AVM and demonstrated moderately brisk flow characteristics, hence transvenous embolization was considered feasible and eventually led to angiographic cure of the AVM. It is possible that such an approach may be of unique value, once safety and efficacy have been demonstrated, in patients with multiple en-passage AVM feeding vessels.
There are several risks to the transvenous approach in embolization of an AVM. There is the undefined and concerning risk of AVM rupture during initial closure of the venous segment but before nidal penetration. Blood pressure reduction, initial occlusion of accessible arteries and temporary trans-arterial assisted balloon occlusion may help reduce the risk of AVM rupture during transvenous embolization although these maneuvers likely also increase procedural risk. Another disadvantage to the transvenous approach is that if embolization at the fistulous or nidal penetration could not be achieved, complete or partial outflow obstruction and cortical reflux may occur and lead to delayed hemorrhage, or to venous occlusive syndromes and parenchymal congestion. Microcatheter retrieval may result in avulsion due to the thinner and more fragile venous wall. Finally, migration of embolic material into the pulmonary vasculature may lead to pulmonary embolism. Because of these risks, we highlight that transvenous therapy should only be used in patients for whom traditional approaches cannot be used or are contraindicated. We consider this approach, at the current time, as a ‘last approach’ option.
There are several limitations in our case report. We are unable to histologically confirm that the described vascular dilatation was a nidal aneurysm, pseudoaneurysm or venous sac, as angiographic interpretation is imperfect.10 11 However, in spite of the differential histologic considerations, we felt that the morphologically dilated vascular sac suggests a high risk of re-hemorrhage and therefore considered this finding a target for therapy.
Although it is conceivable that iatrogenic occlusion of the initially accessed arterial branch, due to thrombosis, spasm or dissection, assisted in angiographically curing the AVM, we note that following the initially demonstrated branch occlusion (prior to transvenous cannulation), early venous shunting was still identified.
We believe that in select AVM cases, where anatomically supportable, and especially in acute cases of hemorrhage with concerning angiographic features at high risk for rebleeding, transvenous embolization may be considered. However, an exclusive transvenous approach may raise the risk of hemorrhage. At the current time, we suggest that such an approach should only be reserved for patients in whom all other traditional therapies have been exhausted, cannot be used or are contraindicated.
References
Footnotes
Please note the content of this manuscript has been altered to protect the identity of the patient.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.