Article Text

Abstract
Aim To evaluate the efficacy of vertebral augmentation (VA) in cancer patients.
Materials and methods From a retrospectively compiled database, 147 cancer cases (236 levels) were treated with VA. Mean age was 71±12 years and 56.5% were female. Variables evaluated include age, sex, procedure type, vertebral level treated, number of levels treated per procedure and technical approach. Outcomes were assessed by a previously described method retrospectively applied from medical records: a binary system of ‘responders’ versus ‘non-responders’ and further subcategorization with a four level pain scale. Two patient groups were analyzed: (1) 147 cancer patients with either osteoporotic or malignant vertebral compression fractures (all compression fractures (ACFs)) and (2) 102 cases with documented metastatic compression fractures (MCFs). Univariate and multivariate analyses determined outcomes.
Results 93% of MCFs and 88.5% of ACFs showed response to treatment (pain improvement or resolution): 30% of ACFs and 31% of MCFs experienced pain resolution. MCFs showed increasing age to be a predictor of response to treatment in univariate (OR=1.79, p=0.04) and multivariate (OR=2.05, p=0.03) analysis. In ACFs, bipedicular needle approach decreased the odds of pain resolution (OR=0.28, p=0.01). In MCFs, lung cancer (OR=0.06, p=0.03) and multiple myeloma (OR=0.10, p=0.01) decreased the odds of pain resolution.
Conclusions VA provides pain relief for a majority of ACFs and MCFs. Increasing age may be predictive of pain relief outcomes in MCFs. There are special planning, imaging and technical considerations (eg, needle placement) in using VA to treat cancer patients.
- Metastatic
- intervention
Statistics from Altmetric.com
Introduction
As many as 70% of cancer patients are affected by bone metastases during the course of their illness.1 2 In these patients, malignant bone disease with or without concomitant osteoporosis weakens the structural integrity of the bone and can eventually result in a vertebral compression fracture (VCF).3 Conservative palliative treatment of malignant VCFs includes bed rest, orthotic braces, non-steroidal anti-inflammatory drugs and narcotic medications. These can result in further immobilization which could cause accelerated bone resorption (resulting in an increased risk of a new fracture),4 pneumonia, deep venous thrombosis and decubitus ulcers.5 6 More aggressive management includes chemotherapy (such as bisphosphanates), surgery, external beam radiation therapy, and, recently, percutaneous vertebral augmentation (VA) techniques.7 In patients with malignant spinal compression fractures, VA techniques may be used alone and/or in conjunction with radiation therapy.8
VA techniques such as vertebroplasty and kyphoplasty are minimally invasive procedures that can provide immediate pain relief for patients with VCFs while simultaneously providing bone stabilization.9 Vertebroplasty was initially developed in France in the 1980s to treat vertebral hemangiomas and is now commonly used in the management of osteoporotic, traumatic or neoplastic VCFs.4 9 10 Although small studies have shown that vertebroplasty and kyphoplasty are rapid, safe, durable and effective palliative treatments for metastatic VCFs,5–7 9–12 the literature lacks analyses of a large cohort of patients. We present a single institution experience of 147 cases in cancer patients to demonstrate their efficacy in this particular subset of patients as well as to identify technical and clinical variables that may potentially influence outcomes in this population.
Vertebroplasty involves cannula placement through one or both vertebral pedicles with subsequent injection of polymethylmethacrylate (PMMA) into a compressed vertebral body. The procedure is done using fluoroscopic or CT guided visualization. Kyphoplasty, developed in 1997, is a variant of this technique that involves the creation of a cavity in the vertebral body using an inflatable balloon. The balloon is then removed and PMMA is subsequently injected into the cavity.13 The mechanism of action of VA procedures in pain relief either in cancer patients or in those with osteoporotic compression fractures is unknown and thought to be multifactorial. PMMA stabilizes microfractures and increases the stiffness of the vertebral body.2 9 It is thought that the stabilization of microfractures and reduction of mechanical forces results in analgesia. PMMA is also directly cytotoxic and causes necrosis at the PMMA–tumor interface. It has also been hypothesized that the thermal effects of PMMA polymerization directly coagulates tumor tissue and destroys pain receptors and nerve endings in the affected vertebrae thereby relieving pain.2 9
Methods
Data collection
Using a methodology described previously,11 we compiled a database of 613 cases of vertebroplasty and kyphoplasty performed for compression fractures between May 2003 and March 2008 at our institution. Patients were identified through an electronic database search using the terms ‘kyphoplasty,’ ‘vertebroplasty,’ ‘augmentation’ and various operator's names. We attempted to be as comprehensive and exhaustive as possible to identify the cases treated. Paper records were used to identify additional patients (missed by the electronic searches) between 2006 and 2008. Of the 613 patients, 168 cases had a current and known diagnosis of cancer but no follow-up information was available for 21 of these patients who were therefore excluded from the study. The analysis included the remaining 147 cases (and 236 levels) with a current and known diagnosis of cancer.
Data collection included procedure dates, sex, age at the time of procedure, type of malignancy, fracture etiology, history of cancer treatment (including time and dose of radiation therapy wherever applicable), type of procedure performed (vertebroplasty, kyphoplasty), vertebral level treated (thoracic, lumbar, sacral), the number of levels treated per procedure, the type of approach used (unipedicular vs bipedicular), procedural notes (complications) and follow-up information (dates and pain outcomes).
All data were obtained through electronic medical records. The study was institutional review board approved, and data collection and analyses were conducted in accordance with Health Insurance Portability and Accountability Act guidelines.
Procedures
Experienced staff interventional neuroradiologists at our hospital performed all of the procedures (vertebroplasty and kyphoplasty) using standard methods.12 Procedures were performed with MAC anesthesia or using intravenous conscious sedation. Local anesthesia (1% lidocaine) was used at the access sites of the targeted vertebral pedicles. Needle placement, balloon inflation and cement injections were performed using single plane or biplane fluoroscopy. Vertebral bodies were accessed through a unilateral or bilateral approach. No more than three levels were treated in a single procedure. After each procedure, the needles were removed and direct pressure was applied to the access sites until hemostasis was achieved. Patients were subsequently transported to the post-anesthesia recovery area.
Outcome measures
The primary outcome measure was pain relief experienced after the VA procedure. This information was collected from notes obtained from our institutional electronic medical records. The information was documented either in office visits with a physician/nurse practitioner in the interventional neuroradiology department, the patient's primary care physician, or the patient's oncologist. The time of patient follow-up in relation to the procedure was also noted.
Two separate outcome measures were used. The first was a dichotomized system that categorized patients as ‘responders’ (those who experienced improved or resolved pain after the procedure) versus ‘non responders’ (those who had no change or worsening of pain after the procedure). The second outcome measure built upon the dichotomized system by further quantifying pain using a four level pain scale. This pain scale categorized patients by those who experienced resolution of VCF related pain (level 1), improvement in fracture related pain (level 2), no change in pain (level 3) and worsening of pain (level 4) after the procedure.
Definition of patient groups
Outcomes were measured for two separate patient groups.
The first group consisted of 102 metastatic compression fractures (MCFs) where the fractures were caused by metastases documented by pathology or by imaging.
The second group consisted of all 147 cancer patients with either osteoporotic or malignant VCFs, referred hereafter as ACFs (all compression fractures). ACFs included cases where the cause of the VCF was undetermined—that is, either osteoporotic or pathologic (see figure 1, MCFs are a subset of ACFs). ACFs were included in the analysis in order to assess the results of V and K for compression fractures in cancer patients related to osteoporosis (or other undetermined etiologies, possibly malignant VCFs that were not documented as such).
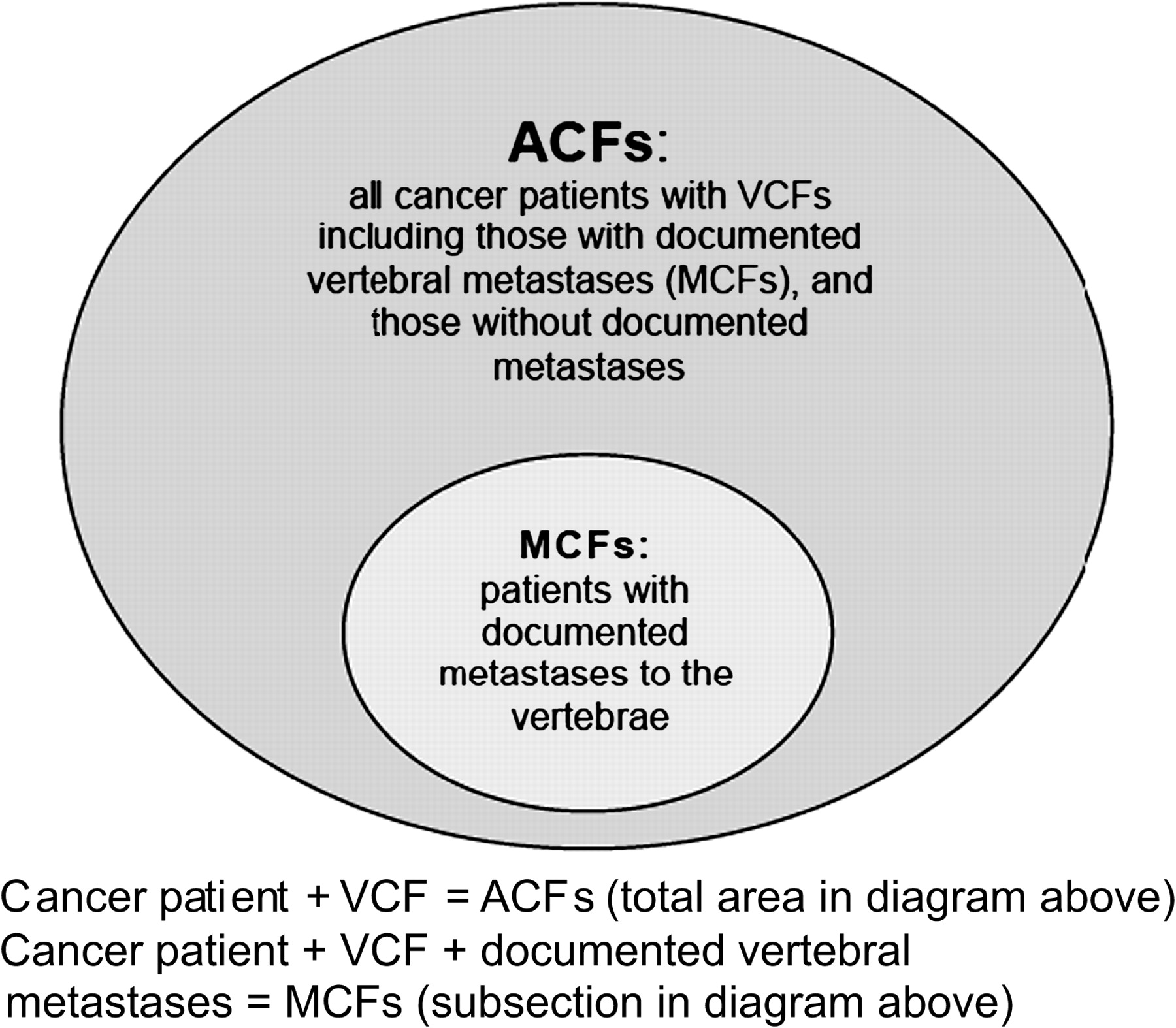
Classification of compression fractures. As shown, metastatic compression fractures (MCFs) are a subsection of the cancer patients with vertebral compression fractures (VCFs) in whom vertebral metastases have been documented. All compression fractures (ACFs) include cancer patients with MCFs as well as those in whom metastases have not been documented. ACFs can therefore be cancer patients who suffer from concurrent osteoporotic disease causing their compression fracture or patients who do have malignant compression fractures that were not documented by pathology/radiology.
Statistical analyses
The variables included in the analysis were the presence of MCFs, gender, age at the time of the procedure, age category by decade, type of cancer, type of procedure performed (vertebroplasty, kyphoplasty, both), vertebral levels treated (thoracic, lumbar, both), number of vertebral bodies treated per case and type of approach (unilateral, bilateral, both).
For both ACFs and MCFs, univariate (binary logit) and multivariate (multiple logistic regression) analyses were conducted. The univariate analyses identified the possible isolated effect of each variable on both outcome measures. Student's non-paired two tailed t tests were used for between group comparisons of continuous data and χ2 tests for comparisons of proportions (eg, proportion of responders in ACFs vs MCFs). The multiple regression model was selected using a forward stepwise procedure with variable entry criterion of p=0.10.
All analyses were conducted using the SAS Statistical System V.9.1 (SAS Institute). Statistical significance in all analyses was determined by p values ≤0.05 and estimates are presented with 95% CI.
General patient characteristics
General patient and procedure characteristics (including age, sex, type of procedure, vertebral region treated, number of levels treated per case and needle placement approach) are presented in table 1.
General patient characteristics
Results
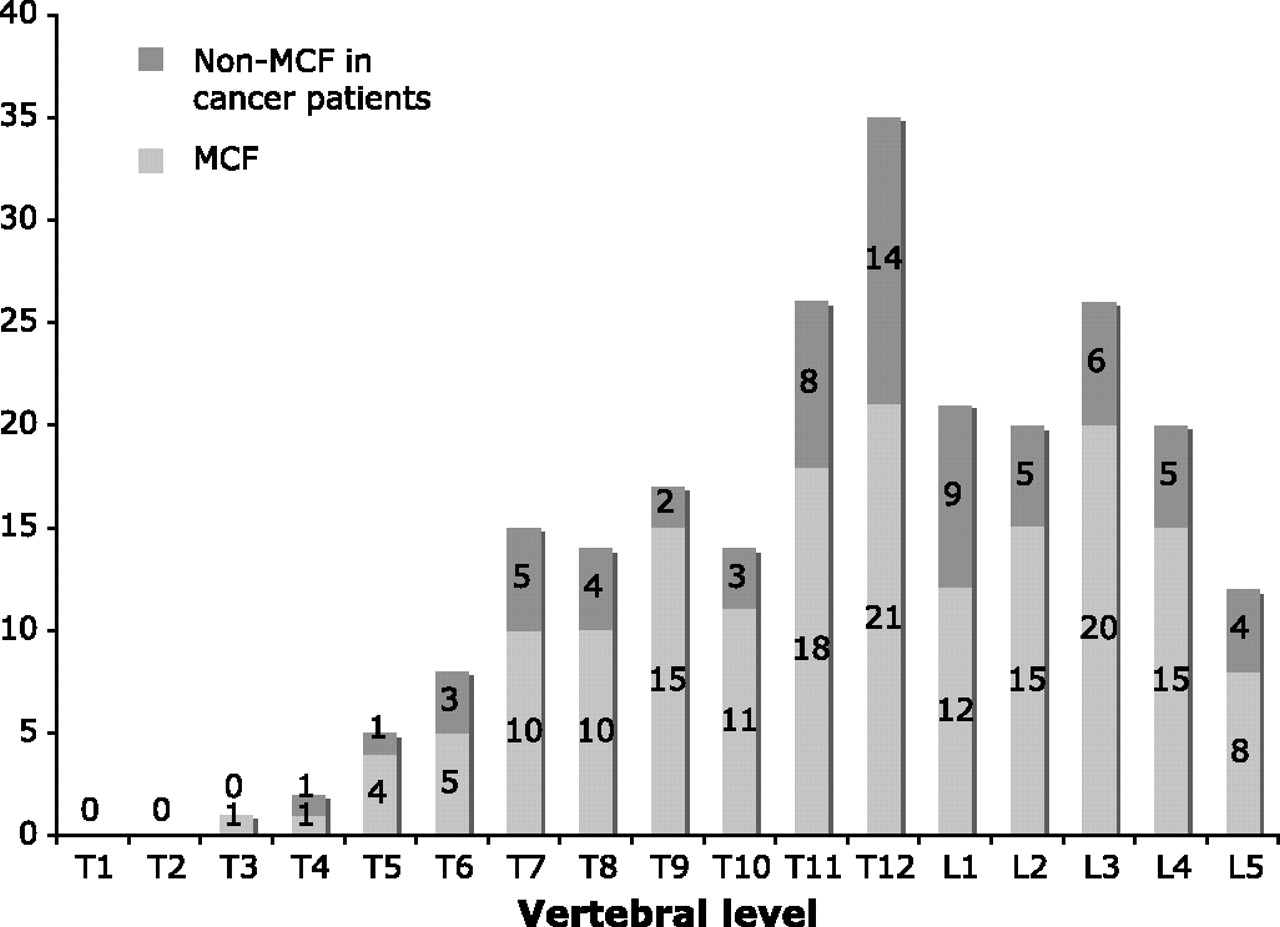
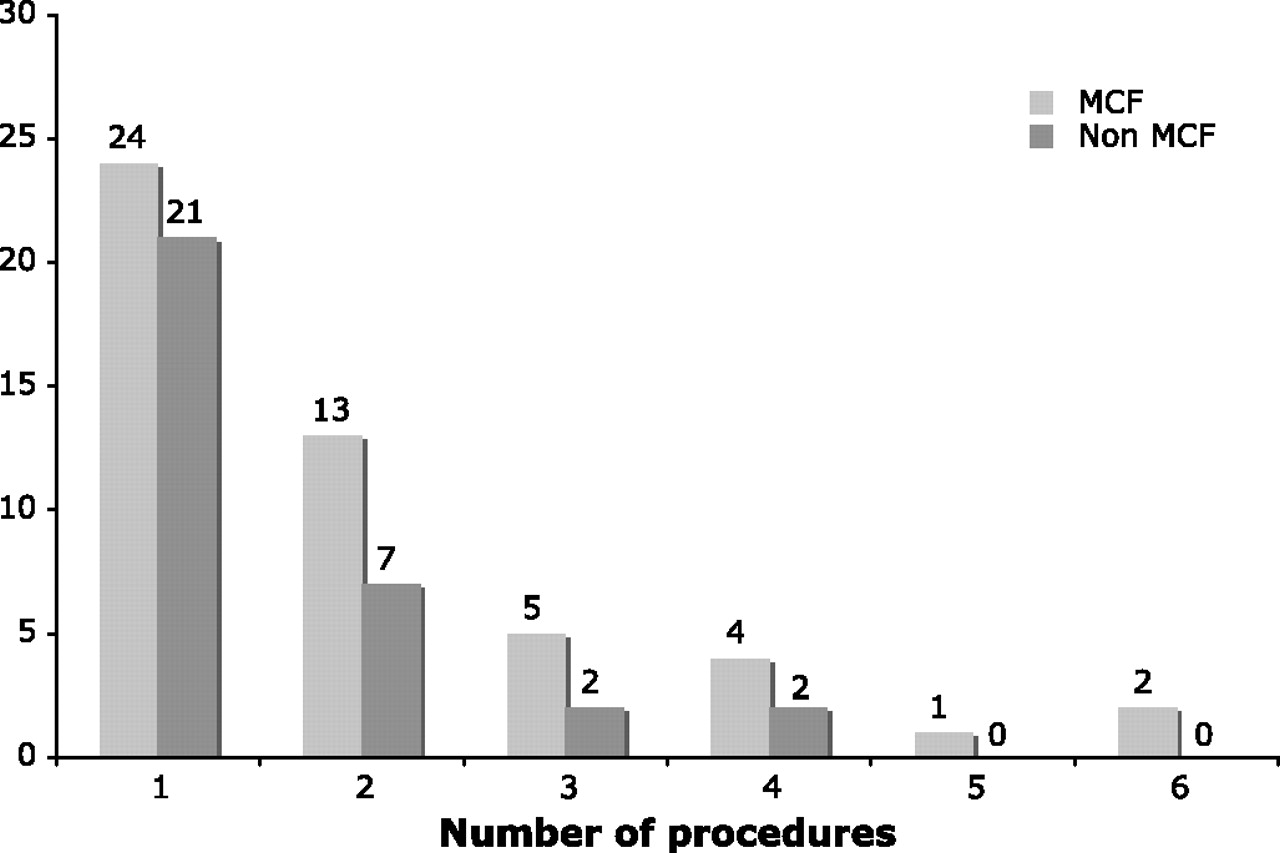
In the 147 cases, a total of 236 vertebral levels were treated with either vertebroplasty or kyphoplasty. Most compression fractures occurred at the thoracolumbar junction, with T11, T12, L1 and L2 accounting for 69.4% of all treated levels (figure 2). The distribution of compression fractures by type of cancer (figure 3) show that 88.2% of documented MCFs and 71% of ACFs had multiple myeloma, breast cancer or lung cancer. Unlike osteoporotic compression fractures, in cancer patients there was a fairly even distribution of ACFs and MCFs between the two sexes (table 1). Patients with documented MCFs tended to have more procedures (average 2.00±1.34) compared with patients who did not have documented MCFs (average 1.53±0.88; p≤0.08) (figure 4). None of the patients required re-treatment of the same vertebral level.

Distribution of fracture by vertebral level showing the breakdown of compression fractures by metastatic compression fractures (MCFs) and non-MCFs in cancer patients treated with vertebral augmentation techniques.
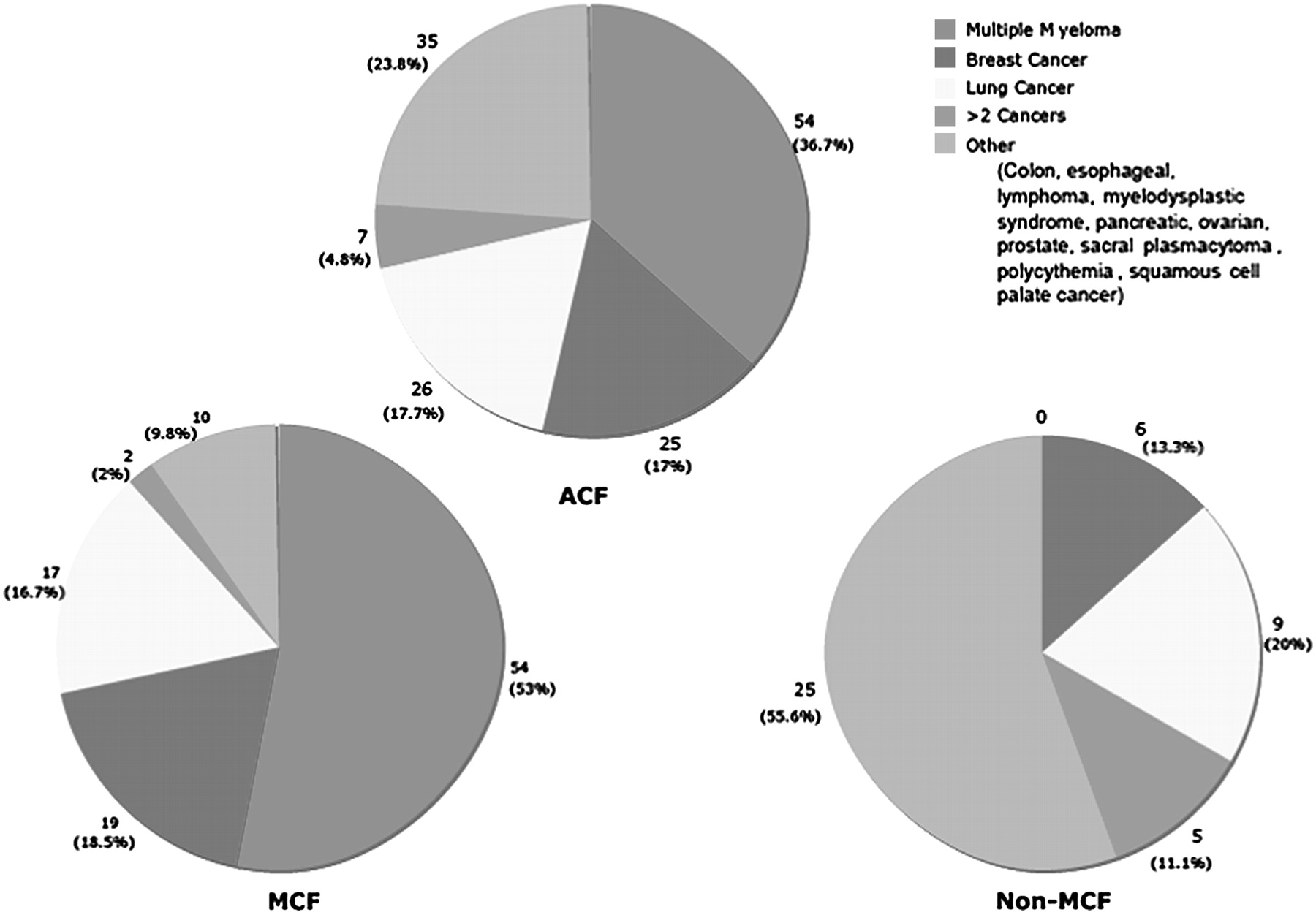
Distribution of compression fractures by type of cancer. The top graph (all compression fractures (ACFs)) shows the distribution of fractures by cancer diagnosis in all cancer patients with the majority of fractures (54) in patients with multiple myeloma. The graph on the bottom left (metastatic compression fractures (MCFs)) shows the same distribution among patients with compression fractures from documented metastases—again, multiple myeloma is the most common diagnosis. The graph on the bottom right (non-MCFs) shows the distribution of cancer diagnoses among patients without documented metastases to the spine—this is the result of all cancer patients minus those with MCFS.
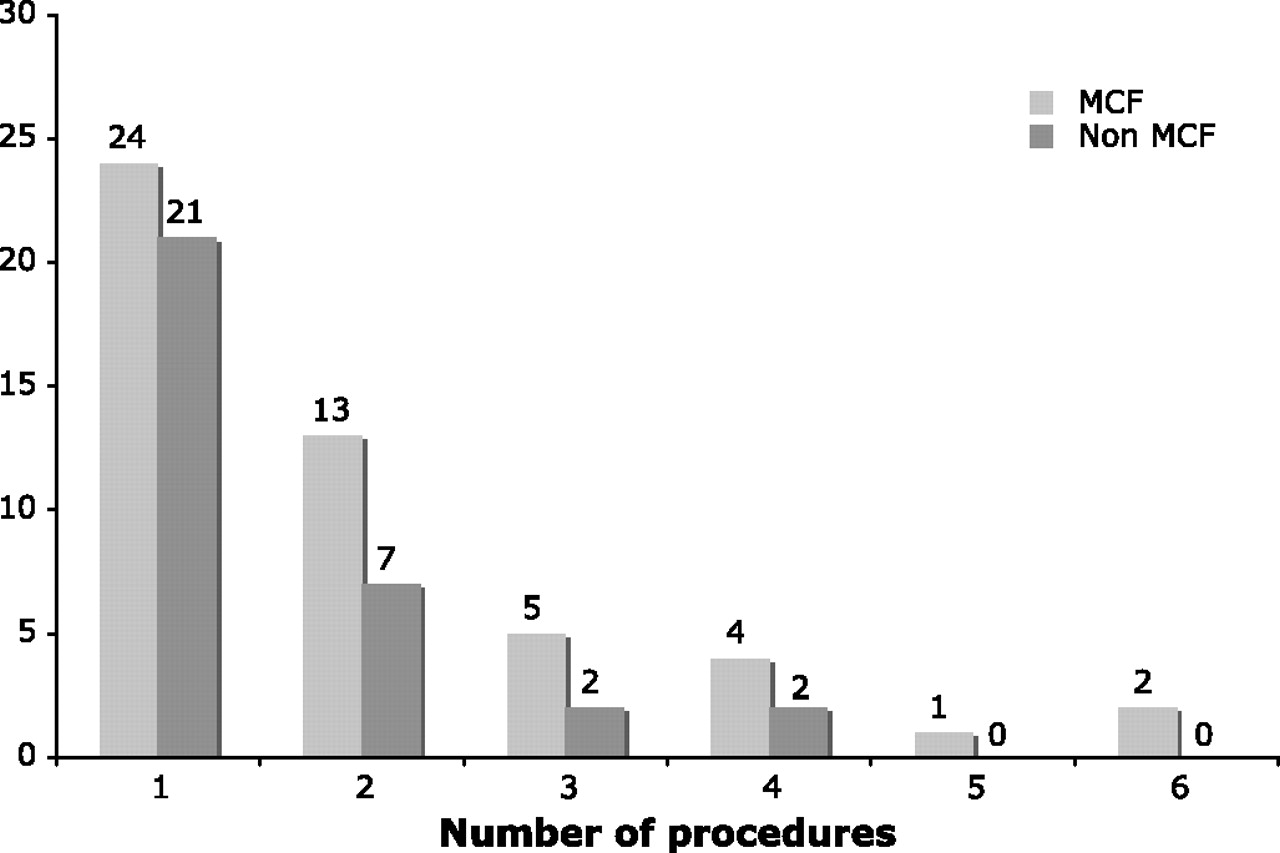
Distribution of the number of procedures in cancer patients for those with metastatic compression fractures (MCFs) and those with non-MCFs.
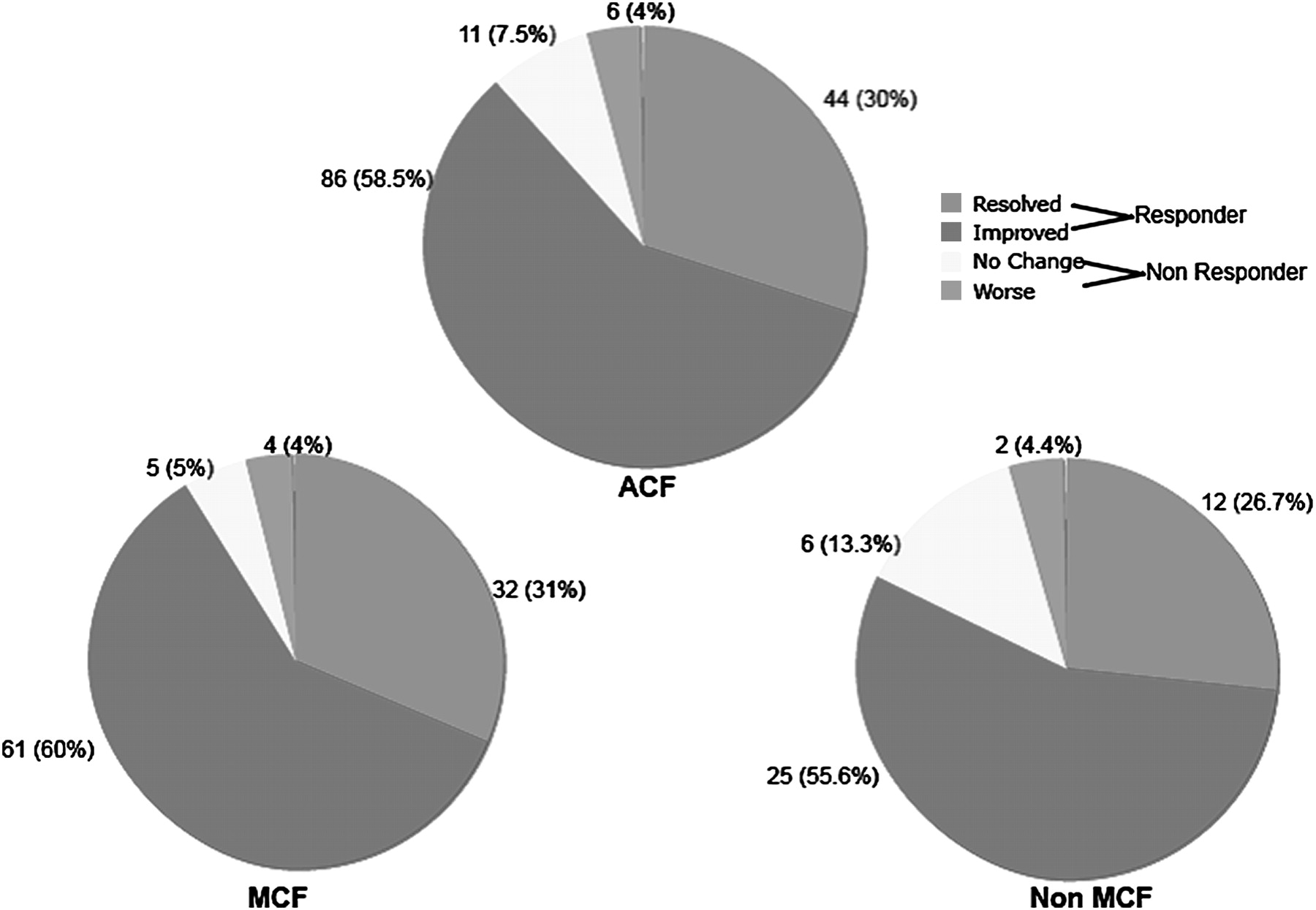
There was virtually no difference in outcomes between patients with ACFs (n=147 cases) and those with documented MCFs (n=102 cases) (figure 5). The majority of patients (93% of MCFs and 88.5% of ACFs) were responders—the difference between the proportion of responders in these two groups was not statistically significant (p≤0.49). The distribution of responders by subgroup analysis is shown in figure 6. Thirty per cent of all cancer patients (ACFs) and 31% of those with MCFs experienced complete pain resolution. Only 4% of patients in both groups reported worsening of their fracture related pain after the procedure. Follow-up time ranged from 1 week to >1 year, with most patients following up within 6 months (table 2).
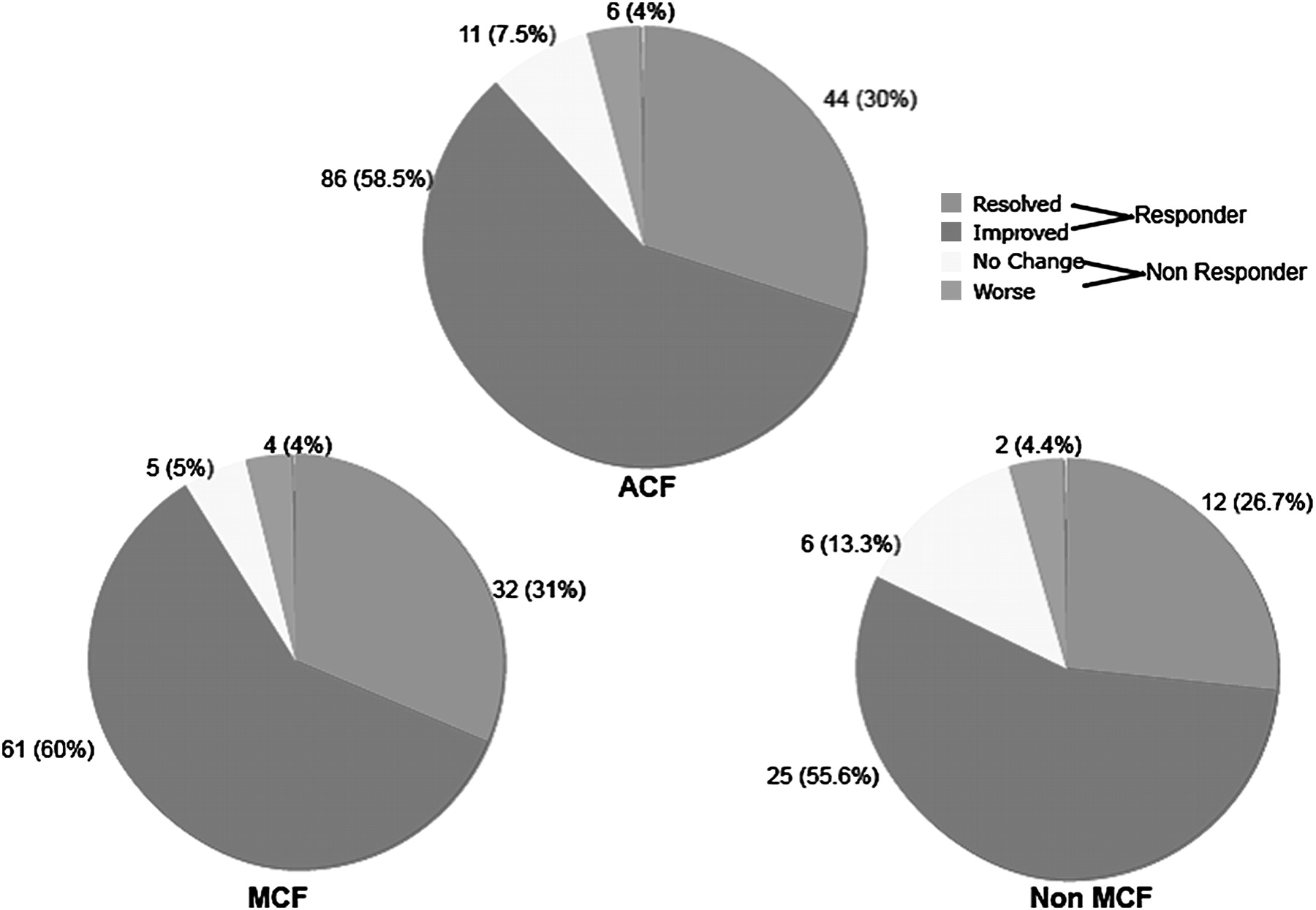
Outcome overview of vertebral augmentation techniques in cancer patients: responders are those patients who report either resolved pain or improved pain. Non-responders are categorized as patients who report no change or worsening pain. The top chart demonstrates outcomes in all cancer patients (all compression fractures (ACFs)), the bottom left chart illustrates the outcomes in those with documented metastatic compression fractures (MCFs) and the bottom right chart shows the outcomes in cancer patients without documented MCFs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of responders in cases of all compression fractures (ACFs) and metastatic compression fractures (MCFs) within each variable. For example, in ACFs within the variable sex, 92.2% of men were responders and 85.5% of females were responders. In MCFs, within the variable sex, 91.5% of men and 90.9% of women were responders. The graph demonstrates that, regardless of the variable subcategory, the majority of the patients were responders to treatment and achieved pain improvement or resolution. BC, breast cancer; Kyp. (K), kyphoplasty; LC, lung cancer; MM, multiple myeloma; O, other; Vert. (V), vertebroplasty.
Pain follow-up timeline
Statistical analyses of responders versus non-responders
To determine whether any of the independent variables were predictive of responders to VA, univariate and multivariate statistical analyses of both groups (ACFs and MCFs) were performed (table 3).
Variables predictive of ‘responders’ to vertebroplasty/kyphoplasty
In patients with MCFs, age was a statistically significant univariate predictor of response to treatment where increasing age resulted in an increased likelihood of being a responder (OR=1.79, p≤0.04). Statistical analyses on the effect of the type of cancer (lung cancer, breast cancer, multiple myeloma and other) could not be performed because there were only two non-responders with a diagnosis of breast cancer and only one non-responder with a diagnosis of lung cancer. None of the other variables (including sex, diagnosis, procedure type, region treated, number of levels treated, needle placement approach or radiation treatment) had a statistically significant affect on the proportion of responders. Similarly, in ACFs, although there was a high proportion of responders within each of the independent variables, none of them was predictive of response (table 3, figure 6).
The stepwise multiple logistic regression model suggested that out of all cancer patients, patients with documented MCFs tended to be more likely to be responders (OR=3.14, p≤0.11). This model also demonstrated that in MCFs, age (p≤0.03) was an independent predictor of dichotomized outcome (ie, responders). No other variables tested provided a statistically significant incremental effect on outcome in either ACFs or MCFs.
Statistical analyses of pain improvement versus pain resolution
Given the small proportion of non-responders (figure 5) among ACFs (11.5%) and MCFs (9%), we further analyzed the responders by categorizing them as patients who experienced complete pain resolution (30% in ACFs, 31% in MCFs) versus those who reported improvement in pain post-procedure but still had residual discomfort (58.5% in ACFs, 60% in MCFs). Univariate and multivariate analyses were performed on both groups (table 4).
Variables predictive of pain scale outcome ‘resolved’ versus ‘improved’
Although not statistically significant, in the univariate model of ACFs, patients with lung cancer (OR=0.18, p≤0.06) and multiple myeloma (OR=0.27, p≤0.08) tended to be less likely to experience complete pain resolution. In patients with MCFs, this outcome was statistically significant where the odds of pain resolution decreased in patients with lung cancer (OR=0.05, p≤0.02) and multiple myeloma (OR=0.16, p≤0.04).
The stepwise multivariate model also identified the type of cancer as a likely predictor of pain resolution versus improvement. Again, although not statistically significant, in ACFs patients with lung cancer (OR=0.18, p≤0.07) and multiple myeloma (OR=0.28, p≤0.09) appeared to have lower odds of pain resolution. In MCFs, this finding was statistically significant where patients with lung cancer (OR=0.06, p≤0.03) and multiple myeloma (OR=0.10, p≤0.01) had decreased odds of pain resolution. This multivariate analysis also reaffirmed that a bilateral needle placement approach in ACFs decreased the odds of pain resolution (OR=0.28, p≤0.01).
Complications
Only one clinically relevant complication was encountered in the 147 cases. Intramedullary balloon ruptures and asymptomatic cement leaks were not considered complications for the purpose of this analysis. We did not review adjacent or other vertebral body fractures in this study.
The clinically relevant complication was procedural, non-fatal and consisted of a laceration of the left-sided L2 lumbar artery in a 57-year-old patient with a spinal meningioma invading the vertebral body. The lacerated segmental artery was observed when bright red blood emerged from the 11 gauge needle while in the parapedicular position. Immediate arteriography confirmed no radiculomedulary or radiculopial supply. The segmental artery was sacrificed and the vertebroplasty was completed. The patient was discharged home and did not require transfusion or any additional therapy.
Discussion
As survivorship among cancer patients is growing,14 therapies directed towards improving quality of life and decreasing pain are becoming increasingly important. Bone pain from metastatic disease is frequent and often debilitating.15 Analgesics, chemotherapy and radiation therapy are different modalities that provide cancer patients relief from this pain but none addresses the underlying mechanical abnormality of the fractured bone. Vertebroplasty and kyphoplasty are emerging interventional techniques that can potentially both effectively address pain as well as stabilize the fracture. They have been deemed safe and durable procedures in appropriate patients 4and have been used individually, and/or in conjunction with local radiation therapy, to treat compression fractures.8 The clinical benefit of VA in cancer patients has led to early reports of treatment outside of the spine with promising results seen in the acetabulum and calcaneus.16 17 Although there is a suggestion that these techniques provide pain relief in cancer patients, the literature currently lacks large analyses of the safety and efficacy of these procedures in this subset of patients.18 19
This study evaluated pain outcomes in patients treated with vertebroplasty and kyphoplasty for VCFs in all cancer patients (ACFs, n=147) as well as in those with documented MCFs (n=102). There was no significant difference in outcomes between these two groups. To our knowledge, this is one of the largest reported series assessing outcomes of VA techniques in cancer patients with vertebral compression fractures. Moreover, this analysis looked at all comers, which included many patients with relative contraindications to therapy or other clinically challenging circumstances. In both MCFs and ACFs, an overwhelming majority of cancer patients (93% and 89% respectively) were responders to VA treatment experiencing either improvement or resolution in their symptoms. Moreover, there was an extremely low complication rate (0.6%) and the type of complication observed here has been described in previous reports.20 Responses to vertebroplasty and kyphoplasty were not analyzed separately because, in a prior analysis (including this patient group), there was no difference in outcomes between the two types of procedures.11
As expected, comparing ACFs with MCFs, there was no significant difference in pain outcomes (in the binary system, as well as within the subgroups of the ‘responders’) based on sex, procedure type (ie, vertebroplasty or kyphoplasty), vertebral region treated or the number of levels treated per case: comparable and large percentages of patients within each of these variables were responders and experienced pain improvement or resolution. Certain patient characteristics influenced pain outcomes in a statistically significant manner. These are described below and include age and needle placement technique.
Both univariate and multivariate analyses revealed that in patients with documented MCFs, older patients had increased odds of being responders. Multivariate analysis indicated that a bipedicular needle placement approach resulted in a statistically significant lower odds of pain resolution in ACFs.21 A bipedicular approach involves cannulation of both pedicles for cement injections whereas a unipedicular technique uses only a single pedicle to inject the PMMA.21 The latter theoretically reduces the risks involved with cannulation by 50%.21 It also potentially reduces procedure time and radiation exposure.21 There have been no randomized trials comparing the efficacy and safety of unipedicular to bipedicular approaches of VA. Cadaveric studies have demonstrated that there is no statistically significant difference in vertebral stiffness between the two groups.22 Cadaveric studies have also shown that a unipedicular approach does not increase the incidence of lateral wedging and provides comparable height restoration of the vertebral bodies.21 In our study there was no difference between ‘responders’ and ‘non-responders’ based on the approach used. However, cancer patients had a statistically significant increased odds of pain resolution with a unipedicular approach. To our knowledge, this is the first report of the improved efficacy of this approach for pain resolution in cancer patients. Recent randomized trials regarding the efficacy of vertebroplasty for osteoporotic compression fractures have reported negative results demonstrating no statistically significant difference in outcomes between vertebroplasty and a controlled intervention suggesting that the benefits of VA may derive from the placebo effect, or at least another mechanism than previously thought.23 24 However it is important to note that these studies are not applicable to cancer patients or malignant compression fractures. Our cohort analysis indicates that VA appears to be an excellent addition to the palliative treatment options as a component of multidisciplinary cancer care.
The type of cancer did not influence whether patients would respond to treatment (table 3, figure 3), but appeared to influence the extent to which patients will respond (ie, with pain improvement versus complete pain resolution) (table 4). The reported incidence of bony metastases in patients with multiple myeloma is 70–95%, 65–75% in patients with breast cancer and 30–40% in patients with lung cancer.15 These three diagnoses constituted the majority of cases (88.2% of MCFs and 71% of ACFs) in our study, and within each cancer diagnosis, greater than 88% of patients reported a positive response to treatment—that is, either pain improvement or pain resolution. However, unlike patients with MCFs from breast cancer, patients with lung cancer or multiple myeloma were less likely to experience complete pain resolution, a finding that was statistically significant. We hypothesize that this may be related to the fact that patients with multiple myeloma and lung cancer are sicker and have an overall worse prognosis25 26 compared with patients with breast cancer or some of the other cancers analyzed in this study. It would be interesting to examine the additional and/or simultaneous effects of the differential use of bisphosphanates and radiation therapy on outcomes of VA in these different types of cancers. The effect of the timing and dose of radiation therapy on outcomes in this patient group was not statistically significant, likely due to the small number of these cases, and this will be further presented and discussed in a separate study.27
As is common with retrospective analyses, our study has several limitations, including observation bias, inability to account for regression to the mean, natural history and placebo effects. It is also important to note that this study did not analyze data regarding use of prescription or over the counter pain medication but this is potentially accounted for in the pain scales used since patients treated at our center and therefore included in this study had insufficient response to conservative medical management before the procedure. Another limitation of this study is that the degree and duration of pain prior to the procedure was not available. It would be interesting to further research whether pain improvement or resolution from the procedures was in the setting of the same number and dose of pain medication, or whether the procedure resulted in a decrease in the number/doses of analgesic therapies; this was not analyzed in the present study. A similar argument applies to the variable follow-up time—in fact, outcomes measured at a longer follow-up time potentially reflect lasting relief from these procedures since prior to the augmentation the patients were unable to experience improvement or resolution of their pain with medical management alone.
Forty-five of the 147 patients did not have definitive histologic diagnosis from the vertebral body and these compression fractures could have been a result of metastatic disease or concomitant osteoporosis and may have been categorized incorrectly. The loss to follow-up of 21 patients, as well as those possibly not included despite our diligent review of the PACS system, could potentially have led to an overestimation of treatment response. The study did not evaluate the effect of pain improvement or resolution on activities of daily living.
Notwithstanding the many limitations we have described above, we believe this retrospective review provides meaningful information from a large experience of cases. This is especially true in light of the paucity of sizeable studies in the literature and the lack of randomized controlled trials. Moreover, this study is a hypothesis generating analysis that identifies important clinical variables (such as type of cancer) that can influence outcomes. Although not a priori determined as outcome predictors, these hypotheses and variables can be specifically addressed in future randomized controlled trials.
Conclusion
This study suggests that vertebroplasty and kyphoplasty provide equivalent, significant, effective and safe pain relief for VCFs in the vast majority of cancer patients with or without documented MCFs. Given the low complication rate and the potential to significantly improve the lives of these patients, we propose that these procedures should be considered as part of the therapeutic armamentarium offered to cancer patients with compression fractures. However, further large studies and randomized controlled trials are required to validate the results of this study before definitive statements can be made about the safety and efficacy of these procedures in relieving pain and improving the quality of life in cancer patients.
Key messages
Vertebral augmentation is primarily used in the USA to treat osteoporotic compression fractures.
The literature more often addresses those cases of osteoporotic fractures and benefits from analyses of a large cancer patient cohorts.
This study is a retrospective analysis of 147 cases, investigating the safety and efficacy of vertebral augmentation in cancer patients. This study describes results in ‘all comers’—that is, all those that were treated. This includes patients with relative contraindications to vertebral augmentation.
In both documented metastatic compression fractures and cancer patients where the underlying fracture etiology is unknown, vertebral augmentation appeared to provide significant pain relief in the vast majority of cases without a significant difference in response related to tumor histology.
We did not observe an increase in local complications that one might expect could have resulted from displacement of tumor mass.
References
Footnotes
See linked article, p 219
Linked articles 002394.
Competing interests JAH is a consultant for and minor shareholder in Cardinal and Medtronic. The authors had complete control of the data and the information in this publication.
Ethics approval This study was conducted with the approval of the institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.