Article Text

Abstract
Objective To evaluate the rate of peri-procedural thromboembolic events after the endovascular treatment of cerebral aneurysms. The rate of diffusion-positive lesions was assessed in relation to selected procedural and technical factors.
Methods 184 patients treated with coil embolization (198 total procedures) between July 2004 and February 2007 were included. In 65, the procedure was coiling alone; in 55, coiling with balloon remodeling; in 48, coiling with Neuroform stenting; and in 30, coiling, Neuroform stenting and balloon remodeling. All patients underwent a routine diffusion weighted magnetic resonance imaging (DWI) within the 72 h after the intervention for the detection of ischemic complications.
Results Regardless of the technique used, thromboembolic complications were more common (p<0.0001) in patients with ruptured aneurysms (33/65, 51%) than in those with unruptured aneurysms (40/133, 30%). Balloon remodeling tended to be associated with a lower rate of DWI positivity than the other techniques. Younger patients (≤60) with unruptured aneurysms had the lowest rates of DWI lesions regardless of the technique used.
Conclusion In this study, peri-procedural DWI-positive lesions occurred in approximately one-third of all cases. These were threefold more common in the setting of ruptured aneurysms. Adjunctive devices did not increase the rate of ischemic events. On the contrary, there was a trend toward fewer DWI abnormalities in the procedures in which balloon remodeling was employed. This may, in part, be related to the application of the conglomerate coil mass technique of balloon remodeling.
- Balloon
- stent
- emboli
- aneurysm
- embolization
- aneurysm
Statistics from Altmetric.com
Introduction
With the advent of diffusion weighted imaging (DWI), there is increasing evidence that endovascular procedures for the treatment of intracranial aneurysms can be associated with peri-procedural cerebrovascular ischemic events.1 Intravascular stent support and balloon remodeling are two widely accepted techniques that are used to assist embolization of complex aneurysms not amenable to simple (unassisted) coiling.2 Some have hypothesized that these adjunctive techniques result in an increased incidence of ischemic complications.
We present a retrospective assessment of the rate of peri-procedural diffusion lesions in patients who underwent aneurysm embolization with, or without, balloon and/or stent assistance. Additional variables considered included aneurysm status (ruptured vs unruptured), patient age, and the aneurysm location (anterior vs posterior). Our analysis indicated that adjunctive devices did not increase the rate of ischemic events. On the contrary, a trend towards lower DWI abnormalities was seen in the procedures in which balloon remodeling was employed. This may be related to our novel technique of balloon remodeling.
Patients and methods
Patients
The study involved 198 procedures in a group of 184 patients treated with coil embolization between July 2004 and February 2007.
In 65 of the procedures, patients had presented with subarachnoid hemorrhage (SAH) due to acute aneurysmal rupture. Forty-six of the patients in this group were women, and the mean age was 52. Heparin use was recorded in 34 of the procedures. The techniques used for coiling were stent-assisted in 2, balloon-assisted in 39, and coiling alone in 24.
One hundred thirty-three procedures were done in patients with unruptured aneurysms, 108 of whom were women. The mean age was 56. Patients were pretreated with either aspirin or clopidogrel in 90 cases. Heparin was used in all procedures in this group. The techniques used for coiling were stent-assisted in 46, balloon-assisted in 16, stent and balloon-assisted in 30, and without assistance in 41 procedures.
All data were retrospectively reviewed using inpatient clinical charts, and institutional review board approval was obtained.
Procedure
All procedures were performed by four experienced neurointerventionalists (DF, HHW, TJM, PAR) with the patients under general anesthesia. Stent assistance, balloon remodeling, or both, were used as an adjunctive technique in a group of patients based on the location, configuration, and status (ruptured vs unruptured) of the aneurysms.
Antiplatelet therapy was typically instituted in patients whom we expected would need stent reconstruction. Aspirin and/or clopidogrel were typically used at doses of 325 mg and 75 mg, respectively, starting at least 5 days before the procedure or after an initial clopidogrel loading dose of 300–600 mg. Response to the antiplatelet therapy was routinely verified using aggregometry. When platelet suppression was insufficient, a loading dose of 325–650 mg (aspirin) and 300–600 mg (Plavix) was given before the procedure, or the procedure was delayed pending alteration of the regimen and retesting showing adequate antiplatelet activity. Heparin was administered in IV boluses during the procedure. An ACT value >250 s was considered therapeutic.
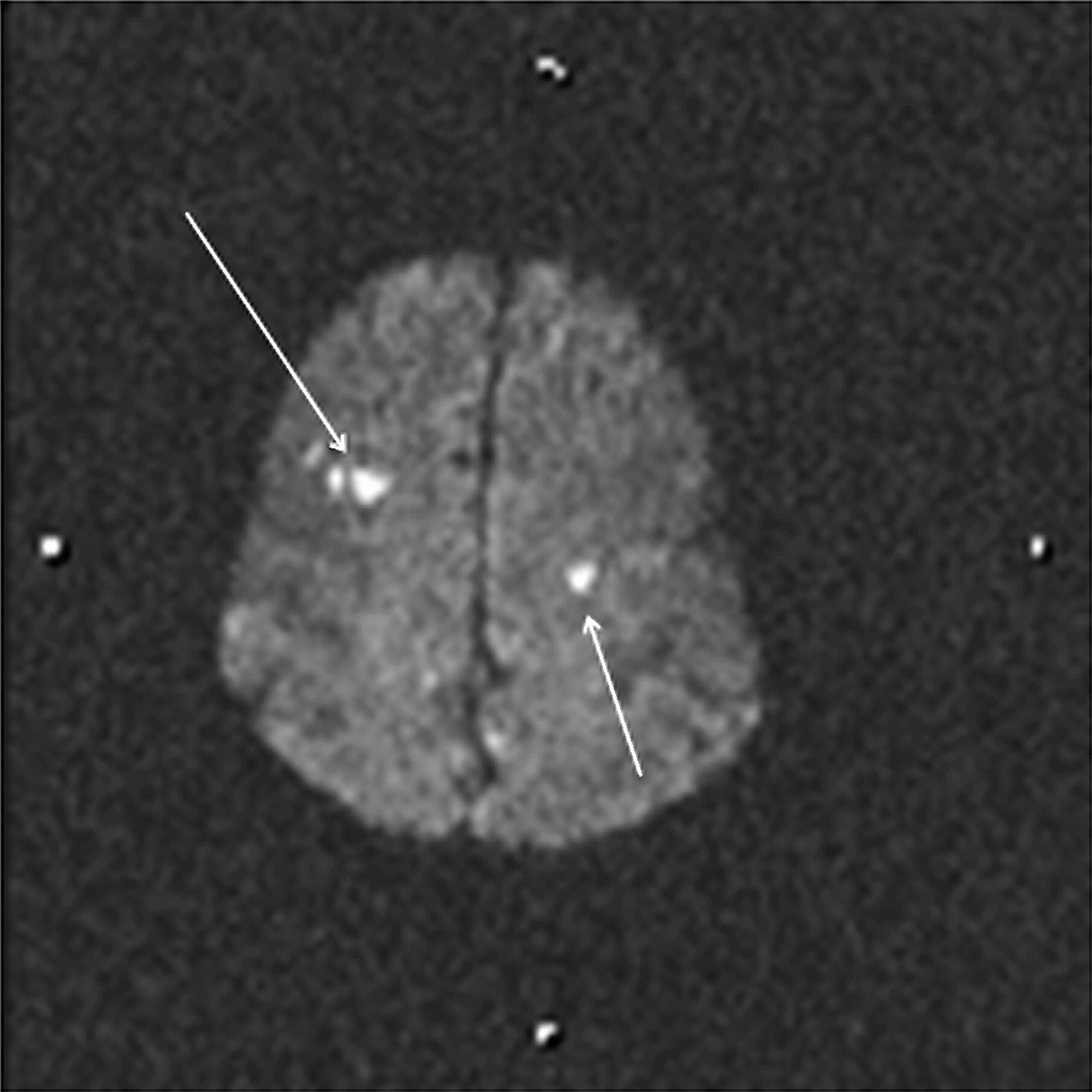
The patients had DWI MRI within the 72 h post-procedure as a routine protocol for the detection of procedure-related ischemic complications. The imaging was performed on a 1.5 T MR imaging system (Siemens Medical, Forcheim, Germany). Any area of restricted diffusion, regardless of size or clinical presentation (from a punctate hyperintensity to a confluent infarction) was considered a positive result (figure 1).
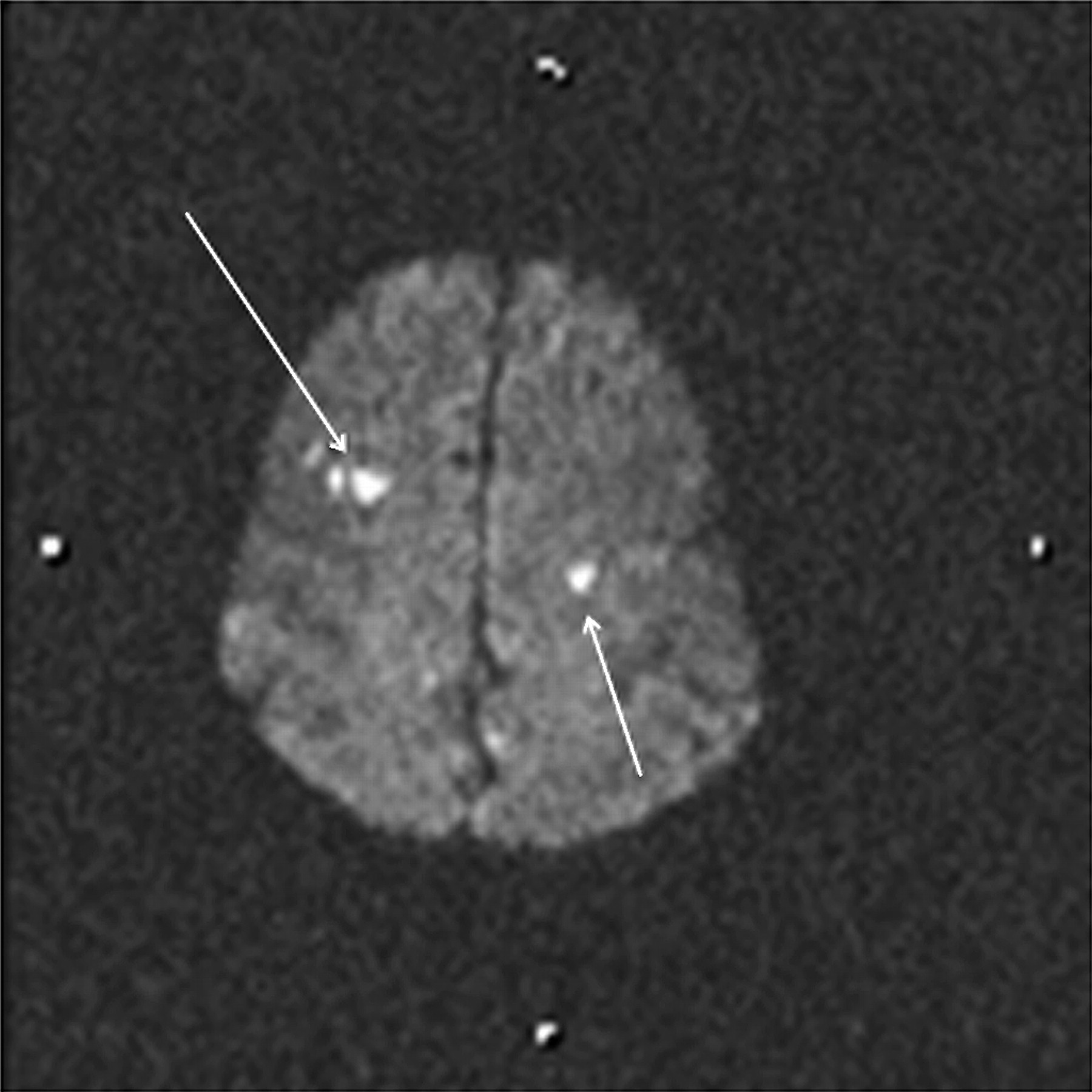
Hyperintense lesions on diffusion weighted magnetic resonance imaging representing thromboembolic events in a 40-year-old patient with ruptured anterior communicating artery aneurysm who had coil embolization (arrows).
Statistical methods
Two-way Fisher's exact test and logistic regression analysis were used for all comparisons. A p value <0.05 was considered statistically significant.
Results
The aneurysms treated were located in the internal carotid artery (n=93), middle cerebral artery (n=6), anterior communicating artery (n=46), basilar artery (n=47), posterior inferior cerebellar artery (n=3), posterior cerebral artery (n=2), and vertebral artery (n=1).
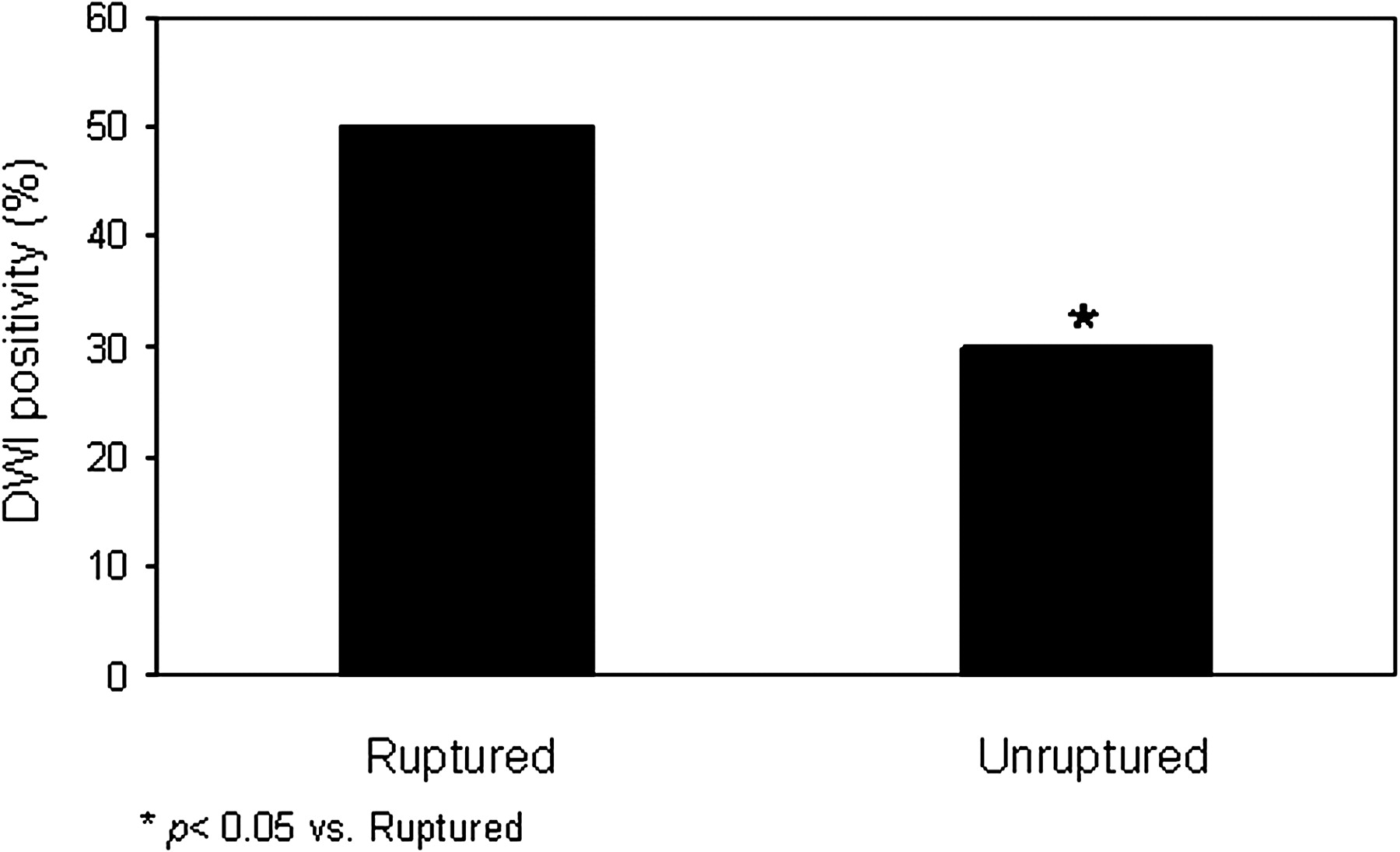
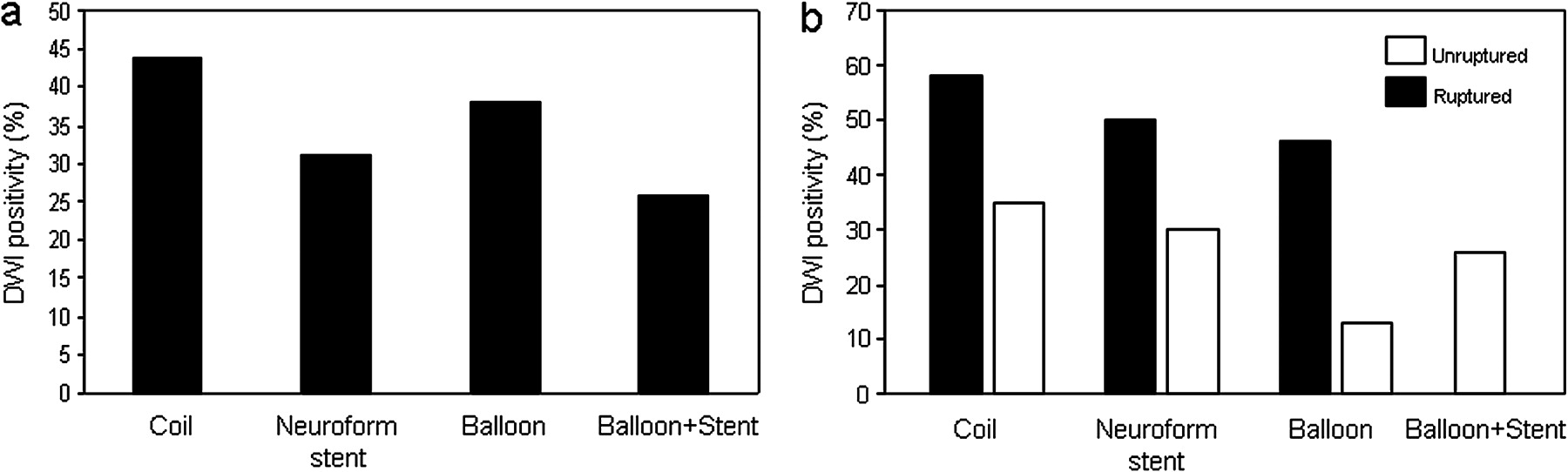
Clinically evident events were rare and seen in three (5%) patients treated with coiling only, one (2%) patient with assisted coiling, four (7%) with balloon remodeling, and one (3%) with both stenting and balloon remodeling. Overall, the rate of DWI abnormality between groups of each procedure type was not significant (figure 2). However, DWI lesions were detected in 51% (n=33) of the procedures performed on patients with ruptured aneurysms, versus only 30% (n=40) of the procedures performed in patients with unruptured aneurysms (figure 2). This was statistically significant (p=0.019).

Histogram demonstrating the percentage of diffusion weighted magnetic resonance imaging (DWI) lesions in patients with ruptured versus unruptured aneurysms after endovascular procedures. Patients with ruptured aneurysms were associated with higher rate of thromboembolic events.
In the unruptured aneurysm group, DWI demonstrated areas of restricted diffusion in 30% (n=14) of the procedures with Neuroform stenting, 13% (n=3) with balloon remodeling, and 26% (n=8) with both techniques. When no adjunctive technique was used, 35% (n=14) of the coiling procedures had a DWI lesions.
In the patients with ruptured aneurysms, the DWI abnormality rate was 46% (n=18) and 58% (n=14) in the procedures with balloon remodeling, or with no assisting technique, respectively. Stent assistance was used in two patients, one of whom had a DWI abnormality.
There was no statistical significance between the groups undergoing different procedures in either aneurysm status (figure 3), which was not surprising given the small sample size.
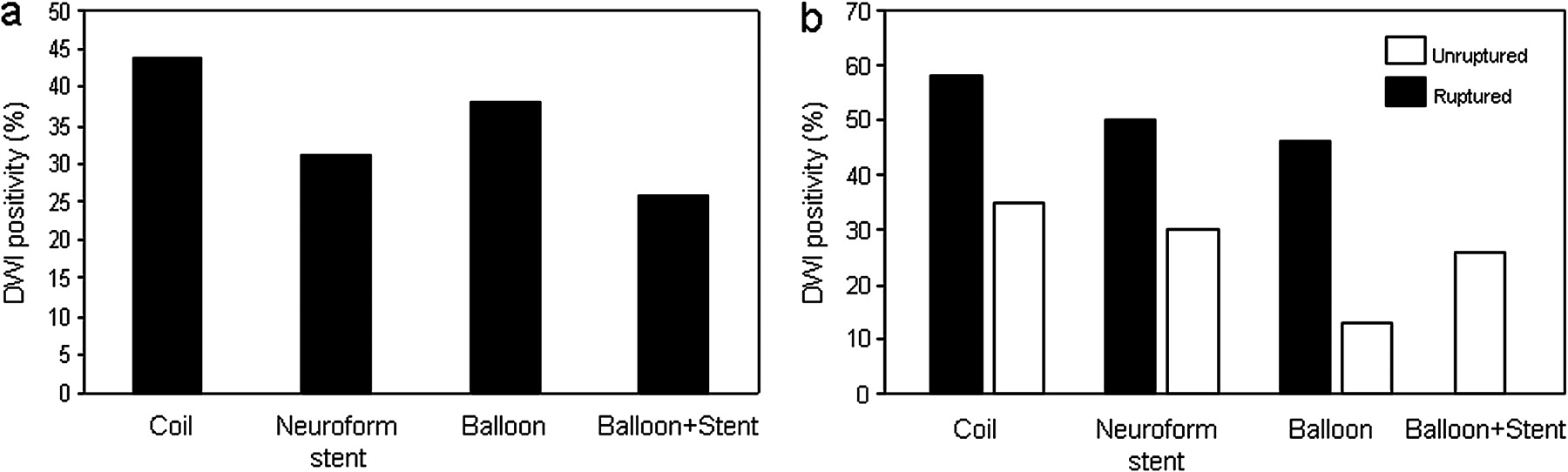
Histogram demonstrating the percentage of diffusion weighted magnetic resonance imaging (DWI) lesions regardless of (A), or based on (B) the aneurysm status compared with the type of procedure applied.
DWI abnormalities were independent of anatomic location. In younger (≤60) patients with unruptured aneurysms, the procedures with adjunctive techniques were associated with DWI hits 20% (n=6), 18% (n=3), and 18% (n=4) in groups of Neuroform, balloon remodeling, or both techniques, respectively, each of which was statistically significant when independently compared with 54% (n=11) in simple coiling procedures. However, there was no difference between any of the treatment groups for the patients >60 years of age (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histogram demonstrating the percentage of diffusion weighted magnetic resonance imaging (DWI) lesions in patients above or below the age of 60, compared with the type of procedure applied. Patients aged ≤60 had significantly lower DWI lesions when they received any type of adjunct technique. Above 60, the type of procedure did not matter.
Discussion
The endovascular treatment of complex cerebral aneurysms can be technically challenging. Those lesions which are not amenable to simple coiling procedures can now be treated using one of several adjunctive techniques such as balloon remodeling and stenting. While these advanced techniques may facilitate aneurysm treatment, some have hypothesized that the use of these adjunctive devices may result in a higher rate of procedural thromboembolic complications.3–12 In this study, we quantified the incidence of peri-procedural cerebral ischemic lesions following aneurysm coil embolization using post-procedural MR diffusion imaging.
Overall frequency
The widespread and routine application of post-procedural MR imaging after coil embolization has made us aware that clinically silent thromboembolic phenomena occur in up to one-third of cases,13 14 although they are not considered thromboembolic complications. The overall frequency of DWI abnormalities (36%) in this study was consistent with that reported previously in the literature.13
Aneurysm status: ruptured versus unruptured
In our study, rupture status was the main independent predictor of peri-procedural DWI abnormalities. Our results were in agreement with those reported by Brooks et al.15 They also reported higher rates of diffusion lesions in patients with SAH compared with those without SAH regardless of the technique used. Similarly, Hadeishi et al demonstrated multifocal cortical ischemic lesions due to microcirculatory disturbances in SAH.16 Vasospasm and hypercoagulability have also been proposed to explain the increased incidence of thromboembolic events in SAH.17 18 In another study, levels of the thrombin–antithrombin complex were found to be elevated.19 These studies strongly suggested the activation of coagulation cascades, thus making the patients with SAH more prone to thromboembolic events.
Adjunctive techniques
We did not observe any trend toward a higher rate of diffusion lesions when adjunctive devices were used to assist coiling.
Balloon remodeling
Some authors have reported that the balloon remodeling technique is associated with greater occurrence of procedural ischemic events.3 4 20 21 On the other hand, others could not find a significant increase in the diffusion lesion rates compared with conventional coiling,22–24 or could even demonstrate a lower rate.25 26 Those who failed to suggest the role of adjunctive techniques in thromboembolism mainly cited other factors, including aneurysm size, coil prolapse or dome/neck ratio as important determinants of post-procedural ischemic events.22 24
The differences between the observed rates of diffusion lesions after balloon remodeling are probably due to differences in techniques, which vary widely between operators. While many operators perform balloon remodeling by inflating and deflating the balloon with each coil placement and detachment, the avid balloon remodelers in our series (HHW, DF) typically left the balloon inflated for several (5–10) minutes during the rapid placement and detachment of a series (3–8) of coils. Using this “conglomerate coil mass technique” (Fiorella et al, LINC course, Houston, TX October 2008), the operator can often completely coil the target aneurysm with only one or two balloon inflations over a very short period of time (in comparison with the traditional technique which can require 5–10 balloon inflations and deflations depending on the number of coils placed). This conglomerate technique avoids the constant inflation and deflation of the temporary occlusion balloon, which may contribute to regional vessel wall trauma, substantially increase procedural time, cumulative occlusion time, balloon catheter manipulation and repositioning, and most importantly microemboli formation related to blood product infiltration of the balloon chamber.
By occluding the aneurysm neck with the balloon and placing multiple coils during the initial inflation, the aneurysm is typically well occluded at the time of the first deflation. As such, this technique limits the duration of time that blood is flowing into and out of the aneurysm through a non-occlusive, yet thrombogenic early coil mass (as occurs with a non-balloon-assisted technique or with the balloon-up/balloon-down technique). Furthermore, if the aneurysm can be completely occluded with one or two inflations, this limits the required repositioning of the occlusion balloon, which may drift out of position during each inflation–deflation cycle.
Limitations
Our study has several limitations. Sulcal subarachnoid blood can cause artefacts on DWI mimicking cortical infarcts. Some patients did not undergo MRI within 72 h owing to severe hemodynamic or neurological instability, or non-MRI-compatible implants. We did not grade the volume or number of DWI lesions; at least one lesion was present on imaging. The use of this binary determination as a surrogate marker for procedural safety has some inherent inaccuracy. The study is retrospective, and the data on pre- and post-procedural clinical status were based on chart review.
Conclusion
In this study, peri-procedural thromboembolic phenomena occurred in approximately one-third of all cases. These were threefold more common in the setting of ruptured aneurysms. Adjunctive devices did not increase the rate of ischemic events. On the contrary, there was a trend towards fewer DWI abnormalities in the procedures in which balloon remodeling was employed. This may, in part, be related to the application of the specific remodeling technique with single balloon inflation for multiple coil placement. More defined analysis of this technique is warranted.
Key messages
Use of balloon and stents during endovascular coiling has allowed treatment of a wider range of cerebral aneurysms.
The safety of the procedure using balloon and stents has been of concern, particularly as a source of thromboembolism during the procedure.
A large series of aneurysm embolizations with routine post-coiling MRI scans performed to screen for diffusion abnormalities were reviewed, and although such abnormalities occurred often, their frequency was not increased with the use of these adjuvant devices.
References
Footnotes
Competing interests None.
Ethics approval The database is prospectively collected and approved by the Institutional Review Board of the Cleveland Clinic Foundation, Cleveland, Ohio.
Provenance and peer review Not commissioned; externally peer reviewed.