Article Text

Abstract
Background Embolization of intracranial arteriovenous malformations (AVMs) is generally a preoperative adjunctive procedure in the USA. However, sometimes embolization can result in complete angiographic obliteration of the AVM. There is significant controversy regarding the best management strategy for this subset of patients. There is a scarcity of literature predicting which embolized, angiographically obliterated AVMs are likely to recur and which ones are cured. We present our series of patients with complete obliteration of their AVMs from embolization.
Methods A prospectively maintained database identified 122 patients who underwent embolization of an intracerebral pial AVM with liquid embolics. Eighteen patients (15%) achieved complete angiographic obliteration of the AVM with embolization. We followed several parameters to assess possible predictors of recurrence.
Results Fifteen of 18 patients (83%) had angiographic/anatomical follow-up to assess for AVM recurrence and 3 (17%) refused angiographic follow-up. Three patients underwent surgical resection with intraoperative angiography despite complete AVM obliteration with embolization alone. Thirteen of the 15 (87%) patients with follow-up remained obliterated at time of follow-up, and all of these patients had an embolic cast that had a similar morphology to the AVM nidus. Two of 15 patients (13%) had AVM recurrence, both of whom had incomplete embolic nidal opacification (proximal pedicle embolization).
Conclusions A minority of intracranial AVMs can be safely obliterated with stand-alone embolization. Proximal occlusion of feeding arteries appears to be associated with recurrence. Prospective studies with longer follow-up and larger patient numbers are necessary.
- Arteriovenous malformation
- endovascular
- embolization
- angiographic obliteration
- artery
- embolic
- malformation
- angiography
- intervention
Statistics from Altmetric.com
- Arteriovenous malformation
- endovascular
- embolization
- angiographic obliteration
- artery
- embolic
- malformation
- angiography
- intervention
Introduction
Surgical resection has been the historic definitive treatment to cure intracranial arteriovenous malformations (AVMs) with good surgical risks.1 2 The development of stereotactic radiosurgery has expanded the armamentarium for the treatment of intracranial AVMs, achieving cure for many small AVMs. Endovascular embolization of AVMs has significantly evolved since described by Luessenhop and Spence3 in the 1960s. Early embolization materials were deployed proximal to the AVM and the flow toward the AVM carried the embolic material toward the feeding pedicles and sometimes the nidus.4 This technique was prone to recanalization as the particles dissolved, and it was associated with high complication rates.4 Since that time, the development of liquid embolics, such as n-butylcyanoacrylate (n-BCA) (TruFill n-BCA; Cordis Neurovascular, Miami Lakes, Florida, USA) and ethylene vinyl alcohol copolymer (EVOH) (Onyx; eV3 Neurovascular, Irvine, California, USA) have made embolization more effective and more durable. Liquid embolic agents are more likely to be injected directly into the AVM nidus, rather than a proximal pedicle. All three treatment approaches are being utilized to treat specific AVM subsets, supported by a growing body of publications.5–8
Embolization has traditionally been limited to preoperative surgical resection.9 More recently, embolization has been used for preoperative nidus reduction before radiosurgery,10 occasionally as a stand-alone treatment procedure,11–15 and rarely as a palliative procedure to reduce shunting in symptomatic non-ruptured AVMs.16 Throughout the world there is significant literature to support the use of endovascular embolization as stand-alone treatment for AVMs.11 13–15 17–23 However, this is not widely supported in the USA.10 24 25 In this country there has been recent published controversy regarding how angiographically obliterated AVMs should be treated.26 27
There is a clinical decision-making dilemma when an embolized AVM is completely angiographically obliterated. These patients have a risk of recurrence if the lesion is followed expectantly, and they have a risk of complications if the lesion is surgically resected. Therefore the best management is not known. Furthermore, there are no solid data on the hemorrhage risk in an angiographically obliterated AVM. Experience has shown that there seem to be risk factors that make some AVMs more likely to remain occluded while other AVMs are more likely to recur after a previous angiographic obliteration with embolization alone. One of the factors believed to be a cause of AVM occurrence is incomplete embolic nidal opacification which is often caused by proximal pedicle embolization without good penetration into the nidus. For the purposes of this article, nidal opacification refers to filling of the AVM with liquid embolic material and not angiographic contrast. Incomplete nidal opacification (ie, proximal pedicle embolization) can result in the AVM becoming angiographically occult, but the nidus remains patent, and can therefore continue to produce growth factors which can lead to neovascularization and recurrence.28
We present our series of patients in whom complete angiographic obliteration was achieved following embolization. We hypothesized that a subset of patients can be successfully obliterated using stand-alone embolization and that incomplete nidal opacification (proximal pedicle embolization) could lead to recurrence. To the best of our knowledge, there have been no published reports that associate extent of embolization with likelihood of recurrence.
Methods
Approval was obtained from the Vanderbilt University and University of Florida Institutional Review Boards for this study. A prospectively maintained database identified 122 patients who underwent embolization of an intracranial AVM with liquid embolic agents by one surgeon (RAM). Eighteen of 122 (15%) patients achieved angiographic obliteration of the AVM with embolization alone. Seven of these patients were embolized with n-BCA, and 11 were embolized with EVOH to achieve angiographic obliteration. We analyzed the following data on each of these 18 patients: age, sex, presentation, description of AVM, location of AVM, Spetzler–Martin grade,1 number of endovascular embolizations, presence of proximal pedicle embolization, endovascular complications, adverse events, clinical follow-up with modified Rankin Scale (mRS) assessment, duration of clinical follow-up and angiographic/anatomical AVM follow-up with duration. These data are summarized in table 1.
Complete angiographic obliteration of intracranial arteriovenous malformations (AVMs) with endovascular embolization: incomplete nidal opacification is associated with AVM recurrence
Results
Eleven of 18 (61%) patients who underwent complete angiographic embolization were male, at an average age of 45 years. Nine (50%) patients presented with hemorrhage, six (33%) had seizures, one (6%) with a transient ischemic attack (TIA), one (6%) with headaches and one (6%) who had an asymptomatic AVM detected on MRI following trauma. The average Spetzler–Martin grade was 2.5 with a range of grades of 1–4. Of note, one patient had undergone radiosurgery 19 and 13 years previously and multiple embolizations by a different physician 13 years previously. However, these were all unsuccessful and the majority of the AVM was not treated 13 years later when we began embolization alone for the AVM.
An average of 2.5 embolizations per patient was used to achieve angiographic obliteration, with a total of 45 embolization sessions. There were two patients who had proximal pedicle embolization, and therefore the embolic cast had a different morphology than the nidus. The remaining patients had nidal embolization with an embolic cast having similar morphology to the nidus (figures 1 and 2). There was one technical complication (6%) that occurred during embolization which had no clinical sequelae. There was a small amount of extravasation of contrast seen on the angiogram, which was quickly controlled with proximal n-BCA glue and the patient had no change in his neurological examination. There were three postembolization adverse events (16.7%): one patient developed Stevens–Johnson syndrome secondary to Dilantin. Another patient had a prolonged hospitalization secondary to respiratory distress, urinary tract infection and deep venous thrombosis. A final patient developed intraventricular hemorrhage and cerebral edema 2 days after his final embolization for a Spetzler–Martin grade 4 AVM, which achieved angiographic obliteration. He required bilateral ventriculostomies and had a protracted intensive care unit (ICU) stay. The ventriculostomies and ventilator were eventually weaned and he was transferred to rehab. At recent follow-up, the patient was nearly back to neurologic baseline with an mRS of 1 (complaints of mild memory deficit but returned to work, and able to carry out all usual duties).

(A) Digital subtraction angiography (DSA) of Patient 16, lateral view. This image shows the morphology of the arteriovenous malformation (AVM) nidus prior to embolization (circled). (B) DSA of the same patient, same view after angiographic obliteration of the AVM using embolization alone. Note how the embolic cast (circled) has the same morphology as the AVM nidus (A), indicating complete nidal opacification.
{kind=link}
{kind=link}
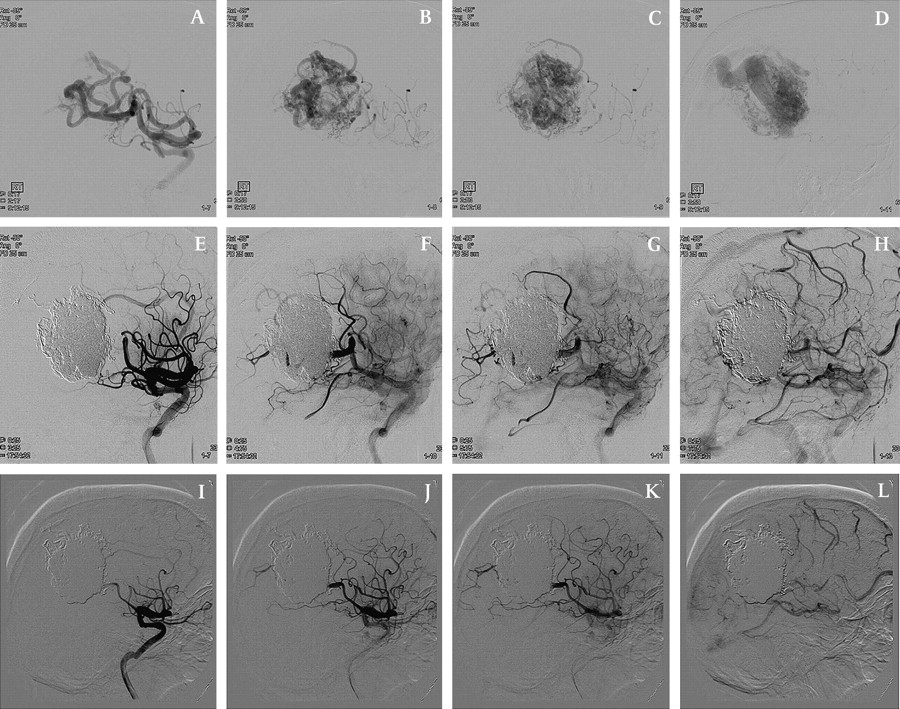
(A–D) Digital subtraction angiography (DSA) of Patient 18, lateral views. Because of the high flow, multiple images are necessary to show all phases of the angiogram. (A) Early arterial phase; (B) mid-arterial phase showing the feeders to the arteriovenous malformation (AVM); (C) late arterial phase showing the AVM nidus; (D) venous phase. (E–H) DSA of the same patient immediately after complete angiographic obliteration of the AVM, in the same angiographic phases as in (A–D). Note that the nidal cast has the same morphology as the AVM nidus. No filling of the AVM nidus is seen. (I–L) DSA of the same patient at 9 months follow-up. There is no AVM nidus or early venous drainage seen in these follow-up angiographic images.
Angiographic follow-up was performed an average of 19 months following complete occlusion in 12 (67%) patients. Three patients (17%) chose craniotomy and surgical resection by one surgeon (RAM) despite complete angiographic obliteration by embolization alone. Resection was performed at an average of 1.5 months following angiographic obliteration. There were no complications during any of the open surgical resections. Careful analysis of the AVMs was performed during resection and there was no evidence of any residual or recurrent blood flow through any AVM nidus during surgical resection. Intraoperative angiography was also performed in all three craniotomies and there was no residual AVM identified. Therefore 15 out of 18 patients had anatomical follow-up confirming no AVM recurrence. The three final patients (17%) refused further follow-up after achieving initial angiographic obliteration. Thirteen patients of the 15 with anatomical follow-up (87%) remained completely obliterated during their follow-up. All 13 of these patients had an embolic cast with morphology similar to the AVM nidus (figures 1 and 2). The remaining two patients (13%) had recurrence of their AVM. Both of the patients with recurrences had incomplete nidal opacification with an embolic cast morphology that was significantly smaller than the nidal morphology. Both patients proceeded to have uncomplicated surgical resection of the recurrent AVM nidus.
Discussion
The complete angiographic obliteration rate from embolization alone in this series is comparable to rates published by other international authors.15 22 It is possible that advances in agents and improvements in other aspects of endovascular treatment might increase the percentage of AVMs amenable to complete endovascular obliteration in the future. It is perhaps more probable, however, that only a fraction of AVMs have the proper mix of anatomy, location, drainage and other factors that make it favorable to complete obliteration with embolization alone.
Some experts argue that embolization cannot provide permanent occlusion, and that attempts to obliterate carry an unacceptably high complication rate.29 With regard to durability, there are two generally accepted reasons why an embolized AVM might not remain permanently occluded. The first is recanalization, which most commonly occurs due to the inherent properties of certain particles, such as polyvinyl alcohol (PVA), to dissipate or flush out of the AVM in to the draining veins over time.30 31 Liquid embolic agents have strong cohesive properties which make them unlikely to dissipate and therefore this type of recanalization is very low with liquid embolic agents.32
The second explanation for AVM recurrence following embolization is neovascularization/recruitment of new feeders by untreated nidus. This can occur after proximal occlusion of an arterial pedicle, leaving portions of the nidus untreated and available to recruit new feeders (neovascularization).28 This can be recognized on fluoroscopic images because the embolic cast is significantly smaller than the morphology of the AVM nidus on angiography. When portions of the nidus remain unembolized, they can form new arterial feeders through neovascularization.28 This idea of proximal occlusion leading to recurrence is supported by our series of patients. Both of the AVM recurrences in our series were in subjects who had portions of the nidus not completely filled with embolic material secondary to proximal pedicle embolization in the absence of deep nidal penetration. Additionally, all of the remaining patients without recurrence had an embolic cast that looked similar in morphology to the nidus, indicating no portions of the nidus were untreated. We believe the best method to predict recurrence after complete angiographic obliteration of an AVM is to draw a perimeter line around the nidus with a dry erase marker and observe opacification of the area inside the perimeter with embolic agent, as previously described.33 This study does not address all of the possible factors leading to angiographic obliteration or recurrence and it is likely that other predictors exist.
In our early experience, after endovascular angiographic obliteration of an AVM, patients were offered one of two possible approaches: first, microsurgical resection with determination of any blood flow in the AVM nidus at the time of surgery or, secondly, a conservative approach with follow-up cerebral angiography at 6, 12 and 24 months. Both of these approaches have been advocated in the literature after achieving angiographic obliteration from embolization.9 15 Two of our patients elected surgical resection and all of the remaining 16 patients elected only follow-up angiography. However, after gaining more experience with complete endovascular angiographic obliteration and determining no blood flow in the angiographically obliterated AVMs, we changed our recommendations. We now only recommend follow-up angiography for all patients. Surgical resection is now only recommended if there has been documented recanalization of the AVM on follow-up angiography.
The incidence and severity of complications from endovascular embolization has decreased over the last 20 years.20 22 23 This evolution is illustrated by Wikholm et al,22 who reported a complication rate, from ‘slight’ to ‘death’ of 52% in cases performed in 1987–88 and a rate of 23% in 1992–93 with no severe complications or deaths. In our current series and others, the complication rate in recent years appears to be even lower.20 23 Mounayer et al20 in 2007 reported a 12% neurologic deficit or death rate in 94 embolizations and Katsiridis et al20 23 in 2008 reported an 11% neurologic deficit or death rate in 219 embolizations while achieving angiographic obliteration of 54% of the patients who have completed their embolizations. In this series, 75% of their patients were high Spetzler–Martin grades (grade 3, 4 or 5).23 These rates compare favorably with the complication rates associated with surgery, described by Spetzler et al1 for grade 3, 4 and 5 AVMs as 16%, 27% and 31%, respectively. In our current series the mortality rate was zero, the adverse event rate was 16.7% (3 out of 18), and two of the three adverse events were not neurological and were unrelated to the AVM.
Some of the limitations of this series are that it represents only a small number of patients mined from a prospectively maintained database, and the length of angiographic follow-up was only 13 months in the patients receiving follow-up angiography. However, it should be noted that persistent angiographic obliteration after 1 year of a previously obliterated AVM would be considered excellent follow-up for a series of patients with either surgical resection or radiosurgery treatment.
Conclusion
We believe that after endovascular embolization of an intracranial AVM, if angiographic obliteration is achieved, one might be able to predict the possibility of recurrence by comparing the embolic cast morphology with the pre-embolization nidus morphology. This preliminary study represents the first publication with evidence of the possible relationship between proximal pedicle embolization and AVM recurrence. Further studies with more patients and longer follow-up intervals will be necessary. In deciding how to treat an individual patient, the neurovascular team must consider size, location and eloquence, as well as age and comorbidities to determine which strategy is the safest and most appropriate.
Key messages
When embolization of an arteriovenous malformation (AVM) results in complete angiographic obliteration, there are limited data describing which AVMs are likely to recur and which ones are cured. We analyzed our database of AVMs that were angiographically obliterated using stand-alone embolization to assess for predictors of recurrence. Proximal pedicle embolization appears to be a predictor of recurrence and when the embolic cast does not match the pre-embolization AVM nidus, recurrence may be more likely.
References
Footnotes
Competing interests The senior author (RAM) performs physician training and physician proctoring for Onyx HD 500, for which he receives compensation from eV3. No other author on this paper has any financial relationship of any sort with eV3 or any other company.
Ethics approval This study was conducted with the approval of the Vanderbilt University IRB.
Provenance and peer review Not commissioned; externally peer reviewed.