Article Text

Abstract
We present the case of a 47-year-old man with a fusiform aneurysm of the basilar cerebral artery, who was successfully treated with the placement of a novel flow diverter system (Silk stent).
- Stent
Statistics from Altmetric.com
Case report
A 47-year-old man presented chronic posterior headaches and an episode of syncope. Upon admission, the patient appeared alert and oriented and had stable hemodynamic and respiratory parameters. Cerebral angiography (CA) and CT (figure 1), revealed a 30 mm partially thrombosed aneurysm of the basilar artery (BA). Given the lack of adequate circulation, deconstructive treatment options were not considered. For several reasons, including the very small size of the contralateral vertebral artery (VA) and the absence of significant anterior to posterior circulation collaterals, a reconstructive endovascular plan was pursued. Constructive treatment with conventional stent-supported coiling was determined as unlikely to provide durable and complete occlusion of the aneurysm. The use of the Leo Plus stent as scaffolding for the Silk stent was not considered because there are no reliable data to support this practice. For these reasons, parent vessel reconstruction with a flow diversion device (Silk; Balt Extrusion, Montmorency, France) was pursued. The patient was premedicated with an antiplatelet regimen using 75 mg of clopidogrel and 100 mg of acetylsalicylic acid (ASA) for 8 days before the procedure.
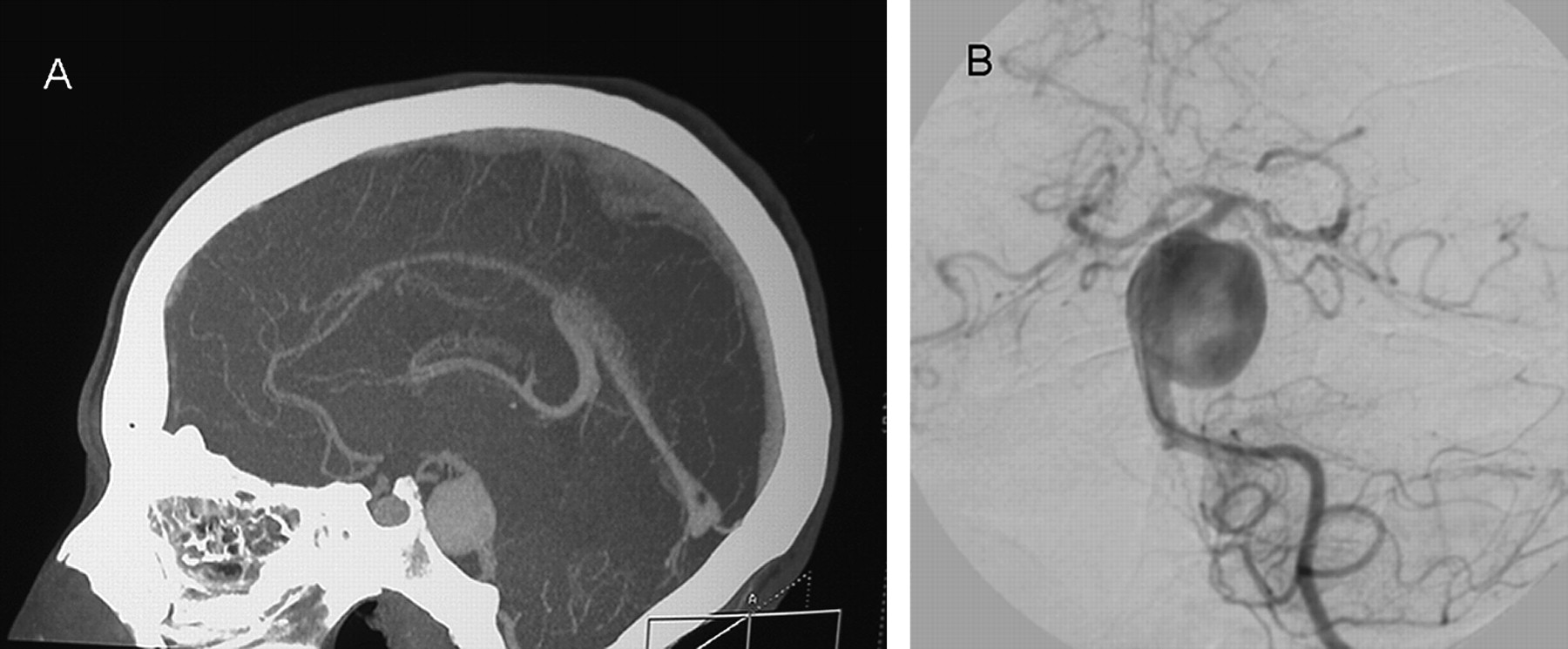
Pretreatment imaging. Conventional subtracted angiographic image in posteroanterior projection (A) and sagittal reconstruction of aCT angiogram (B) showing a fusiform aneurysm from the basilar trunk.
The Silk has been designed to hemodynamically exclude the aneurysms from the parent artery and to provide sufficient scaffolding to support neointimal repaving of the neck defect. The Silk has a high-density braiding technology with 48 wires that allow excellent wall apposition and conformability, four helicoidal radio-opaque markers on the whole length allowing better control of the deployment and flared ends to avoid the ‘Tulip’ effect and better wall apposition in tight curves. The stent is repositionable up to 90% deployed and is available in diameters ranging from 2.5 to 5 mm and from 12 to 75 mm lengths. The interstices between the strands are designed to allow enough flow to maintain the patency of large branch vessels as well as small perforators (figure 2).
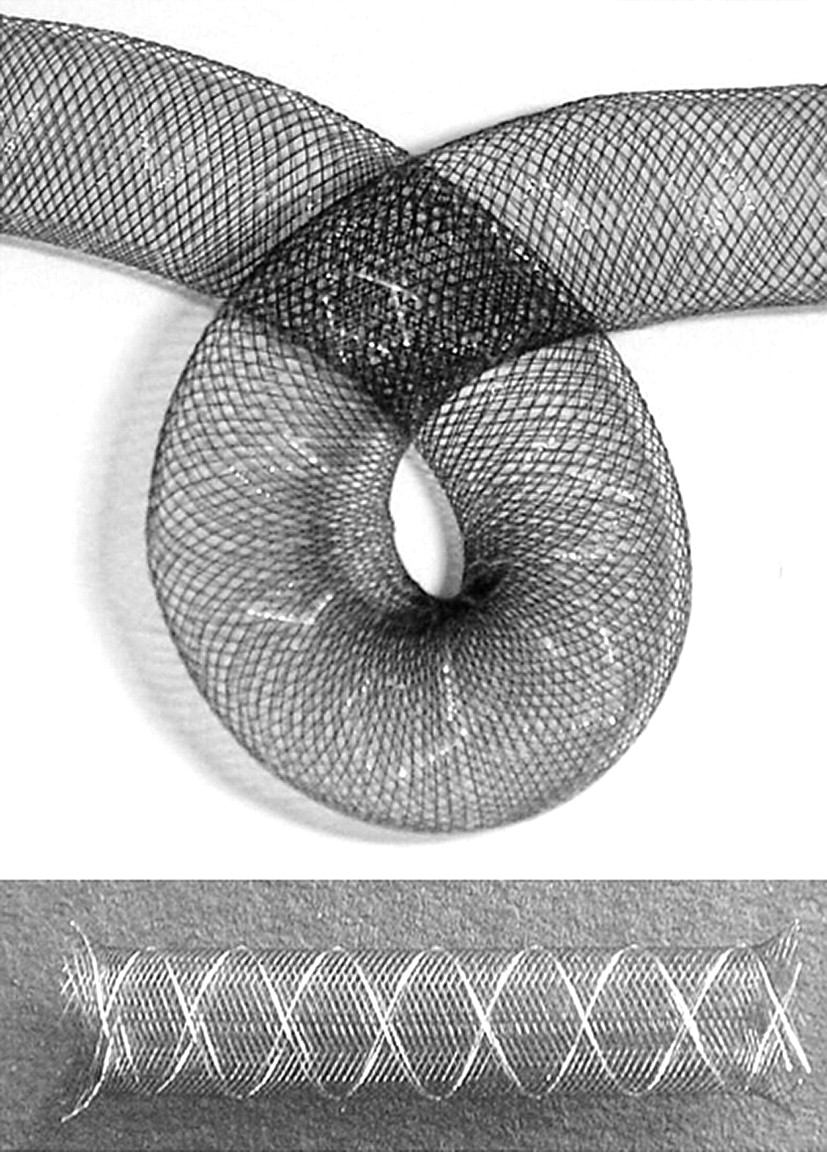
Schematic image of the SILK with a conglomerate structure composed of 48 wires of nitinol with four helicoidal radio-opaque markers on the whole length and flared ends.
The stenting technique performed was similar to that previously described for Leo stents (Balt, Montmorency, France).1 The treatment was performed under general anesthesia using intravenous heparinization after placing a 6F sheath into the femoral artery to reach an activated clotting time of between 250 and 350 s. A guiding catheter (Envoy 6F; Cordis Endovascular, Miami Lakes, Florida, USA) was passed smoothly into the left VA, a microguidewire (Terumo 16) and a microcatheter Vasco Plus 21 (Balt, Montmorency, France) were coaxially advanced into the target vessel to provide sufficient support for stent placement. After retrieval of the microguidewire, using a road-mapping technique, a 4.5×40-mm Silk stent was advanced into the Vasco and deployed carefully across the aneurysm extending from the proximal BA to just below the origins of the superior cerebellar arteries (SCAs), to reconstruct the parent artery. Immediate angiogram showed significant flow reduction into the aneurysm and residual filling in the remaining aneurysm (figure 3). There were no immediate complications and the patient was maintained on a low dose of intravenously administered heparin (300 U/h) for 24 h after the procedure. One week later the patient was discharged, completely asymptomatic, with clopidogrel 75 mg/day and acetylsalicylic acid 100 mg/day for 3 months.

Immediate post-treatment imaging. Digital subtraction angiography in posteroanterior projection showing anatomic reconstruction of the basilar artery after SILK deployment
Follow-up digital angiography and CT angiogram (figure 4) performed at 6 months revealed stable anatomic reconstruction of the parent vessel with slight dilatation of the distal BA without involvement of the SCAs or residual filling of the aneurysm. The mass effect from the aneurysm was largely resolved and the patient showed complete resolution of his symptoms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up imaging at 6 months. Frontal view angiogram (A) andfrontal (B) and lateral (C) reconstructions of a CT angiogram showing stable anatomic reconstruction of the parent vessel with no residual filling of the aneurysm.
Discussion
Fusiform intracranial aneurysms are defined as a circumferential dilatation of a cerebral artery without any ostium or neck representing <1% of all intracranial aneurysms and they are commonly located on the supraclinoidal internal carotid artery (ICA), the VA or the BA.2 Fusiform aneurysms of the BA are among the most difficult to treat, and the ideal treatment modality is complete occlusion of the aneurysm and preservation of the parent artery. Until recently, the only definitive treatment was the complete trapping by endovascular coiling or surgical clipping, presenting high rates of periprocedural morbidity and mortality. Recently, new techniques and materials have widened the range of aneurysms susceptible to endovascular treatment. Stent technology has improved with the introduction of self-expanding stents (Neuroform; Boston Scientific, Natick, Massachusetts, USA; Enterprise; Cordis Neurovascular, Warren, New Jersey, USA; LEO and LEO Plus; Balt Extrusion, Montmorency, France) and new devices designed to allow enough flow through the construct to maintain the patency of large branch vessels as well as small perforators arising along the course of the parent vessels bearing the aneurysm. Recognition of the potential for aneurysm treatment by flow diversion is evidenced by the recent development of two devices: Pipeline Neuroendovascular Device (PED; Chestnut Medical Technologies, Inc., Menlo Park, California, USA) and Silk (Balt, Montmorency, France). These flow diversion systems have low porosity and high pore-density values and represent an important advance of the endovascular remodeling strategy for aneurysm treatment by promoting intra-aneurysmal thrombosis while maintaining patency of the parent vessel and side branches.3–7 Although they are two similar systems, the Silk system differs from the Pipeline system in that it is composed of nitinol and has more variety of lengths facilitating not having to put telescoping stents. In the present case, a 47-year-old man with a fusiform aneurysm of the BA was successfully treated with the placement of a Silk stent. To our knowledge, although there are two previous reports,6 7 this is the first fusiform basilar aneurysm successfully treated using the placement of a neurovascular dedicated stent.
The Silk system appears to represent an optimal treatment modality of complex, wide-necked and fusiform/dissecting aneurysms with promising preliminary results. Although longer follow-up and expanded clinical trials are needed in order to assess whether it is a definitive treatment, whether there is long-term risk of recurrence and what is the effect on vessel patency after placement of the Silk device.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.