Article Text

Abstract
Purpose To assess the long-term safety and clinical effectiveness of inferior vena cava (IVC) filters in patients with stroke.
Method and materials In this institutional review board-approved, Health Insurance Portability and Accountability Act-compliant retrospective study, we reviewed the clinical data of patients who had stroke and were treated with an IVC filter from 2002 to 2009. The demographics, clinical data, indications for IVC filter, procedural complications, symptomatic post-filter pulmonary embolism (PE) and deep vein thrombosis (DVT), caval occlusion and incidental, imaging-evident filter-related complications were recorded. Safety was assessed through occurrence of filter-related complications during placement and follow-up. Effectiveness was assessed through occurrence of post-filter fatal and non-fatal PE.
Results During this period, 371 patients (224 male; mean age 67.5 years) with stroke received an IVC filter. The stroke was hemorrhagic in 28%, ischemic in 20%, associated with intracranial malignancy in 21% and trauma in 31%. 235 (63%) patients (PE in 159) had venous thromboembolism on imaging. The indications for IVC filter included contraindication to anticoagulation in 251 (68%), prophylaxis in 83 (22%), added protection in 22 (6%) and complication or failure of anticoagulation in 15 (4%). There was one procedural complication. During a follow-up of 1.74±2.36 years, 180 (49%) patients died, three due to post-filter PE and the remainder all due to primary disease. Symptomatic post-filter PE and DVT occurred at a frequency of 15% (54/371) and 16% (60/371), respectively. Of these, 15 (4%) had imaging-proven PE. Three (0.8%) succumbed to post-filter PE. Imaging-proven new or recurrent DVT occurred in 6% and 8%, respectively. Symptomatic caval occlusion was seen in five (5/371, 1.3%).
Conclusion IVC filters have an acceptable safety profile in stroke patients. In our cohort, they were effective in preventing life-threatening PE.
- Deep venous thrombosis
- intervention
- pulmonary embolism
- stroke
- vena cava filters
- vein
- venous thromboembolism
Statistics from Altmetric.com
- Deep venous thrombosis
- intervention
- pulmonary embolism
- stroke
- vena cava filters
- vein
- venous thromboembolism
Introduction
Stroke remains the third leading cause of death in the United States.1 In patients with fatal cerebral infarcts (ie, those who died within 30 days of initial event), non-neurological conditions such as cardiac, pulmonary and infectious processes contribute to death in a substantial number of patients. This is especially true if the patient has survived for >8 days after the onset of stroke.2 In addition, stroke and its ravages such as paraparesis and immobility put the patient at high risk of symptomatic or asymptomatic deep venous thrombosis (DVT) and pulmonary embolism (PE).3 The risk of fatal PE is 4.9-fold higher in immobilized patients following neurological disease.3 The corrected rate of fatal PE among patients with ischemic stroke ranged from 1.5% to 2.1% in a 19-year study period that analyzed deaths from the United States Bureau of the Census Compressed Mortality File.4 Recurrent venous thromboembolism (VTE) is also more common in patients with limb paresis following stroke.5 The risk is even higher in patients with brain tumors presenting as stroke.6
Anticoagulation with heparin, low molecular weight heparin or warfarin is the treatment of choice for VTE; however, it may not be acceptable in many patients with stroke due to the risk of spontaneous intra-cerebral hemorrhage. Therapy with intermediate doses of unfractionated heparin was associated with death and recurrent stroke in 0.5% of participants in the International Stroke Trial.7 The risk of major hemorrhage in stroke patients treated with warfarin for 3 months was 1%.7 As such, these patients are often treated with inferior vena cava (IVC) filters for preventing PE. The published reports on the effectiveness and safety of IVC filters are limited to specific designs or involved the general population with various risk factors.8–11 The safety and effectiveness of IVC filters in patients with stroke is not well known. Thus, the purpose of our study is to assess the safety, effectiveness and long-term morbidity of IVC filters in patients with stroke.
Materials and methods
This retrospective study was approved by our Institutional Review Board and the requirement to obtain informed consent from the study subjects was waived. This study complies with the Health Insurance Portability and Accountability Act.
Study design
The study subjects were identified through the Research Protocol Database Registry and a list of patients who had stroke and had an IVC filter between 2002 and 2009 was retrieved. The clinical and imaging data of the patients were reviewed from electronic medical records and from picture archiving and communication systems. The demographics, clinical and imaging data, indications for IVC filter, procedural complications, symptomatic post-filter PE, post-filter DVT, symptomatic caval occlusion and incidental, imaging-evident filter-related complications were entered into a database (Filemaker Pro 10.0; Filemaker, Santa Clara, California, USA). We used the reporting standards for IVC filter placement published by the SIR.12
Patients
During the 8-year period, 371 patients with stroke received an IVC filter. There were 224 male (60%) and 147 female (40%) patients. The age of the patients at the time of filter implantation ranged from 20 to 105 years, with a mean of 67.5 years, median of 69.6 years (men: 20–105 years, mean 65, median 66.8; women: 24–101 years, mean 72, median 76.5).
Diagnosis of stroke
The diagnosis of stroke was suspected clinically and confirmed using cross-sectional imaging in all patients using standard institutional protocols. The pathophysiology for stroke was intracranial hemorrhage in 105 (105/371, 28%), ischemia in 73 (73/371, 20%), intracranial malignancy in 77 (77/371, 21%) and cranial trauma in 116 (116/371, 31%).
Thromboembolic events and diagnosis of thromboembolism
Thromboembolic events
One hundred and eighty-five (185/371, 50%) patients presented with symptoms of PE. All these patients underwent imaging studies at our hospital and were available for review. Fourteen of these patients (14/185) also had symptoms of DVT. Seven additional patients had chest CT for suspected pulmonary process (other than PE) and six were found to have asymptomatic PE. In addition, 10 patients had symptoms of PE at an outside hospital before presenting to our hospital. The imaging data were not available for review, but the medical records documented the presence of PE in all 10 patients on imaging studies performed elsewhere.
Seventy (70/371, 19%) patients presented with symptoms of DVT. The symptoms included leg swelling and pain in the calf. Fourteen of these patients also had symptoms of PE. In addition, 197 (197/371) patients had imaging studies for detection of DVT either as part of evaluation for PE or as routine studies for detection of asymptomatic DVT. Of these 197 patients, 83 had DVT on imaging studies. In addition, 13 patients had symptoms of DVT at an outside hospital and imaging confirmed the presence of DVT in all. The imaging records were not available for review.
Overall, 264 (264/371, 71%) had symptoms of VTE. Among these, 181 patients had symptoms of PE, 14 had symptoms of PE and DVT, and 69 patients had symptoms of DVT only.
In addition, 53 patients had prior history of VTE, but no acute VTE at the time of filter request.
Diagnosis of PE
Imaging studies were available for review in 185 patients (all patients with symptoms of PE). CT pulmonary angiography (CTPA) was performed in 148 (148/185, 80%) patients, pulmonary angiogram in 17 (17/185, 9%), ventilation-perfusion scintigraphy (V/Q scan) in 10 (10/185, 5%) and CT chest in 9 (9/185, 5%). In one patient (1/185, 1%), trans-thoracic echogram was performed. PE was confirmed on imaging studies in 143 (143/185, 77%) patients. As explained earlier, seven patients had chest CT for other pulmonary processes and six were found to have PE. Ten additional patients had symptomatic, imaging-proven PE at an outside hospital before presenting to our hospital. Thus, the total number of patients who had imaging-evident, symptomatic or asymptomatic PE was 159 (159/371, 43%).
Diagnosis of DVT
Imaging studies for detection of DVT were available for review for 267 (267/371, 72%) patients (70 symptomatic and 197 asymptomatic). CT venography (CTV) of the thighs and pelvis was performed in 135 (135/267, 51%), compression ultrasound (CUS) of the thighs in 129 (48%) and MR venography of the pelvis in 3 (3/267, 1%). DVT was seen on imaging in 141 (141/267, 53%). In addition, 13 patients had imaging studies performed at an outside hospital and were found to have DVT. Thus, the total number of patients who had imaging-evident symptomatic or asymptomatic DVT was 154 (154/371, 42%).
Indications for filter placement
Contraindication to anticoagulation constituted the major indication for filter placement in our group. Two hundred and fifty-one patients (251/371, 68%) had a contraindication to anticoagulation (table 1). In 83 (83/371, 22%) patients, filters were placed as a prophylaxis against PE. In 22 (22/371, 6%) patients, filters were implanted as an additional protective measure against PE despite receiving full-dose anticoagulation. Nine patients (9/371, 2%) received filters because they developed complications following anticoagulation. Six patients (6/371, 2%) developed recurrent VTE despite anticoagulation and then received an IVC filter.
Results
Technical data
Filter implantation
Filter implantation was performed under fluoroscopy (n=356) or intravascular ultrasound (IVUS) guidance (n=15) by board-certified interventional radiologists. IVUS-guided filter placement occurred in patients who could not be mobilized to the fluoroscopy suite. The filters deployed under IVUS include TrapEase (Cordis Endovascular, Warren, New Jersey, USA) (n=4), OptEase (Cordis Endovascular) (n=3), Celect (Cook Medical, Bloomington, Illinois, USA) (n=3), Gunther Tulip (Cook Medical) (n=4) and Recovery (Bard Peripheral, Tempe, Arizona, USA) (n=1).
Venous access was obtained through the femoral, jugular or a peripheral vein. Cavography was performed prior to filter deployment under fluoroscopy. Filters were deployed per the manufacturer's guidelines. Following filter placement, patients were observed for access site complications. The observation period ranged from 4 h for femoral venous puncture to 2 h for jugular and brachial venous puncture.
Venous access was obtained through the femoral vein (n=355, 95.6%), the jugular vein (n=14, 3.7%) or the brachial vein (n=2, 0.5%). Cavography demonstrated thrombus in the IVC in six (1.6%). Narrowing of the cava was seen in two patients—extrinsic compression of the IVC due to right hydronephrosis in one and concentric stenosis of the IVC at the location of a previous filter in one. Filters were deployed in the infrarenal position in 365 (98.4%) patients and in the suprarenal position in six (1.6%). The types of filter used in our patient cohort are as follows: TrapEase in 252, OptEase in 41, Recovery in 38, Gunther Tulip in 18, Vena Tech (Braun, Bethlehem, Philadelphia, USA) in 8, Simon-Nitinol (Bard Peripheral) in 6, Celect in 5, Greenfield (Boston Scientific, Natick, Massachusetts, USA) in 1, Bird's Nest (Cook Medical) in 1 and in 1 patient the name of the filter was not specified.
Filter retrieval
A lower extremity venous duplex study always preceded the first attempt at retrieval. Retrieval of the filter was performed if there was no DVT. Cavography was performed and if there was no thrombus in the filter, the retrieval procedure was continued. The filter hook was snared with a loop snare and the filter was retrieved per the manufacturer's guidelines. Post-retrieval angiography of the IVC was performed.
The filter was retrieved in 12 patients, through the jugular (n=10, four Celect filters, five Recovery filters, one Gunther Tulip) or femoral (n=2, both OptEase filters) approach.
Follow-up
Clinical and imaging follow-up data were recorded whenever available. The occurrence of symptomatic caval thrombosis, DVT and PE after filter placement was recorded. Whenever there was clinical suspicion of post-filter PE/DVT, the imaging data were reviewed. Abdominal CT performed for any reason during follow-up was reviewed for asymptomatic filter-related complications such as filter fracture, filter migration, penetration of the vena cava wall by the filter, thrombus in the filter and thrombus in the IVC. If a thrombus in the filter or IVC was detected, the medical records were reviewed for any related symptoms.
End points
The safety of the filter was assessed by calculating the frequency of symptomatic and asymptomatic filter-related complications (such as access site complications, procedure-related complications, filter migration, filter fracture and filter thrombosis) during placement, retrieval and follow-up. The effectiveness was assessed through occurrence of post-filter fatal and non-fatal PE. The median survival of patients following filter placement in this patient population was assessed through Kaplan–Meier curves.
Results
Clinical follow-up
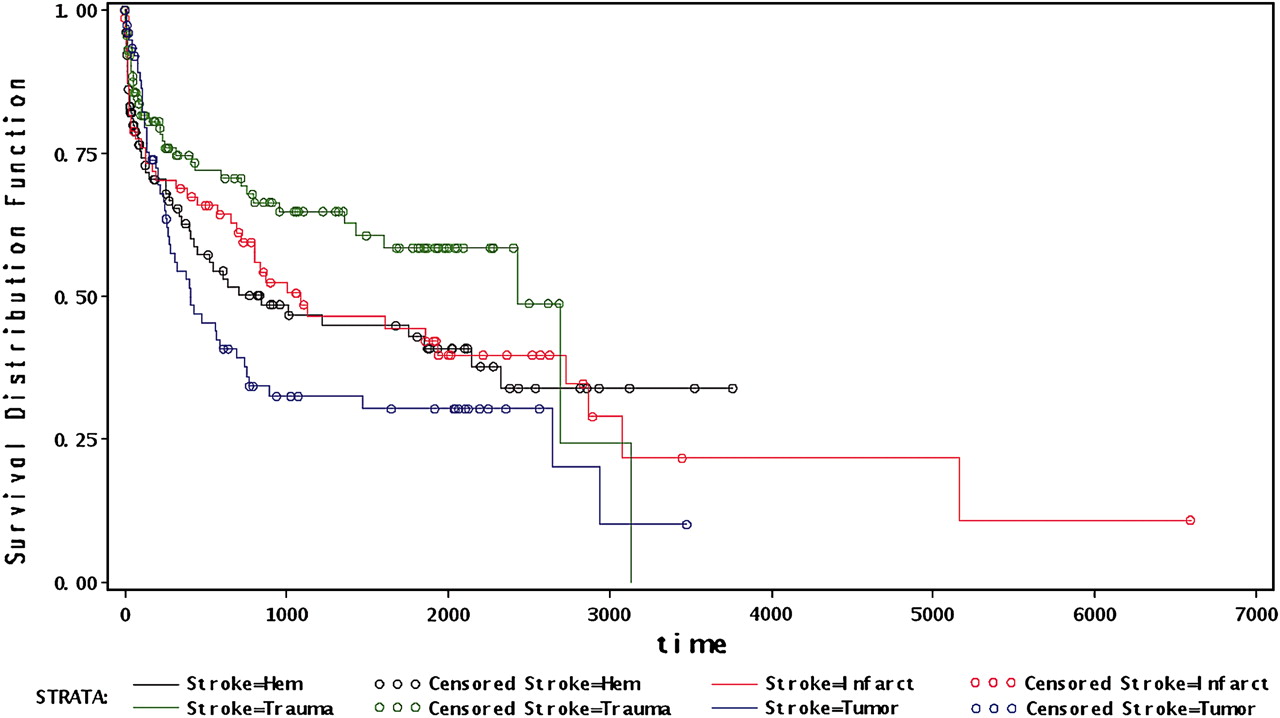
Clinical follow-up was available in all patients and ranged from 1 month to 10.2 years with a mean of 1.74±2.36 and a median of 0.4 years. During this period, 180 (180/371, 49%) patients died. The median survival following filter placement was as follows: 1.1 years for patients with intracranial malignancy, 2.3 years for patients with hemorrhagic stroke, 2.9 years for patients with ischemic stroke and 6.6 years for patients with trauma (figure 1).
{kind=link}
Kaplan–Meier curves for probability of survival following filter placement in patients with stroke.
Procedural complications
There was one complication during deployment—one filter was accidentally deployed in the right gonadal vein. Another filter was deployed in the infrarenal cava in the same patient. There were no access site complications. One retrieval procedure was complicated by requirement of femoral cut-down to remove the filter, as the filter could not be engaged in to the femoral sheath during the retrieval process.
Anticoagulation during follow-up
Eighty-two (82/371, 22%) patients received anticoagulation (low molecular weight heparin followed by warfarin) following filter placement. Sixteen of these received aspirin in addition to anticoagulation. In addition, 57 patients received aspirin alone. Among the 82 who received anticoagulation, one patient had post-filter PE and eight, post-filter new DVT. Five patients had non-occlusive thrombus in the filter and 10, IVC thrombosis.
Post-filter PE
Fifty-four (54/371, 15%) patients developed symptoms of PE following filter placement after a mean 1.5±22.8 months (median 0.68, range 0.1–69 months). All patients underwent imaging for confirmation of PE (tables 1 and 2). Imaging confirmed the presence of PE in 14 (14/54, 26%). Thirteen additional patients with no symptoms of PE underwent CT for suspected lung disease. One patient (1/13) had PE on CT. Thus, symptomatic or asymptomatic, imaging-confirmed PE occurred at a frequency of 4% (15/371). PE was fatal in three of the symptomatic patients. Thus, post-filter fatal PE occurred in 1% (3/371) of our group.
Post-filter complications
Post-filter DVT
Sixty patients (60/371, 16%) presented with symptoms of DVT following filter placement (table 1). Imaging (CTV in 4, CUS in 56) was performed in all 60 patients. Twenty-nine (29/60) patients had DVT on imaging. Ninety additional patients underwent surveillance imaging for detection of DVT (CTV in 47, CUS in 43) and imaging revealed DVT in 22 (22/90). In total, post-filter, imaging-confirmed DVT occurred in 51 (51/371, 14%) patients. Of these, 21 had new DVT, and 30, recurrent DVT. Symptomatic caval occlusion was seen in five (5/371, 1.3%). The symptoms of caval occlusion occurred after a mean period of 33 months following filter placement in these patients.
Imaging with CT abdomen
One hundred and seventy-two (172/371, 46%) patients had CT abdomen after a mean period of 8.1±18.7 months (median 0.63, range: 0.03–96.2 months). Thrombosis of the cava was seen in 25 patients (25/172, 15%) (table 3). Of these 25 patients, two had symptoms of caval occlusion. In addition, 26 (26/172, 15%) patients had non-occlusive thrombus in the filter. Significant filter migration was seen in two patients: one cranial migration to the suprarenal IVC and one caudal migration to iliac vein confluence. Fracture of filter components was seen in six (6/172) patients. Penetration of caval wall by the filter legs was observed in seven (7/172).
Filter complications on CT abdomen (n=172)
Discussion
Stroke is a leading cause of severe and long-term disability.1 While at times inevitable, complications due to pneumonia, DVT, PE and urinary tract infection portend poor quality of stroke care.13 Studies indicate that half of all patients admitted to hospital for an acute stroke develop DVT and more than a quarter of them may then go on to develop PE.7 14 Half of clinically evident PEs after stroke present as sudden death and most of these patients may not have clinical evidence of DVT.15 Clinical factors independently associated with an increased risk of fatal PE were immobilization for neurological disease (4.9-fold higher), age >75 years (2.54-fold higher) and cancer (2.04-fold higher).3 Recurrent VTE is also more common in patients with limb paresis following stroke.5
Incidence of DVT after stroke exceeds that following surgery and is equivalent to that after hip or knee arthroplasty; however, thromboprophylaxis in stroke patients is less effective compared with those with hip fractures.7 Intermittent pneumatic compression devices for prevention of DVT are effective after stroke, but they are not well tolerated by this group of patients.7 Regular, extensive use of thromboprophylaxis with anticoagulants can prevent 50% of PEs and 66% of DVTs in stroke patients.16–18 Despite thromboprophylaxis, PE still accounts for one-eighth to one-quarter of early deaths after stroke.7 Moreover, in the International Stroke Trial,7 intermediate-dose unfractioned heparin was associated with a 0.5% risk of death and recurrent stroke, and a 1.5% risk of non-fatal extracranial bleeding. Risk of major hemorrhage in stroke patients treated with warfarin for 3 months was 1%.7 Schulman et al19 noted major bleeding in 8.6% of stroke patients on indefinite warfarin, after 4 years of follow-up.
Given the high incidence of VTE and risks of thromboprophylaxis, high-risk stroke patients may benefit from aggressive therapeutic strategies, such as vena cava filter insertion.3 Published reports on the effectiveness and safety of IVC filters are limited to specific designs or involved the general population with various risk factors. In a randomized controlled study of patients with DVT, IVC filters reduced the short-term risk of PE, but were also associated with long-term risk of recurrent DVT.20 Streiff et al21 concluded that symptomatic post-filter PE occurred in 2.6%–3.8% of patients during a mean follow-up of 6–18 months. In a 26-year single-center study, post-filter fatal and non-fatal PE occurred at a frequency of 3.7% and 5.6%, respectively, during a mean follow-up period of 16 months.8 Post-filter fatal PE occurred in 0.8% of patients in our study. Reported fatal PE in stroke patients ranged from 1.5% to 2.1%.4 Compared with the historical incidence of PE in stroke patients, there was a moderate reduction in the incidence of fatal PE in our group. Additionally, post-filter non-fatal PE occurred in 4%, which is comparable to other published data on the effectiveness of filters, suggesting similar effectiveness of IVC filters in stroke patients.8 22
In our study, there were minimal procedural or access site complications. Symptomatic caval thrombosis was seen in 1.3%. However, asymptomatic caval thrombosis on CT was seen in 13%. Filter migration was noted in 1.2%. These are comparable to published data on the safety of IVC filters among patients with various risk factors.21 23 Thus, our study demonstrates that stroke patients who receive an IVC filter are not at higher risk of symptomatic caval thrombosis compared with patients with other risk factors.
An increasing trend of prophylactic filter placement was observed by Athanasoulis et al, in a study that encompassed 26 years: 4.7% during the initial years and 16.4% during the final years of their study.8 In our study, 22% of filters were placed for prophylactic reasons, which may reflect increased awareness of the availability of filters and increased interest in preventive measures to improve the outcome of stroke patients. Similarly, a trend towards new retrievable filters is also observed in other studies.24 The role of retrievable filters in stroke patients is not known. In our study, 49% of patients died within a mean period of 1.35 years following stroke. Many patients who survived continue to be at high risk for DVT. Among the patients who received retrievable filters, only 14% of the filters were retrieved. This suggests that the role of retrievable filters in this population might be limited.
The main limitations of our study are its retrospective nature, lack of a control group and lack of imaging follow-up in all patients. However, our study provided long-term clinical follow-up and data on asymptomatic and symptomatic complications.
In conclusion, this study demonstrates an acceptable safety profile of IVC filters in patients with stroke. In our cohort, they were highly effective in reducing fatal pulmonary embolism.
Key messages
Half of the hospital admissions for stroke develop deep vein thrombosis and more than a quarter of them progress to pulmonary enbolism (PE).
Despite thromboprophylaxis, PE still accounts for one-eighth to one-quarter of early deaths after stroke.
Given the risks of thromboprophylaxis, high-risk stroke patients may benefit from aggressive therapeutic strategies, such as vena cava filter insertion.
Inferior vena cava filters have an acceptable safety profile and are effective in reducing fatal PE in patients with stroke.
References
Footnotes
Funding JAH is a shareholder in Intratech.
Competing interests SPK has conflict of interest with Angiodynamics.
Ethics approval This study was conducted with the approval of the Institutional Review Board of Massachusetts General Hospital.
Provenance and peer review Not commissioned; internally peer reviewed.